GASTRIC NEOPLASIA
The incidence of gastric neoplasia in the dog and cat is low, and clinical signs are insidious in onset. Often the only signs observed are inappetence, which can be present for months before other symptoms develop, and subtle weight loss.
Partial obstruction of pyloric outflow and abnormal motility cause progressively worsening vomiting, anorexia, and weight loss. Ulceration and chronic blood loss causes hematemesis and melena. Gastric neoplasia is summarized here. A more detailed discussion is included in Chapter 11.Adenocarcinoma is the most common gastric malignancy in dogs, followed by lymphosarcoma, leiomyosarcoma, fibroma, squamous cell carcinoma, and plasmacytoma. Adenocarcinoma occurs more frequently in males, with an average age of 8 years at the time of diagnosis. Lymphosarcoma is the most common gastric tumor of cats but does not have breed or gender predisposition. Diagnosis of gastric tumors is based on radiographic, endoscopic, or surgical findings. Contrast radiographs may reveal a thickened and ulcerated gastric wall. Endoscopic findings often reveal discolored and thickened mucosa, raised plaques with large central ulceration and thick raised margins (Figure 5-9; see color plate), or polypoid lesions. Diffuse

Figure 5-9 Malignant gastric ulcer located on the incisura angularis (1 to 3 o’clock position in the field of view) in a 13-year-old weimaraner with a 2-month history of chronic vomiting and weight loss. The dog had hypochromic microcytic anemia. The raised edges and central crater of the ulcer were very firm and required that multiple biopsy specimens be obtained from each of several sites to ensure adequate depth of tissue was obtained. Histopathologic findings confirmed gastric adenocarcinoma. (See color plate.)
thickening of the gastric wall, referred to as scirrhous carcinoma, also occurs.
More than half of tumors occur in the pyloric antrum, often near the incisura. Lymphosarcomas can appear as raised nodular masses anywhere in the gastric wall (Figure 5-10; see color plate) or as diffuse mucosal thickening, often with erosion or ulceration. Leiomyoma is the most common benign tumor and the second most common gastric tumor in dogs but is rare in cats. Leiomyomas are often asymptomatic unless pyloric outflow is obstructed. Benign polyps appear as pedunculated or polypoid nodules that protrude from the mucosal surface. Their cause is unknown, and they seldom cause problems unless they are large enough to cause delayed gastric emptying.Focal gastric carcinomas are best treated by surgical resection, whereas diffuse or extensive lesions are not usually resectable. Metastasis of carcinomas to lymph nodes, liver, or lungs has often occurred by the time of diagnosis,and adjunctive chemotherapy is not effective in improving survival. Lymphosarcoma is treated with chemotherapy, although the prognosis is guarded. Benign tumors and adenomatous and hyperplastic polyps causing partial outflow

Figure 5-10 Diffuse nodular gastric lymphosarcoma in a 9-year-old beagle with intermittent vomiting of 2 weeks’ duration and weight loss. Clinical signs resolved with chemotherapy (Adriamycin and L-asparaginase). After 6 months of remission, clinical signs reoccurred and the dog was euthanized. (See color plate.)
obstruction can successfully be resected with a good long-term prognosis.
References
Albibi R, McCallum RW: Metoclopramide: pharmacology and clinical application, Ann Intern Med 98:86, 1983.
Allan DA et al.: Hypertonic saline/dextran resuscitation of dogs with experimentally induced gastric dilatation-volvulus shock, Am J Vet Res 52:92,1991.
Allen FJ, Guilford WG: Radiopaque markers: preliminary clinical observations J Vet Intern Med 8:151J, 1984 (abstract).
Arnbjerg J: Gastric emptying time in the dog and cat, JAm Anim Hosp Assoc 28(1):77,1992.
Barber DL, Mahaffey MB:The Stomach. In Thrall DE, ed: Textbook of veterinary diagnostic radiology, ed 3, Philadelphia, 1998,WB Saunders.
Bayerdorffer E et al.: High dose omeprazole treatment combined with amoxicillin eradicates H. pylori, Gastroenterology 102:A38, 1992.
Brockman DJ, Holt DE, Washabau R: Pathogenesis of acute canine gastric dilitation-volvulus syndrome: is there a unifying hypothesis? Compend Contin Educ Pract Vet 22(12):1108, 2000.
Burns J, Fox SM: The use of a barium meal to evaluate total gastric emptying time in the dog, Vet Radiol Ultrasound 27:169, 1986.
Carrig CB, Seawright AA: Mastocytosis with gastrointestinal ulceration in a dog, Aust Vet J 44:503, 1968. Cheville NF: Uremic gastropathy in the dog, Vet Pathol 16:292, 1979.
Couto CG: Gastrointestinal neoplasia in dogs and cats. In Kirk RW, ed: Current veterinary therapy XI, Philadelphia, 1993, WB Saunders.
DeNovo RC, Magne M: Current concepts in the management of Helicobacter gastritis. Proceedings, American College of Veterinary Internal Medicine Forum, Orlando, Fla, 1995.
Dewey CW et al.: Azathioprine therapy for acquired myasthenia gravis in five dogs, J Am Anim Hosp Assoc 35:396, 1999.
DiBartola SP et al.: Clinicopathologic findings resembling hypoadrenocorticism in dogs with primary gastrointestinal disease, J Am Vet Med Assoc 187:60, 1985.
Editorial: antibacterial therapy of Helicobacter pylori- associated peptic ulcer disease: a new strategy, J Clin Gastroenterol 19(1):6, 1994.
Ellison GW: Gastric dilatation volvulus: surgical prevention, Vet Clin North Am Small Anim Pract 23:513, 1993.
Feldman M, Burton ME: Histamine2-receptor antagonists: standard therapy for acid-peptic diseases, N Engl J Med 323:1672, 1990.
Flemstrom G: Gastric and duodenal mucosal bicarbonate secretion. In Johnson LR, ed: Physiology of the gastrointestinal tract, New York, 1987, Raven Press.
Freston JW: Overview of medical therapy of peptic ulcer disease, Gastroenterol Clin North Am 19:121, 1990.
Glickman LT et al.: A prospective study of survival and recurrence following the acute gastric dilatationvolvulus syndrome in 136 dogs, J Am Anim Hosp Assoc 34:253, 1998.
Graham DY: The relationship between nonsteroidal anti-inflammatory drug use and peptic ulcer disease, Gastroenterol Clin North Am 19:171, 1990.
Guilford GW, Strombeck DR: Chronic gastric diseases. In Guilford GW et al., eds: Strombeck' small animalgastroenterology, ed 3, Philadelphia, 1996, WB Saunders.
Guilford WG, Strombeck DR: Gastric structure and function. In Guilford WG et al., eds: Strombeck' small animal gastroenterology, ed 3, Philadelphia, 1996, WB Saunders.
Hall JA, Twedt DC, Burrows CF: Gastric motility in dogs. II. Disorders of gastric motility, Compend Contin Educ Pract Vet 12:247, 1990.
Hall JA et al.: Gastric motility in dogs. I. Normal gastric function, Compend Contin Educ Pract Vet 10(11):1282, 1988.
Handt LK, Fox JG, Dewhrist FD: Helicobacter pylori isolated from the domestic cat: public health implications, Infect Immun 62:2367, 1994.
Hayden DW, Fleischman RW: Scirrhous eosinophilic gastritis in dogs with gastric arteritis, Vet Pathol 14:441, 1977.
Horne WA et al.: Effects of gastric distension-volvulus on coronary blood flow and myocardial oxygen consumption in the dog, Am J Vet Res 46:98, 1985.
Hosgood G: Gastric dilatation-volvulus in dogs,J Am Vet Med Assoc 204:1742, 1994.
Jenkins CC, DeNovo RC: Omeprazole: a potent antiulcer drug, Compend Contin Educ Pract Vet Ed 13:1579,1991.
Johnson SA et al.: The effect of misoprostol on aspirin- induced gastroduodenal lesions in dogs, J Vet Intern Med 9(1):32,1995.
Johnson SE: Fluid therapy for gastrointestinal, pancreatic and hepatic disease. In DiBartola SP, ed: Fluid therapy in small animal practice, Philadelphia, 1992,WB Saunders.
Kim CH, Azpiroz F, Malagelada JR: Characteristics of spontaneous and drug-induced gastric dysrhythmias in a chronic canine model, Gastroenterology 90:421,1986.
Konturek SJ, Pawlik W: Physiology and pharmacology of prostaglandins, Dig Dis Sci 31:6S, 1986.
Lee A et al.: Role of Helicobacter felis in chronic canine gastritis, Vet Pathol 29:487, 1992.
Miller ME, Christenson GC, Evans HE: The digestive system and abdomen. In Anatomy of the dog, Philadelphia, 1964, WB Saunders.
Miyabayshi T, Morgan JP: Gastric emptying in the normal dog, Vet Radiol Ultrasound 25:187, 1984.
Muir WW: Acid-base and electrolyte disturbances in dogs with gastric dilatation-volvulus, J Am Vet Med Assoc 181:229, 1982.
Murray M et al.: Primary gastric neoplasia in the dog: a clinicopathologic study, Vet Rec 91:474, 1972.
Murtaugh RJ et al.: The use of misoprostol for prevention of gastroduodenal hemorrhage and ulceration associated with aspirin therapy, J Vet Intern Med 6(2):129, 1992.
Neiger R, Simpson K: Helicobacter infection in dogs and cats: facts and fiction, J Vet Intern Med 14(2):125, 2000.
Orton EC, Muir WW: Hemodynamics in experimental gastric dilatation-volvulus in dogs, Am J Vet Res 44:1512, 1983.
Patnaik AK, Hurvitz AL, Johnson GV: Canine gastrointestinal neoplasms, Vet Pathol 14:447, 1997.
Pennick DG et al.: Ultrasonographic evaluation of gastrointestinal diseases in small animals, Vet Radiol Ultrasound 31(30):134, 1990.
Rawlings CA et al.: A rapid and strong laparoscopic- assisted gastropexy in dogs, Am J Vet Res 62(6):871, 2001. Robert A: Cytoprotection by prostaglandins, Gastroenterology 77:761, 1979.
Sikes RI et al.: Chronic hypertrophic gastropathy: a review of 16 cases, J Am Anim Hosp Assoc 22:99, 1986.
Silen W, Ito S: Mechanisms for rapid re-epithelialization of the gastric mucosal surface, Ann Rev Physiol 47:217, 1985.
Simpson K et al.: The relationship of Heilcobacter spp. infection to gastric disease in dogs and cats, J Vet Intern Med 14(2):223, 2000.
Skirrow MB: Diseases due to Campylobacter, Helicobacter and related bacteria, J Comp Pathol 111:113, 1994.
Smout AJ, Akkermans LM: Normal and disturbed motility of the gastrointestinal tract, Petersfield, UK, 1992, Wrightson Biomedical.
Sorjonen DC et al.: Effects of dexamethasone and surgical hypotension on the stomach of dogs: clinical, endoscopic, and pathologic evaluations, Am J Vet Res 44:1233, 1983.
Stanton ME, Bright RM: Gastroduodenal ulceration in dogs, J Vet Intern Med 3:238, 1989.
Tarnawski A, Hollander D, Gergely H: The mechanism of protective, therapeutic and prophylactic actions of sucralfate, Scand J Gastroenterol 22(suppl 140):7, 1987.
Twedt DC: Cirrhosis: a consequence of chronic liver disease, Vet Clin North Am 15:151, 1985.
Van den Brom WE, Happe RP: Gastric emptying of a radionuclide-labeled test meal in healthy dogs: a new mathematical analysis and reference values, Am J Vet Res 47:2170, 1986.
Wallace JL, Bell CJ: Gastroduodenal mucosal defense, Curr Opin Gastroenterol 8:911, 1992.
Wallmark B, Lorentzon P, Lorsson H:The mechanism of action of omeprazole: a survey of its inhibitory actions in vitro, Scand J Gastroenterol 20(suppl 108):37, 1985.
Walter MC, Matthiesen DT: Acquired antral pyloric hypertrophy in the dog, Vet Clin North Am 23:547, 1993.
Zerbe CA et al.: Pancreatic polypeptide and insulinsecreting tumor in a dog with duodenal ulcers and hypertrophic gastritis, J Vet Intern Med 3:178, 1989.
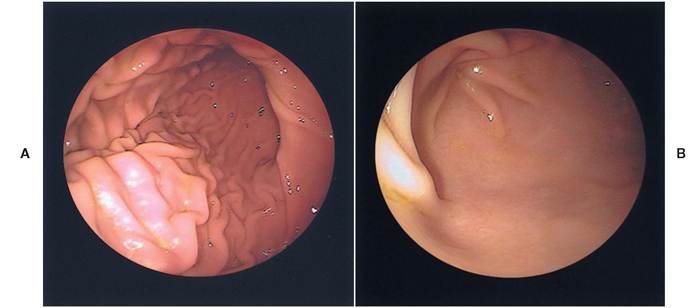
Figure 5-4 Normal stomach. A, Endoscopic appearance of a normal stomach.The smooth, pale-pink rugal folds of the greater curvature of the gastric body gradually become more linear distally at the junction with the pyloric antrum.The incisura angularis appears as a curved fold located at the 12 to 3 o'clock position. B, Appearance of a normal pyloric antrum (foreground) and pylorus (upper left).The antral mucosa is smooth, pale pink, and without rugal folds.The closed pyloric orifice is located at the center of the converging mucosal folds.

Figure 5-5 NSAID-induced ulcerative gastritis. Diffuse ulcerative gastritis in a 9-year-old German shepherd-mix with degenerative joint disease.The dog was being treated with aspirin (325 mg 2 times a day). Treatment began 2 months before presentation, but clinical signs of weakness, vomiting, melena caused by acute gastrointestinal blood loss, and anemia did not occur until the day of presentation.
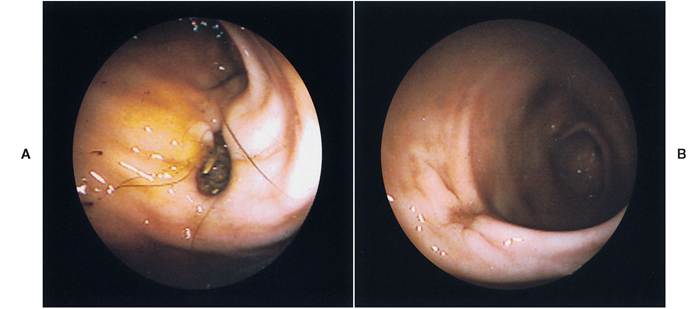
FIGURE 5-6 NSAID-induced gastric ulcer. A, Gastric ulcer in pyloric antrum of a 5-year-old Welsh corgi that had been treated for back pain with ibuprofen (325 mg every day for 5 days).The dog had an acute onset of vomiting and an episode of melena on the day of presentation. B, Healing gastric ulcer in the same patient after 7 days of treatment with omeprazole (0.3 mg/lb every day).
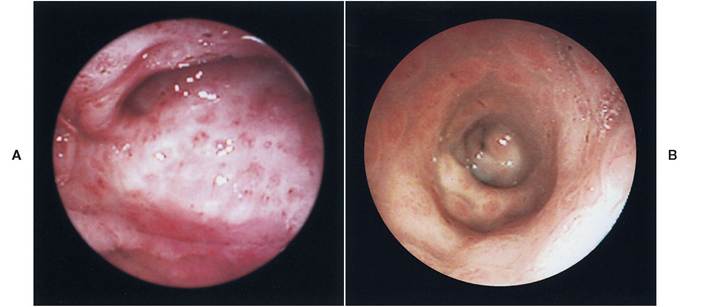
Figure 5-7 Helicobacter gastritis. A, Endoscopic view of the gastric body and incisura angularis in a 3-year-old English bulldog with chronic intermittent vomiting. Raised nodules, some with a central reddened craterlike appearance, were present throughout the body and antrum. B, Endoscopic view of the pyloric antrum from the same dog showing a diffusely nodular mucosa.The pylorus is seen distally in the center of the image. Biopsy revealed the nodules to be accumulations of lymphocytes. Urease-positive Helicobacter organisms were present on the surface musosa and extending into the gastric pits. Clinical signs resolved after treatment with omeprazole (0.3 mg/lb every day) in combination with amoxicillin (10 mg/lb 2 times a day) for 14 days.
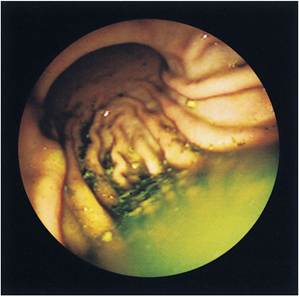
FIGURE 5-8 Gastric retention of food particles and bile-colored fluid in a 12-year-old miniature poodle with clinical signs of intermittent vomiting, regurgitation, inappetence, and bloating.The dog had no food or water for 14 hours before endoscopy. Results of gastric mucosal biopsies were normal, and the dog was diagnosed with primary (idiopathic) gastric motility disorder. Clinical signs improved, but did not resolve, when the dog was treated with cisapride and dietary management (small meals, fat- restricted food).

FIGURE 5-9 Malignant gastric ulcer located on the incisura angularis (1 to 3 o'clock position in the field of view) in a 13-year-old Weimaraner with a 2-month history of chronic vomiting and weight loss.The dog had hypochromic microcytic anemia. The raised edges and central crater of the ulcer were very firm and required that multiple biopsy specimens be obtained from each of several sites to ensure adequate depth of tissue was obtained. Histopathologic findings confirmed gastric adenocarcinoma.
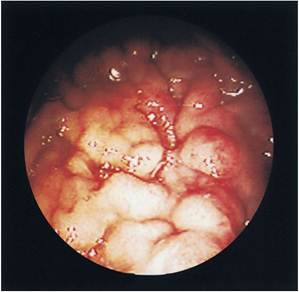
Figure 5-10 Diffuse nodular gastric lymphosarcoma in a 9-year-old beagle with intermittent vomiting of 2 weeks' duration and weight loss. Clinical signs resolved with chemotherapy (Adriamycin and L-Asparaginase). After 6 months of remission, clinical signs reoccurred and the dog was euthanized.