gastric Dilatationvolvulus syndrome
bassets, bulldogs, miniature poodles, dachshunds, and Pekingese are affected. GDV is rare in cats. GDV occurs in animals ranging in age from 2 months to 15 years, with a mean of about 6 years.
No sex predilection has been identified.No single cause of GDV has been identified; however, several risk factors are thought to be of importance for the development of this condition. Deep-chested breeds of dogs appear to have an increased potential for rotational instability of the stomach, in part because of laxity of hepatoduodenal and hepatogastric ligaments. Large-volume intake of food and water causes chronic gastric distention that can potentially impair gastric emptying. Exercise with a distended stomach, particularly in deep-chested dogs, might subsequently cause the stomach to become displaced and result in volvulus. Dietary composition, particularly feeding dry-food diets, has also been suggested as a contributing factor to GDV; however, a direct relationship has not been established. The incidence of GDV was reported to decline when dry food was dampened before feeding, presumably preventing swelling of dry food with water in the stomach. Aerophagia from rapid eating, hyperventilation, and esophageal motility abnormalities have also been associated with recurrent GDV. Impaired eructation may result from an anatomically or functionally abnormal gastroesophageal junction (GEJ) in deep-chested dogs. The oblique angle of the GEJ may become exaggerated, especially if the stomach is distended following a large meal, preventing normal eructation.
Pathophysiology of Gastric Dilatation-Volvulus
GDV traps ingesta, fluid, and gas in the stomach, which rapidly causes extreme increase of intragas- tric pressure. A cascade of life-threatening effects develops that, if not corrected rapidly and aggressively, will cause death. The most immediate effect is impedance of gastric blood flow by increased intragastric pressure, gastric wall edema, vasoconstriction, and thrombosis.
Gastric ulceration, necrosis, and perforation develop rapidly. As the stomach enlarges, respiratory tidal volume and cardiac venous return from the viscera decrease, resulting in impaired respiration, acidosis, and decreased cardiac output. Malposition of the spleen results in splenic congestion, thrombosis, and necrosis. Ischemic viscera release endotoxins that further contribute to hepatic, renal, pancreatic, and cardiac damage.Vascular collapse, disseminated intravascular coagulation (DIC), and sepsis occur. Treatment by gastric deflation and derotation and by the rapid administration of fluids, although very necessary, can have further detrimental effects on the patient. Reperfusion injury and release of endotoxins and cardiodepressant factors, hemodilution, and metabolic acidosis further contribute to metabolic dysfunction and cardiovascular compromise.
The metabolic consequences of GDV are variable but can be severe, depending on the duration of the problem. Acid-base and electrolyte imbalances may initially be absent but usually develop during treatment. Frequent monitoring of these parameters is necessary until the patient is stabilized. Metabolic acidosis occurs commonly in the GDV patient from decreased circulating blood volume, arterial hypoxemia, and lactic acidosis. Metabolic alkalosis, caused by fluid sequestration in the stomach and by loss of gastric H+, Cl-, and K+, occurs less frequently. Hyperventilation can cause respiratory alkalosis, whereas hypoventilation from gastric distention can interfere with diaphragmatic function and cause respiratory acidosis. Electrolyte abnormalities occur less frequently than acid-base imbalances, with hypokalemia being the most common.
Presumptive diagnosis of GDV is made on the basis of clinical findings and is confirmed by radiographic findings and gastric decompression. Clinical features of GDV are listed in Table 5-9. The most characteristic clinical signs are an acute onset of retching, but without vomiting, rapidly developing abdominal distention and tympany, and depression.
Some animals are reluctant to stand, whereas others are recumbent. Rapid and weak pulses, prolonged capillary refill time, and pale, congested, or cyanotic mucous membranes are indicative of cardiovascular failure. Cardiac arrhythmia is usually present or develops soon after presentation. Arrhythmias are usually ventricular in origin and range from intermittent ventricular premature conductions to ventricular tachycardia; supraventricular arrhythmias such as atrial fibrillation occur occasionally.Radiographs taken following initiation of fluid therapy and decompression are necessary to determine if volvulus is present. Radiographic determination of the location of the pylorus is the key feature to differentiate gastric dilation from gastric volvulus. This is best accomplished by comparing left and right lateral recumbent views (see Figure 5-2). Gastric volvulus usually results in displacement of the pylorus dorsally and to the left, creating a shelflike partition of soft tissue that appears to compartmentalize the stomach. With the pylorus shifted to the left and the patient in left lateral recumbency, the pylorus fills with fluid and gas fills the rest of the stomach. However, when the patient
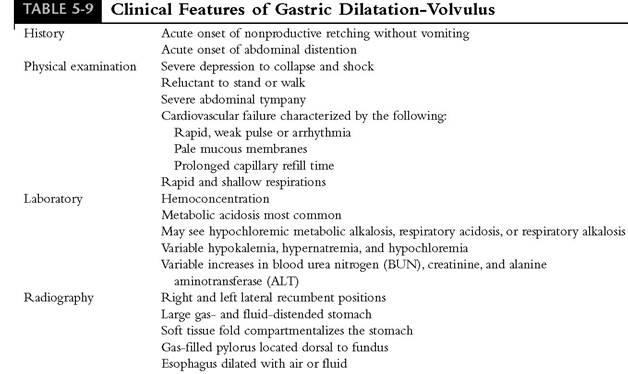
is in right recumbency, gas fills the pyloric portion and fluid shifts to the fundus or body of the stomach. The finding that the pylorus fills with fluid when in the left lateral recumbent position and fills with gas when in the right lateral recumbent position indicates that the pylorus has rotated to the left. The presence of abdominal fluid is suggestive of peritonitis or hemorrhage, and air in the abdominal space indicates that perforation has occurred. Megaesophagus is a common finding.
Treatment
Successful treatment begins with rapid fluid therapy and gastric decompression, followed by surgical repositioning of the stomach and gastropexy. Concurrent therapy for electrolyte imbalances, arrhythmias, and DIC are necessary.
Box 5-9 provides guidelines for the emergency treatment of the patient with GDV.Initial Stabilization
Fluid therapy should be started immediately. A balanced crystalloid such as lactated Ringer's solution should be given intravenously (25 ml/lb) within the first 15 minutes to reestablish cardiac output; an additional 25 ml/lb is then given over the next 30 to 45 minutes. After this initial bolus, a colloid such as hetastarch should be given at a dose of 5 ml/lb as a slow intravenous bolus over
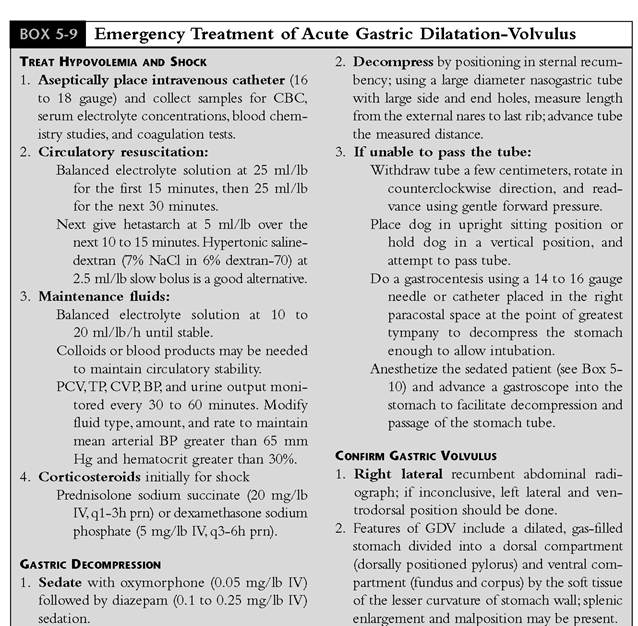
CBC, Complete blood count; PCV, packed cell volume; TPr total plasma protein; CVPr central venous pressure; BPr blood pressure; IV, intravenously; prn, as needed; GDV, gastric dilatation-volvulus.
10 to 15 minutes. Depending on patient response, crystalloid fluid should be resumed at a rate of 10 to 20 ml/lb/hr for the next 2 hours and then decreased to 5 to 10 ml/lb/hr. Pulse quality, capillary refill, central venous pressure, and urinary output should be used as a guide for continued fluid needs. The packed cell volume and plasma total protein concentration should be monitored hourly to avoid hemodilution (total plasma protein concentration should not decrease to less than
3.5 g/dl). Following gastric decompression, the fluid rate can usually be decreased to 5 ml/lb/hr, depending on patient stability. Hetastarch can be repeated within 6 to 12 hours if needed to maintain perfusion. If the plasma protein concentration decreases to less than 3.5 g/dl, a plasma transfusion (10 ml/lb) should be given.
Gastric decompression must be accomplished immediately, occurring as soon as intravenous fluid therapy has begun. Decompression is achieved either by passage of a stomach tube or by gastric trocarization. Trocarization is easier and better tolerated by the patient than gastric intubation; rarely does it cause peritonitis. A 16-gauge 2-inch needle or 14- to 16-gauge over-the-needle catheter is used to trocarize the stomach on the left side at the site of maximal distention.
Partial decompression in this manner often facilitates passage of a large-bore orogastric tube for more complete decompression and for gastric lavage. Once a gastric tube is passed, gastric contents should be removed. If possible, the tube should be left in place while radiographs are taken. If the stomach tube is difficult to pass, attempts should be made to pass the tube while holding the patient in an upright or sitting position. Gently shaking the patient while in the upright position may help. Forcing the tube can cause esophageal or gastric perforation. Inability to pass the tube does not necessarily mean that volvulus is present, nor does the ability to pass the tube mean that volvulus is not present. Gastric decompression can also be achieved by gastrostomy, usually done under sedation and local anesthesia. This is a temporary procedure that fixes the stomach caudal to the right costal arch but does not return the stomach to normal position. It is indicated for patient stabilization if a gastric tube cannot be placed or if the patient needs several days of stabilization before surgical repositioning and gastropexy. As an alternative, gastric decompression can be done using an endoscope if passage of an orogastric tube has not been successful. The patient must be anesthetized for this procedure; either mask induction using an inhalant anesthetic or use of a short-acting injectable anesthetic is sufficient. Once decompression has been achieved, an oral-gastric tube can usually be placed to facilitate ongoing patient stabilization.Surgical Correction
As soon as the clinical condition has been stabilized, surgery should be done to reposition and stabilize the stomach (Box 5-10). The optimal time for surgery to occur is variable, depending on patient condition and response to initial therapy. In general, surgery should not be delayed beyond the initial period of time required for stabilization. If gastric contents are noted to contain digested blood suggestive of gastric ulceration and/or necrosis, if there is radiographic evidence of perforation or peritonitis, if decompression cannot be achieved, or if decompression is difficult to maintain, surgery should not be delayed for more than 1 or 2 hours.
If the patient responds well to initial therapy and decompression is sustained, surgery can be delayed for 12 to 24 hours if necessary. In this circumstance decompression must be maintained by nasogastric or pharyngostomy tubes, gastrostomy, or repeated orogastric intubation. Spontaneous repositioning of the stomach occurs infrequently following decompression. In this circumstance surgery can be delayed or may not be necessary.A gastropexy should be done to prevent recurrence of volvulus. A recent study determined that 55% of dogs that did not have gastropexy following surgery had a recurrence, compared with 4% recurrence for dogs that did have gastropexy. Median survival time was 188 days for dogs not having gas- tropexy, compared with 547 days for dogs that did have a gastropexy. Several types of gastropexy done through laparotomy have been described and include incisional gastropexy, circumcostal gas- tropexy, belt-loop gastropexy, and tube gastropexy. The benefit of doing a prophylactic gastropexy to prevent GDV in a dog that is conformationally or genetically predisposed has not been scientifically proven. It is logical, however, that gastropexy would be of benefit to prevent a first episode of GDV in such patients, as well as for patients in which an episode of GDV was managed medically. A rapid laparoscopic gastropexy technique that provides a strong fibrous adhesion between the stomach and abdominal wall has recently been described that could be used for this purpose, thereby eliminating the need for laparotomy.
BOX 5-10
Surgical Correction of Volvulus
1. Anesthetic induction: Repeat intravenous oxymorphone-diazepam combination used for sedation (see Box 5-9).
Lidocaine (1 mg/lb IV) to facilitate intubation and decrease cardiac arrhythmia.
2. Anesthetic maintenance: Halothane, isoflurane, or sevoflurane and oxygen; nitrous oxide should not be used until permanent gastric decompression is achieved.
3. Monitor continuous ECG, BP, and urine output. Maintain mean arterial BP greater than 65 mm Hg and a urine output greater than 1 ml/lb/hr.
4. Reposition stomach, and evaluate stomach and spleen for vascular compromise; remove necrotic portions. A gastropexy should then be performed to prevent recurrence of the volvulus. Basic details are given below; refer to surgical text for description of surgical procedure.
Ventral midline laparotomy incision; an omentum-covered stomach is usually the first structure visible when a clockwise volvulus has occurred.
Decompress stomach by gastrocentesis or by orogastric intubation.
Retract pylorus in the counterclockwise direction; downward pressure on the right side of the visible portion of stomach will facilitate repositioning of the stomach and spleen.
Examine stomach and spleen for signs of irreversible vascular compromise. Palpate gastric and splenic vessels for pulse.
If organs look grossly normal, lavage stomach with warm water via orogas- tric tube.
Ligate sites of active hemorrhage; hemoperitoneum usually occurs from avulsion of short gastric branches of splenic arteries.
If gastric serosal surface is dark purple to green-black after 10 minutes of normal gastric position, irreversible ischemic damage has likely occurred and resection of that portion of stomach should be performed.
5. Gastropexy should then be performed to prevent recurrence of the volvulus. Refer to surgical texts for detailed description of various procedures.
IV, Intravenously; ECG, electrocardiogram; BPr blood pressure.
Medical Management (Box 5-11)
Antibiotics should be given to dogs with GDV because shock, mucosal damage, and portal hypertension predispose to sepsis. Antibiotics should be effective against gram-positive, gram-negative, and anaerobic organisms. A combination of ampicillin (10 mg/lb intravenously) and enrofloxacin (2.5 mg/lb intramuscularly) is a good choice. Second-generation cephalosporins (e.g., cefoxitin 10 mg/lb every 8 hours intravenously) or trimethroprim-sulfa antibiotics are reasonable alternatives. Corticosteroids may be beneficial for the initial management of shock to improve capillary blood flow, to decrease capillary permeability, to reduce intestinal absorption of endotoxin, and to inhibit tissue-damaging phospholipases. Shortterm, high-dose therapy is recommended; prednisolone sodium succinate (20 mg/lb intravenously, given every 1 to 3 hours as needed) or dexamethasone sodium phosphate (5 mg/lb intravenously, given every 3 to 6 hours as needed) is recommended to treat shock. H2-receptor antagonists can be given to help diminish gastric ulceration. This therapy can be started during initial therapy and continued for 7 to 10 days. If gastric mucosal damage has been severe, omeprazole should be used as soon as oral medication can be tolerated because it is a more potent gastric antisecretory drug.
Management of Complications
Cardiac arrhythmias, DIC, and GI motility disorders are common complications occurring during the acute and convalescent phases of disease. Cardiac arrhythmias can occur at the time of presentation but may not develop until as long as 72 hours after onset of GDV. Continuous electrocardiographic (ECG) monitoring is required from presentation until the dog is discharged from the hospital. Ventricular premature contractions (VPCs), paroxysmal ventricular contractions, and ventricular tachycardia are common. Correction of acid-base, electrolyte (especially potassium), and fluid balance is the first step in control of arrhythmias. Antiarrhythmic therapy is indicated if ventricular tachycardia with a heart rate of 150 beats
BOX 5-11
Postoperative Treatment of the GDV Patient
1. Monitoring
CBC, serum electrolyte levels, acid-base and coagulation tests every 12 to 24 hours until stable.
Pulse, respiration, and temperature, blood pressure, urine production, and continuous ECG monitoring are necessary to detect hypoperfusion, electrolyte and acid-base imbalances, infection, DIC, and aspiration pneumonia.
2. Maintain Perfusion
Fluid therapy with a balanced electrolyte solution at a rate of 3 to 5 ml/lb/hr for 24 hours.
If PCV and TP are low and the patient is hypotensive, blood products or colloids should be given to correct the deficits.
If perfusion is good and the patient is stable 24 hours postoperatively, IV fluids can be decreased to 2 ml/lb/hr for the next 24 hours.
If the patient is stable, small amounts of water and food can be offered 48 to 72 hours postoperatively.
3. Analgesia
Systemic opioids such as morphine at 0.2 mg/lb IM given every 4 to 6 hours for 12 to 24 hours postoperatively will relieve pain and improve recovery.
Butorphanol tartrate at 0.1 mg/lb IV or 0.2 mg/lb IM every 4 to 6 hours can be used as an alternative for mild pain and for longer-term analgesia.
NSAIDs should be avoided because of potential to cause GI ulceration.
4. Treat Cardiac Arrhythmias
Correct acid-base and electrolyte imbalances and fluid deficits.
If cardiac function is poor (hypotension, sustained ventricular tachycardia), attempt should be made to abolish the arrhythmia with lidocaine infusion at a rate of 10 to 20 μg∕lb∕min.
5. Postoperative Complications
Esophagitis, gastric hypomotility, aspiration pneumonia. Metoclopramide is effective in restoring gastric motility, diminishing gastroesophageal reflux, and controlling vomiting.
Ranitidine or omeprazole help reduce gastritis and enhance gastric mucosal healing.
Aspiration pneumonia is treated with broad-spectrum antibiotics and pulmonary therapy with nebulization, coupage, and supplemental oxygen.
DIC is treated with fresh frozen plasma (10 ml/lb) and heparin (100 units/lb every 8 hours) until platelet count and coagulation times begin to normalize.
Local cellulitis and peritonitis around the tube gastropexy site occur from leakage of gastric contents.
If this occurs within 2 to 3 days post- operatively, replace the tube under anesthesia.
If this occurs 5 to 7 days postopera- tively, the tube can usually be left in place.
Thrombosis or avulsion of splenic vessels, or splenic infarction is indication for partial or complete splenectomy. If splenic torsion has occurred, splenectomy should be done before reducing the twist to lessen the release of throm- boemboli and toxins to the circulation.
A three-layer closure of the stomach using polypropylene suture or surgical stapling should be done following partial gastric resection.
CBC, Complete blood count; ECG, electrocardiogram; DIC, disseminated intravascular coagulation; PCV, packed cell volume; TPr total plasma protein; IV, intravenous; IM, intramuscularly; NSAID, nonsteroidal antiinflammatory drug; GI, gastrointestinal.
per minute or greater is present or if multifocal VPCs are occurring. Ventricular arrhythmias are initially managed using lidocaine (1 to 2 mg/lb as a slow intravenous bolus followed by infusion of 25 to 40 μg∕lb∕min). Lidocaine infusion can also be used as an excellent adjunct to other analgesics for the control of postoperative pain. Procainamide is used as a supplement to lidocaine if the arrhythmia is refractory to lidocaine, or as longer-term maintenance therapy (5 to 10 mg/lb intramuscularly or orally every 6 hours). DIC is a frequent complication of GDV and is detected initially by presence of progressively worsening thrombocytopenia and prolonged coagulation times. If DIC is suspected, treatment with plasma (10 ml/lb) in combination with heparin (45 units/lb every 8 hours subcutaneously) should be initiated. Heparin is continued until platelets begin to increase and other coagulation parameters stabilize; plasma transfusions should be repeated if the platelet count continues to decline or if coagulation times become more prolonged. When platelet counts and coagulation times normalize, heparin should be decreased gradually by giving doses every 12 hours for 24 hours and then every 24 hours for the next day to avoid rebound hypercoagulation.
Gastric atony, delayed gastric emptying, and ileus frequently occur following GDV; in most instances these are transient. If intermittent vomiting persists, therapy with promotility drugs (metoclopramide or erythromycin) is helpful to reestablish gastric emptying. Treatment with antisecretory drugs and sucralfate may also be beneficial.
The prognosis for GDV is guarded, especially if gastric damage is severe and requires gastrectomy. Mortality is reported to be from 23% to 60%. Poor prognostic signs at presentation include a pulse rate greater than 180 beats per minute, arrhythmia, cyanotic mucous membranes, prolonged capillary refill time, and severe coagulopathy.