Infectious Causes of Mastitis
Numerous bacterial and mycoplasmal agents have long been associated with caprine mastitis. More recently, retroviral infections have been recognized as an important cause of udder inflammation.
Bacterial Mastitis
Bacteria causing caprine mastitis, with a few exceptions, usually enter the udder through the teat end. Clinical cases occur most commonly in early lactation (Moroni et al. 2005c), as do subclinical infections (McDougall et al. 2014). Control is achieved by udder hygiene during and between milkings.
Organisms and Clinical Syndromes
The clinician cannot expect to identify the organism by the nature of the secretion, but can often make a tentative diagnosis based on herd history (prior probability). Culturing the etiologic agent from the milk or udder tissue is necessary to identify the cause of mastitis. In turn, identifying the organism involved assists the veterinarian and owner in designing future control programs. Organisms are discussed in alphabetical order, because prevalence and importance vary between herds and regions. However, in many areas staphylococci are the predominant species.
Bacillus
Bacillus cereus is a large Gram-positive rod with central and subterminal ellipsoidal spores that causes hemolysis on blood agar. This ubiquitous environmental organism in pure culture has caused toxemia and acute gangrenous mastitis with serosanguineous udder secretions in dairy goats in California (Mavangira et al. 2013). The animals survived, but sloughed the affected half after receiving antibiotic therapy selected by sensitivity testing, as well as fluids and anti-inflammatory agents.
Brucellosis
Brucella melitensis and Brucella abortus can cause a subclinical interstitial lymphoplasmacytic mastitis (Heidrich and Renk 1967). The organism is carried by macrophages to the udder and then to the supramammary lymph node, which may be enlarged (Meador et al.
1989). The number of organisms in the milk and the degree of inflammation in the gland are increased by milk stasis, as when milking or nursing does not occur (Meador and Deyoe 1991). The presence of these organisms is often first suspected when brucellosis is diagnosed as a cause of abortion in the herd (see Chapter 13), or if humans exposed to goats or consuming raw milk products develop undulant or Malta fever (Stiles 1950; Seleem et al. 2010). Serologic testing of the goats is then undertaken, because the milk ring test is not accurate in goat milk (see Chapter 13). Contamination of milk and cheese can also be detected with PCR techniques. Sometimes a clinical mastitis occurs, with palpable nodules in the udder parenchyma and flakes in the secretion (Dubois 1911). The mastitis resolves spontaneously, but the goat should be slaughtered to avoid human infections.Coliforms
Coliforms, including Escherichia coli and Klebsiella spp., occasionally cause clinical mastitis in goats (Adinarayanan and Singh 1968; Lewter et al. 1984). The organisms are Gram-negative, KOH-positive, oxidase-negative rods. Colonies are large, gray or yellow, and moist. E. coli gives off a fecal odor.
Infection appears to be more common in periparturient does. Clinical signs in acute cases include anorexia, fever, and a yellowish or reddish watery secretion with an increased SCC. The affected gland is warm, swollen, and painful. These signs have been reproduced experimentally by intramammary infusion of E. coli endotoxin (Dhondt et al. 1977). Occasionally signs progress to gangrene (Ameh et al. 1994).
These organisms represent “environmental” mastitis. Thus, control involves keeping sleeping areas clean and dry, drying teats thoroughly before milking, and avoiding teat-end injuries. Using postmilking teat dipping does not aid much in controlling coliform infections, because these are initiated between milkings, except when wet udders are milked. Vaccination with a J5 strain provides only partial protection (Aslam et al.
1995).Corynebacterium pseudotuberculosis
Though caseous lymphadenitis is very common in goats, mastitis caused by this disease is relatively rare. However, the organism was found in 7% of 336 milk samples in one Egyptian study (Nabih et al. 2018). Infection of skin wounds on the udder may cause abscessation of the supramammary lymph node, with no involvement of mammary gland tissue. Occasionally, goats develop mastitis or abscesses in the parenchyma of the udder (Addo et al. 1980; Burrell 1981; Schreuder et al. 1990; Nabih et al. 2018). Positive catalase test results distinguish C. pseudotuberculosis from Trueperella pyogenes.
Listeria
It has been suggested that Listeria monocytogenes can cause a subclinical interstitial mastitis, with diagnosis based on isolation of the organism from milk (Sasshofer et al. 1987). A chronic inflammatory lesion with lymphocyte infiltration, alveolar destruction, and fibrosis has been seen in the udder of sheep shedding Listeria in the milk after natural or experimental infection (Tzora et al. 1999). A chronic interstitial mastitis with corpora amylacea has also been documented in the udder of a clinically healthy goat (Addis et al. 2019), and the author (MCS) is aware of another case where several goats were shown to be the source of repeated positive Listeria cultures from the bulk tank, even after haylage was removed from the diet. In Belgium, contamination of cheese made from raw goat milk was traced to a single subclinical shedder in the herd (Delhalle et al. 2012). Listeria are commonly shed in the milk of clinically normal goats during herd outbreaks of listeriosis or immediately after parturition (Loken et al. 1982). Shedding of L. monocytogenes in the milk of goats correlates well with the presence of antibodies against the organism in the milk as detected by an ELISA (Bourry et al. 1997). Listeria ivanovii has been isolated from a mastitic goat in India (Elezebeth et al. 2007). Listeria are more important from a food safety perspective (Pearson and Marth 1990) than as a cause of mastitis in goats.
Mannheimia
Mannheimia (Pasteurella) haemolytica has been isolated only occasionally from goat milk (Schroter 1954; Bagadi and Razig 1976; Manser 1986; Donkin and Boyazoglu 2004), although it is a well-recognized cause of mastitis (including gangrene) of sheep. In an Italian study of 720 goats over an entire lactation, it was responsible for 16% of clinical cases (Moroni et al. 2005c). In Angoras in South Africa, M. haemolytica is reported to be a more frequent cause of acute mastitis than is S. aureus, typically occurring four to six weeks after parturition and seldom being accompanied by gangrenous color changes (Van Tonder 1975). The infection is most likely acquired from suckling kids, since it is a common inhabitant of the upper respiratory tract. The organism is a Gram-negative, oxidase-positive, bipolar rod. Colonies are medium, gray, transparent, and hemolytic on blood agar plates.
Mycobacterium Infections (Tuberculosis)
Mycobacterium bovis, Mycobacterium tuberculosis, and Mycobacterium avium can all be associated with tubercular mastitis in goats (Murray et al. 1921; Davies 1947; Sasshofer et al. 1987). In regions where bovine tuberculosis is common, cows infect goats by the respiratory or alimentary routes (Heidrich and Renk 1967). The udder becomes involved during generalization of the infection to other organs such as lungs, liver, and spleen. Often, the source is infected humans.
The infection is subacute to chronic and manifests itself by slight swelling of the udder and development of firm, caseous or calcified nodules in the parenchyma (Davies 1947; Soliman et al. 1953). Supramammary lymph node enlargement occurs. Antemortem diagnosis is by tuberculin test. Culture requires special media. Affected goats are slaughtered because of the risk they pose to human health.
Pseudomonas
Like Mannheimia, Pseudomonas species are oxidasepositive, Gram-negative rods, but colonies are usually granular and dry and may be a variety of colors. The source is usually contaminated water or teat dips, old pitted inflations, or wet bedding.
If the water system is contaminated, flushing with heavily chlorinated hot water (71 °C∕160 °F or hotter) should kill the Pseudomonas, which are otherwise protected by a biofilm. Cleaning directions for pipeline systems (Dairy Practices Council 2000) are applicable. Paracetic acid can also be used to flush hoses and the water system in the parlor (Yeruham et al. 2005a).In one natural outbreak, systemic signs of illness were so severe that gangrenous staphylococcal mastitis was originally suspected. Only when appropriate antibiotics (based on a sensitivity test) were administered did affected goats survive (Petgen and Martain 1977). In another herd outbreak, 18% of 450 goats were infected and 12.5% developed clinical mastitis due to Pseudomonas aeruginosa. These does were depressed, inappetent, and febrile and the udders were firm, swollen, and painful. Many of these animals developed gangrenous mastitis and 25 died, while the other 57 infected goats were culled because they did not respond to treatment (Yeruham et al. 2005a). In some herds, prolonged infections develop and clinical signs occur periodically.
Goats have been experimentally infected, but inoculation of the udder with large numbers of P. aeruginosa was required; clinical signs varied from mild mastitis to severe, hemorrhagic mastitis with terminal septicemia (Lepper and Matthews 1966).
Burkholderia (Pseudomonas) pseudomallei, the causative agent of melioidosis, is a soil saprophyte found in northern Australia and tropical Asia. Mastitis sometimes occurs, although abscesses are most common in lymph nodes, spleen, and lungs. This may take the form of udder swelling with pus in the milk (Thomas et al. 1988; van der Lugt and Henton 1995). Abscesses in the udder that repeatedly break and drain to the outside also have been observed (Olds and Lewis 1954). The organism has been isolated from macroscopically normal goat milk. Treatment (with tetracycline) is often unsuccessful, and affected goats are usually destroyed because of public health concerns.
Other soil- and water-borne species in this genus (the Burkholderia cepacia complex) have occasionally been isolated from goats with mastitis.Q Fever
Q (Query) fever is caused by the obligate intracellular rickettsial organism Coxiella burnetii. The organism is a common cause of abortion in goats, as discussed in Chapter 13. Cattle, sheep, goats, and wildlife throughout the world may carry the organism, which is then shed heavily in placentas, birth fluids, colostrum, milk, and feces. Shedding of the organism in milk can persist for three months after par- turition/abortion (Caminopetros 1948a). Human infections have been linked to the consumption of raw milk, although more often to inhalation of the organism or contact with placentas and birth fluids. The perceived need to kill C. burnetii was the reason for increasing the milk pasteurization temperature in the United States from 61.7 °C (143 °F) to 62.8 °C (145 °F). Recent authors have questioned the current risk of clinical disease in humans consuming raw milk products (Cerf and Condron 2006; Gale et al. 2015). The diagnosis and control of Q fever are discussed in Chapter 13.
Although the excretion of the organism in goat milk is well documented, little has been written about the development of mastitis in the infected doe. Clinical mastitis has been reported in sheep, which showed high fever, loss of appetite, and a red and edematous, painful udder, with eventual development of a dirty brown malodorous secretion (Martinov 2007). In dairy cattle, presence of the organism (detected by PCR) has been associated with chronic subclinical mastitis and increased SCCs (Barlow et al. 2008). In experimental infection of goats leading to abortion and shedding in the milk, mastitis was not commonly observed histologically (Sanchez et al. 2006).
Staphylococcus aureus
Coagulase-positive (usually hemolytic) staphylococci are a common major pathogen of the goat's udder. In regions free of mycoplasmal mastitis, these organisms are often the most prevalent cause of clinical mastitis in dairy goats. S. aureus isolates from caprine mastitis have been shown to resemble bovine mastitis strains in that most contain surface protein A (that binds to immunoglobin G) and fibronectin binding protein (involved in bacterial adherence and colonization) (Jarp et al. 1989). Most strains produce both alpha hemolysin and beta hemolysin (Roguinsky and Grandemy 1978). Colonies are large on blood agar media and are usually surrounded by a zone of incomplete hemolysis or more than 2 mm of complete hemolysis (Figure 14.10). The organisms are Gram-positive cocci in pairs or clumps and are catalase positive. Although the coagulase test is commonly used to identify S. aureus, Staphylococcus intermedius, and Staphylococcus hyicus (Staphylococcus agnetis) can also be coagulase positive (National Mastitis Council 2017) and are occasionally

Figure 14.10 Zones of complete and partial hemolysis around colonies of Staphylococcus aureus growing on blood agar. Source: Courtesy of Dr. M.C. Smith.
isolated from goat milk (Kalogridou-Vassiliadou 1991; Kyozaire et al. 2005) when full speciation is performed. These organisms are now classified as non-aureus staphylococci.
The infection can be subclinical (identified by culture during herd survey), chronic (decreased production accompanied by induration and abscess formation), or acute (swollen, hot, painful half of the udder, accompanied by systemic illness). The most severe, acute form is gangrenous mastitis, which is described in detail below. These same forms have been reproduced by experimental inoculation of S. aureus into goat udders (Derbyshire 1958a).
As is the case with cows, the organism resides in microabscesses in chronically infected goats and infections are very difficult to cure (Derbyshire 1958b). Transmission to other goats occurs during milking. Animals that are culture positive for S. aureus should be culled to slaughter or milked last. In larger herds with machine milking, a “staph” unit can be identified and used to milk only S. aureus-infected goats. If these animals are retained in the herd, they should certainly be dry treated and then should remain in the “staph string” (the group of infected goats) into the beginning of the next lactation. Intermittent shedding is common, and a single negative culture of a previously infected goat is not proof of a cure. If cultures are repeatedly negative and SCCs remain low, the animal could be returned to the main herd.
Ideally, the milk of infected does should be pasteurized before it is fed to kids. Diarrhea, pneumonia, and death of nursing kids, with isolation of S. aureus from heart blood and abomasal and intestinal contents, have been reported (Paliwal et al. 1977).
Gangrenous Mastitis
Gangrenous mastitis in goats is most frequently due to S. aureus in animals lacking adequate concentrations of antitoxin against the necrotizing alpha-toxin produced by the organism. Clostridial infections have also been implicated, as have coliforms (Renk 1957; Petris 1963) and Bacillus spp. (Mavangira et al. 2013).
The condition usually is restricted to the period of lactation. However, sometimes gangrenous mastitis occurs during the last week of pregnancy, when it often causes loss of the fetuses and death of the doe from toxemia (Petris 1963). Affected goats have poor appetite and a transient fever. In early cases, the skin of the teat or udder floor becomes cool and edematous, and the goat appears lame. A reddish (Figure 14.11) then bluish discoloration of the skin is noted next. The secretion becomes watery and red; gas bubbles may be present and produce a squeaking sound when the teat is stripped. Death may occur within 24 hours. In animals that survive the acute phase, a clear line of

Figure 14.11 Early gangrenous mastitis with edema and erythema of the udder. Staphylococcus aureus was isolated from the milk and a portion of the gland sloughed. Source: Courtesy of Dr. M.C. Smith.
demarcation forms on the udder and the gangrenous portions are sloughed after several weeks or months.
Histologically, there is venous thrombosis, and the initial inflammatory changes are replaced by necrosis and sloughing of epithelial cells (Derbyshire 1958b). This thrombosis is probably responsible for edema of the mammary gland and ventral abdominal wall. The supramammary lymph node is enlarged, edematous, and hemorrhagic.
Because of its dramatic presentation and associated great economic loss, gangrenous mastitis caused by S. aureus is often the most prevalent form of mastitis recognized in herds free of mycoplasmal infections. In one report from Cyprus in 1961, almost 9% of 8000 goats were affected with gangrene (Petris 1963). The average case fatality rate in this study was 40%. The factors that cause some goats to develop gangrene and others to be able to control the infection are not well explained (Rainard et al. 2018).
Non-aureus (PreviouslyCoagulase-Negative) Staphylococci
This classification now includes coagulase-negative organisms, but also coagulase-positive staphylococci that are not S. aureus. In many herd surveys, the most commonly isolated organisms are staphylococci other than S. aureus. As many as 71% of udder halves in a herd have been found to be infected (Sheldrake et al. 1981; Poutrel 1984). In a large California survey (16 herds, 2522 lactating does), coagulasenegative Staphylococcus spp. were isolated from 17.5% of does (East et al. 1987). In four commercial herds in Australia, the prevalence was 13.3% of 896 halves tested (Ryan and Greenwood 1990). In a study in Italy that sampled 305 goats monthly throughout the lactation, 1474 of 4571 udder half samples cultured coagulase-negative staphylococci (Moroni et al. 2005b). In a large longitudinal study of dairy goats in New Zealand, 13.4% of the gland samples yielded coagulase-negative staphylococci (McDougall et al. 2014). Numerous staphylococcal species have been identified, including S. epidermidis, S. intermedius, Staphylococcus caprae, and S. hyicus (Poutrel 1984; Maisi and Riipinen 1988; Maisi 1990b; Kalogridou-Vassiliadou 1991). Many studies have been summarized by Contreras et al. (2003). Because different staphylococcal test systems often result in different species assignments, reported species prevalences in the literature may not be comparable (Burriel and Scott 1998). These infections tend to persist throughout much of the lactation and are more common in older goats (Contreras et al. 1997a; Sanchez et al. 1999) and later lactation. Bilateral infections are common (Moroni et al. 2005b). The organisms commonly reside on the skin or in the environment (Valle et al. 1991; National Mastitis Council 2017).
Some authors regard the coagulase-negative organisms as major pathogens (Dulin et al. 1983), while others see them as minor pathogens or incidental infections (Moroni et al. 2005a). In a study comparing milk production of the udder halves of 25 unilaterally infected goats (Leitner et al. 2004a), production was significantly higher (0.98 kg/ milking) in the uninfected halves compared with the infected halves (0.69 kg/milking). Some authors define an increased cell count to be equivalent to a serious mastitis and then conclude that because some goat milk samples with an increased cell count yield the organism, it must therefore have caused serious mastitis (Hinckley et al. 1985). The economic importance of non-aureus staphylococci remains unclear and may vary with the species. Generally, the practitioner should look further to explain serious illness or marked loss in production, because the coagulase-negative staphylococci are unlikely to be the cause. However, a high prevalence of these bacteria may suggest suboptimal milking procedures that should be addressed (Contreras et al. 2003) or a need to select goats for genetic resistance to mastitis.
Streptococcus agalactiae
Infection with Streptococcus agalactiae has been reported in goats in sporadic or epizootic forms, but occurs less frequently than in cattle. Most reports are in the older literature (Heidrich and Renk 1967) or from India (Mukherjee and Das 1957), New Zealand (McDougall and Anniss 2005), or Brazil (Langoni et al. 2006), although the organism has been found in many surveys in Africa, the Middle East, and Asia. The organism does not appear to be a problem in goats in the United States (White and Hinckley 1999).
The goat is not systemically ill, but induration of the udder and loss of secretory tissue may occur. Streptococcus agalactiae has been associated with severe stromal proliferation and fibrosis in goat udders (Addo 1984). The lesions have been reproduced experimentally (Pattison 1951). Abscess formation does not occur. The disease is transmitted from cow to goat or goat to goat, by milk on the inflations or the hands of the milker. Introduction of the disease to the herd can be avoided by screening bulk tank milk from the herd of origin or culturing the milk of the individual purchased doe before it joins the milking herd. Most isolates are sensitive to penicillin.
Colonies are not sufficiently characteristic in blood agar cultures to permit differentiation from other streptococci (see below), because Streptococcus agalactiae may be accompanied by greening of the medium, beta hemolysis, or no hemolysis. Streptococcus agalactia does not split esculin. The CAMP test is frequently used to make a presumptive diagnosis of Streptococcus agalactiae (Schalm et al. 1971). Erythrocytes sensitized by beta hemolysin from a nearby streak of S. aureus are completely hemolyzed by a factor diffusing into the agar from the S. agalactiae.
Other Streptococci
Streptococci other than S. agalactiae are occasionally the cause of sporadic cases of mastitis of environmental origin (Mallikeswaran and Padmanaban 1991). In one study that followed 720 machine-milked goats over a complete lactation, 16% of the clinical cases of mastitis were ascribed to Streptococcus species, compared with 74% due to Staphylococcus aureus (Moroni et al. 2005c). A herd outbreak of mastitis caused by Streptococcus Zooepidemicus (28 of 50 animals with chronic mastitis) was ascribed to poor hygiene. Clinical signs included udder atrophy, induration, and abscessation (Nesbakken 1975). Outbreaks of Streptococcus Zooepidemicus in three herds in Spain resembled contagious agalactia due to mycoplasma, including the occurrence of septic arthritis, and were controlled with an autogenous vaccine (Ruiz Santa Quiteria et al. 1991). SCCs are elevated, even in subclinically infected goats (Hall and Rycroft 2007). Provision of a clean, dry environment for the goats and assuring that the udder is clean and dry at milking should help to prevent new infections.
Streptococcal species form colonies on blood agar that are smaller than staphylococci, and the bacteria are catalase negative. Some streptococci of environmental origin (and Streptococcus agalactiae) are esculin negative (National Mastitis Council 2017).
Trueperella pyogenes
Trueperella pyogenes was previously classified as Arcanobacterium pyogenes or Actinomyces pyogenes, and formerly as Corynebacterium pyogenes. The organism is non-motile, facultatively anaerobic, catalase negative, and Gram positive, appearing as pleomorphic or coccoid rods. It belongs to the family Actinomycetaceae, in the order Actinomycetales of the class Actinobacteria (Rzewuska et al. 2019). This organism is frequently isolated from udders containing multiple abscesses (Figure 14.12). Teat or udder wounds predispose to the entry and establishment of the infection in the udder. In experimental infections, non-lactating glands are more severely affected than lactating glands (Jain and Sharma 1964). In the chronic stage culling is advisable, although teat (Sasshofer et al. 1987) and udder amputations return the goat to systemic good health if localization in other organs has not occurred. The organism grows slowly on blood agar. Colonies are tiny at 48 hours, but made visible by a narrow zone of clear hemolysis.
Miscellaneous Bacterial and Fungal Organisms
It is conceivable that any pathogenic bacterium introduced into the udder might cause mastitis. For instance, isolation of the environmental organism Serratia is occasionally reported on herd surveys. Based on experience with cattle,

Figure 14.12 Udder abscesses in an aged doe caused by Trueperella pyogenes. The animal was managed by udder amputation. Source: Courtesy of Dr. M.C. Smith.
antibiotic therapy is not helpful, but hygiene of the barn and teat dip should be investigated (National Mastitis Council 2017). If treatment has preceded isolation of an uncommon agent, the possibility of iatrogenic inoculation of the udder cannot be discounted. Miscellaneous organisms isolated from mastitic goat milk and discussed elsewhere in this text include Yersinia pseudotuberculosis (Cappucci et al. 1978; Jones 1982), Nocardia (Dafaalla and Gharib 1958; Bassam and Hasso 1997; Rozear et al. 1998; Maldonado et al. 2004), Cryptococcus neoformans (Pal and Randhawa 1976; Aljaburi and Kalra 1983), and numerous other fungi (Lepper 1964; Pal 1982; Jensen et al. 1996). Fungal mastitis has also been produced experimentally in goats using numerous Candida species and Rhodotorula glutinis. Antibiotic treatment prolonged the disease (Jand and Dhillon 1975). Corynebacterium spp. (Schaeren and Maurer 2006; Hall and Rycroft 2007) and yeasts (McDougall 2000) have been isolated from clinically normal goats. Corynebacterum spp. were isolated from 7.3% of the gland samples from a large survey of dairy goats in New Zealand (McDougall et al. 2014). The isolation of Corynebacterium bovis from dairy cows is usually interpreted as evidence for inadequate teat dipping (National Mastitis Council 2017). Campylobacter spp. and Salmonella spp. are occasionally excreted in goat milk, presumably having entered the udder through the teat in an unhygienic environment, but usually fecal contamination is incriminated when zoonotic infections occur. Sometimes milk cultures are required to identify a carrier animal in the herd (Robinson et al. 2020).
Treatment of Bacterial Mastitis
Although the owner of a valuable or pet goat expects and desires treatment for the doe with mastitis, culling of affected animals is often an economically sound alternative. Culling serves to decrease exposure of other does to contagious organisms and to increase selection pressure for genetic resistance to infection. Culling is also a logical choice when abscesses are found in the udder of a fiberproducing or meat goat during weaning or when selection for rebreeding occurs.
Lactation Treatment with Antibiotics
If treatment is elected, it should begin as soon as clinical signs are noted. Otherwise, additional destruction of milk-secreting tissue may occur or the mastitis may turn gangrenous (Staphylococcus aureus). Lactational treatment of subclinical mastitis detected by culture or somatic cell determination usually is not economically profitable, except possibly for Streptococcus agalactiae, which is uncommon in goats. Milking such animals last is desirable.
Choice OfAntibiotics
The range of antibiotics available for either intramammary or parenteral treatment of mastitis varies from country to country. Practitioners should evaluate the antibiotic sensitivity of isolates relative to drugs that are available, legal, and not prohibitively expensive. Because S. aureus is the most frequent cause of clinical mastitis in many herds, initial treatment (in the absence of sensitivity results) should ideally be with a drug this organism is normally sensitive to; tetracycline and cephapirin are frequently effective in vitro. Resistance to penicillin is common, while ampicillin and amoxicillin have a broader spectrum of efficacy. Some studies have not shown beta lactamase production by goat isolates (Moroni et al. 2005d). Unless the animal is systemically ill, treatment is often limited to intramammary infusion with a full lactating cow tube administered two or three times at 12- or 24-hour intervals.
When extensive swelling or tissue penetration by bacteria such as S. aureus has occurred, parenteral administration of an antibiotic with good bioavailability for five to seven days is recommended (Ziv 1980). Because of pharmacokinetic considerations, some drugs that are administered parenterally do not achieve adequate concentrations in the udder (Ziv and Soback 1989). Gentamicin penetrates the udder poorly, and cephalosporins also do not pass readily from blood to milk. Oxytetracyline and potentiated sulfonamides are broad spectrum and non-toxic, but also have limited or variable penetration. Chloramphenicol has excellent properties for parenteral treatment of mastitis, but is forbidden in many countries. Slow-release formulations (penicillin, tetracycline) are not usually effective in maintaining adequate milk concentrations.
Infusion of the udder on a prescription basis with gentamicin or trimethoprim/sulfadiazine has been recommended for confirmed coliform mastitis (Lewter et al. 1984). Research in cows suggests that gentamicin therapy does not affect severity or duration of E. coli mastitis, and clearance of gentamicin from kidney tissue requires many months (Erskine et al. 1991). The use of this antibiotic, then, is best avoided. Furthermore, infusion of any antibiotic solution other than a commercial mastitis tube is undesirable because of sterility, safety, and residue issues.
The antibacterial and udder penetration properties of several newer agents have been summarized by Ziv and Soback (1989). Florfenicol, enrofloxacin, norfloxacin nicotinate, tiamulin, and doxycycline afford good or excellent udder penetration after parenteral administration. The use of enrofloxacin and other fluoroquinolones in goats is expressly forbidden in the United States.
Owners in the United States wishing to maintain the organic status of their goats will often choose a plant-based
product such as Phyto-Mast™ (Penn Dutch Cow Care, Narvon, PA, USA). One of its active ingredients, thymol, was only detected in the milk at 12hours after treatment with part (5 mL) of a tube per udder half (McPhee et al. 2011). The clearance for the other three herbal components is unknown, and there is minimal evidence for efficacy.
Infusion Techniques
Some commercial bovine infusion tubes have an applicator tip that is too large to be inserted into an average goat's teat. It is currently recognized that full insertion, even in a cow, damages the lining of the streak canal. In addition, bacteria that colonize the keratin lining are forced upward into the teat cistern, thereby predisposing to new infections. Thus, even in the case of a large teat opening, the applicator tip should be inserted only far enough to prevent leakage of the product during infusion. Specially designed 3.5 mm syringe tips such as Opti-Sert™ (Zoetis, Parsippany, NJ, USA) make partial insertion easier. When the teat sphincter is too tight or the doe too uncooperative, a sterile tomcat catheter may be used to infuse the mastitis medicine into the teat. Some authors recommend treating both halves even if only one is clinically affected (Sasshofer et al. 1987).
Teat dipping with a disinfectant before and after infusion is advisable, as is cleansing of the teat end with alcohol. Owners may need instruction in the importance of clean hands (or gloves) and sanitary techniques.
Antibiotic Residue Avoidance
The owner or veterinarian who has treated the lactating goat with antibiotics is left with the question of when the milk will be free of antibiotic residues, in addition to the need to identify treated animals. In one study using commercial lactating cow infusion tubes in the United States, erythromycin, oxytetracycline, penicillin, and cephapirin were administered according to label directions to 10 goats. Antibiotic residues were not detected after the labeled discard periods (36, 96, 60, and 96 hours, respectively), except for one goat that still had detectable penicillin after 72 hours (Long et al. 1984). Another study found that oxytetracycline (426 mg) was still detectable at 108 hours and cloxacillin (200 mg) at 156 hours after last treatment (Hill et al. 1984). A commercial combination product (200 mg amoxicillin trihydrate, 50 mg potassium clavulanate, and 10 mg prednisolone) labeled with a 48-hour withdrawal in dairy cows required 112 hours withholding time to achieve acceptable amoxicillin concentrations in goat milk (Buswell et al. 1989). It seems prudent to at least double the recommended bovine withdrawal period when treating goats. European regulations specify a seven-day withdrawal period for extralabel intramammary treatment of lactating small ruminants (Bergonier et al. 2003). This is not always long enough to avoid residues; emphasis should be placed on good farming practices that avoid the need for antibiotic therapy (Berruga et al. 2016).
Duration of antibiotic residues in healthy goats after intramammary treatment (35 commercially available infusion products) or parenteral treatment (27 injectable products) has been reported by Ziv (1984). Ceftiofur is labeled for systemic use in goats in the United States with zero milk withdrawal, but does not penetrate the udder well. Systemic oxytetracycline is expected to be cleared from goat milk as fast as or faster than cows clear the antibiotic, but a milk discard period of six days has been suggested after high or prolonged dosage (Martin-Jimenez et al. 1997). Duration of penicillin residues in goat milk is variable, especially if given by the subcutaneous route, and testing of the milk is advised (Payne et al. 2006).
As the sensitivity of assays in use increases, it can be expected that the prudent withdrawal period will lengthen. Several residue tests have been shown to detect antibiotic concentrations in goat milk below the tolerance limit set for cow milk in the United States (Zeng et al. 1998); typically no confirmatory testing is done and the producer is presumed to be guilty of supplying milk with an illegal residue. It is also important to remember that detectable concentrations of antibiotics appear in milk from the untreated half (Hill et al. 1984). Even when residue levels are too low to endanger any except the most allergic human consumers, a cultured cheese may fail because of antibiotics in the milk. Ideally, milk from treated does should be tested at a milk plant or laboratory with the most sensitive antibiotic test available; milk with positive test results should not be used for human consumption. Most screening tests are not sensitive enough for detecting quinolones and tetracyclines (Beltran et al. 2015).
False-Positive Inhibitor Tests
Normal goat milk appears to have some antibacterial action. In one study, 24% of pre-antibiotic treatment milk samples from 75 healthy goats showed false-positive Delvotest® (Nelson Jameson, Marshfield, WI, USA) results, and in 11% of the 75 animals the natural inhibitors were heat stable (60 °C∕140 °F for 20 minutes; Ziv 1984). Small zones of inhibition (halos) are sometimes noted with the Bacillus Stearothermophilus disc assay, especially late in lactation, and this naturally attracts the attention of regulatory officials (Hinckley 1991). Iron-binding protein (lactoferrin) in goat milk has been shown to be bacteriostatic for B. Stearothermophilus (Oram and Reiter 1968). Both the bacteriostatic effect and the lactoferrin concentration are increased in dry secretion. Rancidity (lipolysis) is also increased in late lactation, and heat treatment does not affect bacterial inhibition due to fatty acids (Hinckley 1991;
Atherton 1992). The B. Stearothermophilus test may be inappropriate for goat milk (Klima 1980). The Delvotest P culture medium version of the B. Stearothermophilus assay has been shown to produce false-positive results when compared with the disc assay (Zeng et al. 1996). The Penzyme® test (Nelson Jameson) for beta lactam residues has been reported to be sensitive and specific when used on goat milk containing penicillin or cephapirin (Zeng et al. 1996). Another study using eight different test kits and milk from clinically normal goats found all kits, including Penzyme®, to be suitable for screening goat milk when performed according to the manufacturer’s directions, because specificity was at least 0.99 (Contreras et al. 1997b). However, increased SCCs in the milk from untreated animals can result in false-positive tests (Beltran et al. 2015).
Incubating bovine milk samples at warm temperatures, with resulting increase in bacterial numbers and decrease in pH levels, has been shown to cause inhibitory zones in disc assays. Some of these inhibitory zones, like those caused by antibiotics, persisted after raw milk had been heated to 82.2 °C (180 °F) for five minutes (Kosikowski 1963). Thus, improper handling of milk samples may contribute to false-positive residue test reactions.
Non-antibiotic inhibitors in milk may have an importance that transcends regulatory considerations. Residues of disinfectant in milk or iodine originating from excessive dietary levels may interfere with bacterial acidification necessary for cultured products (Le Jaouen 1987).
Supportive Therapy for Mastitis
Frequent stripping, which serves to remove both bacteria and toxins, is beneficial. Oxytocin (5 units) and hot compresses assist in achieving milk letdown from a painful gland. Infection or starvation of kids and spread to other does are potential risks if kids are left on the doe to aid in removal of secretions from the udder.
Anti-inflammatory agents such as intravenous, subcutaneous, or oral flunixin meglumine (1 mg/kg once or twice daily) or corticosteroids (dexamethasone 0.44 mg/kg single dose) are frequently administered to animals with signs of discomfort or toxemia. In an experimental intramammary E. coli challenge, goats treated with anti-inflammatory agents showed some improvement in clinical signs without any adverse effects on bacterial clearance (Anderson et al. 1991). In a clinical trial, intramuscular flunixin meglumine at approximately 2.5 mg/kg once daily for two treatments resulted in more rapid resolution of clinical signs compared with control goats receiving the same intramammary antibiotic but no anti-inflammatory drug (Mavrogianni et al. 2004). Phenylbutazone should be avoided in goats to be used for meat or milk and is explicitly forbidden in some countries. Intravenous fluids may be indicated in systemically ill animals. If the goat is still ambulatory, oral fluids, such as commercial electrolyte products, can be substituted and are less expensive. Oral or subcutaneous calcium might be administered to anorexic animals. Systemic antibiotics are commonly administered when the mastitis is severe or chronic.
Treatment of Gangrenous Mastitis
When a reddish udder secretion is accompanied by blue discoloration and coolness of the udder skin, the severity of the mastitis warrants intensive therapy (or euthanasia) and, usually, a poor prognosis for return to function.
Medical Management
In the early stages, when the affected gland is warmer than normal and painful and the secretion is blood tinged, successful medical treatment has been reported. Even when signs of gangrene were unequivocal (i.e., coolness, pitting edema, loss of skin sensation, and a watery red secretion), complete recovery was reported in 91% of 81 goats in the Sudan (Abu-Samra et al. 1988). Oxytetracycline systemically (5 mg/kg intravenously) and intramammary (426 mg daily) for five days was used in the Sudanese study, but intramammary cephapirin also seems to be a rational choice. The secretion was drained with a sterile teat cannula. In addition, a diuretic (40 mg furosemide) daily for five days and topical treatment of the udder with an antiseptic cream were used.
Most authors do not claim such successful results with less intensive medical treatment. For instance, in a study from Cyprus in which 9% of 8000 goats suffered from gangrenous mastitis, in no case was there complete recovery of the udder (Petris 1963). Sloughing of the affected udder half is expected to occur one to two months later (Mavangira et al. 2013).
Mastectomy
Surgical removal of one half or of the entire udder is sometimes performed.
Indications and Reservations Amputation of the udder can be a life-saving procedure if the goat is very toxic with gangrenous mastitis. Udder amputation avoids the unhygienic and unpleasant process of sloughing of necrotic tissue (Abu-Samra et al. 1988). Another candidate for the surgery is the goat that has chronic abscesses in the udder and is in poor body condition; udder amputation may result in a return to good health (Cable et al. 2004).
The reason for saving the goat’s life should be discussed with the owner in advance. Is it a pet or a commercial animal? Salvaging an animal for later slaughter in societies where meat from sick animals is not consumed is justification for udder amputation and also for use of inexpensive surgery techniques. Salvaging the goat for continued breeding is hard to justify, unless the mastitis was clearly the result of an injury and cannot be attributed to a decreased genetic resistance. In herds participating in a Swedish mastitis control program, goats with milk cultures that were positive for S. aureus were slaughtered because of the poor prognosis for microbiologic cure and the danger to people consuming unpasteurized goat milk products. Therefore, mastitis has become relatively rare in these herds (Danielsson et al. 1980). Owners become more careful and goats are selected for genetic resistance. Lack of colostrum and periparturient complications in goats that have undergone a mastectomy are additional reasons for not breeding these animals (Matthews 2016).
Anesthesia A variety of anesthetic regimens have been used successfully. The choice depends on the previous experience of the veterinarian and the drugs and facilities available. In the United States, gas anesthesia or a keta- mine/xylazine combination is commonly selected. Intravenous barbiturates and lumbosacral spinal anesthesia are other possibilities. These methods are discussed in detail in Chapter 17. Antibiotic therapy (penicillin or cefti- ofur) and anti-inflammatory therapy should be begun before surgery commences and intravenous fluids should be administered during surgery.
Surgical Techniques See Otte 1958; Kerr and Wallace 1978; Anderson et al. 2002; Cable et al. 2004: Matthews 2016; Hermida et al. 2021. The animal should be fasted for 24 hours before surgery if possible. The goat is placed in lateral recumbency with the upper hindlimb pulled cau- dally or in dorsal recumbency, depending on whether one or both glands are to be removed. A clamp attached to the teat simplifies manipulation of the udder during surgery. After skin preparation, an elliptical incision is made around the base of the teat or udder, leaving as much skin as possible to provide for closure. Alternatively, a clover-leaf skin incision can be used, for better exposure of the blood vessels (Plummer and Plummer 2012). Blunt dissection is used to separate the gland from the skin and, if only half is to be removed, from the median suspensory ligament. The supramammary lymph node (caudal and dorsal to the gland) should also be removed. Major vessels that need to be ligated include first the external pudendal artery at the inguinal ring (double ligate), and then the external pudendal vein, the subcutaneous abdominal vein, and the perineal vein (Figure 14.13). Dead space is closed with subcutaneous sutures and drains are placed if deemed necessary. A potential blood donor and equipment for administering a blood transfusion should be located before the surgery is undertaken. Tetanus prophylaxis should be assured. Survival is good after elective surgery, but complications include surgical site infection, dehiscence of the skin wound, and seroma formation (Hermida et al. 2021).
Other Alternatives to Udder Amputation The external pudendal artery and vein can be triple ligated under light sedation and local anesthesia if the goat with gangrenous mastitis is not a good anesthetic or surgical candidate, with the vessels severed distal to the second ligature (Plummer and Plummer 2012). This will greatly decrease the absorption of toxins. Amputation of the teat under tranquiliza- tion and local anesthesia has been used in goats to improve drainage of purulent or gangrenous infections of the udder. The base of the teat is clamped and the teat is amputated in its proximal one-third, distal to the large vessels. Hemostasis is achieved with cautery or ligation after removing the clamp (Sasshofer et al. 1987).
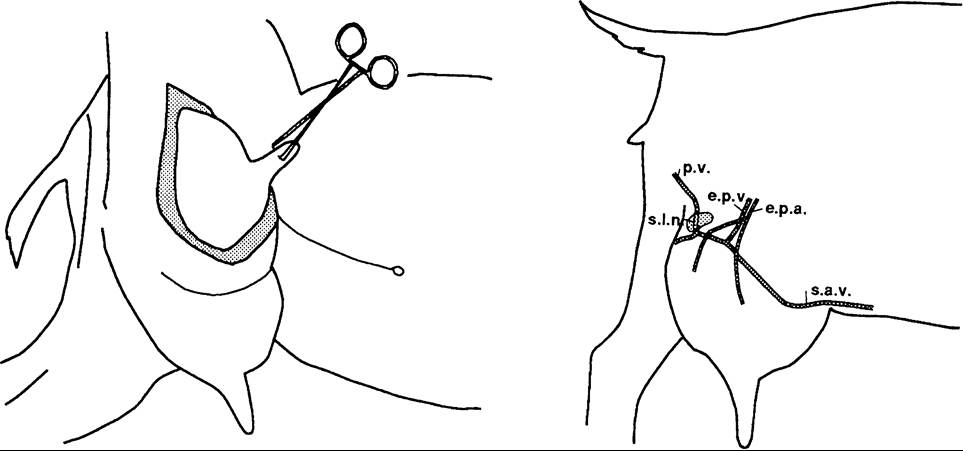
Figure 14.13 Initial skin incision and vessels to be ligated during udder amputation. e.p.a., external pudendal (mammary) artery; e.p.v., external pudendal vein; p.v., perineal vein; s.a.v., subcutaneous abdominal vein; s.l.n.= supramammary lymph node.
In selected cases, when surgery is not an option, the gangrenous gland can be infused once with 60 mL of 5-10% formalin (normally used for fixation of pathologic specimens). The formalin kills organisms and binds toxins produced by either the infectious agent or the necrosis of tissue. The gland thus treated does not return to production, but the doe's life may be preserved. In cattle, both 2% chlorhexidine and 5% povidone iodine have been used to cause cessation of lactation in chronically infected glands (Smith et al. 2005); a dose of 10 mL might be appropriate for goats.
Dry-Off Procedures and Dry-Period Therapy
Dairy goats are commonly allowed a two- to three-month non-lactating (“dry”) period before the next parturition occurs. Provision of this rest period increases milk production in the next lactation. It also permits production of colostrum for protection of neonates; colostrum from goats with a 56-day dry period had an immunoglobulin (Ig)G concentration of 42.4 mg/mL, compared with 5.6 mg/mL in goats not given a dry period (Caja et al. 2006). It is possible to milk a goat daily for several years with reasonable milk yield if production of kids is not desired or the doe fails to conceive.
When does are milking heavily at the time of weaning or dry-off, it is helpful to restrict feed to a poor-quality roughage and (if climate permits) to limit water for several days. During this time, animals should be kept clean and dry and observed for inordinate udder swelling. In commercial dairy herds, careful infusion of a dry-period mastitis preparation (one tube per teat, to avoid contamination) is sometimes recommended. Udders that become severely distended should be milked out and retreated five to seven days later, but in general it is better to not disturb the keratin plug in the teat end. It is very important to clearly mark the animal that has been dry treated, because it is likely to try to return to the milking group if it is put into a different pen, and antibiotic residues will follow. Modern teat sealants can also be used in problem herds, but are less important when housing conditions are clean and dry. One Turkish study of Saanen goats showed that dry treatment with cephalexin and neomycin cured preexisting intramammary infections and significantly reduced the somatic cells counts in the subsequent lactation, although the addition of an internal teat sealant did not significantly improve the results (Ba⅞tan et al. 2015).
In one survey, 76% of udder half infections caused by major pathogens (S. aureus or streptococci) and 55% of infections caused by non-aureus staphylococci persisted through the dry period to the next lactation (Lerondelle and Poutrel 1984). Infusions of an appropriate long-lasting dry cow preparation (one tube per half) at the time of drying off should increase the cure rate during the dry period, while simultaneously preventing some new infections during this period. In one report, approximately two-thirds of infections were eliminated in goats receiving dry treatment (Plommet 1974). A study using a cattle cephapirin benzathine product found a 79% cure rate of infections, most of which were non-aureus staphylococci (Fox et al. 1992). In a study from New Zealand, a dry treatment licensed for goats containing 300 mg procaine penicillin, 100 mg dihydrostreptomycin, and 100 mg nafcillin resulted in a 92% cure rate, compared with 31% cure of untreated glands. S. aureus did not respond as well as other organisms. At the same time, new infections were reduced from 9 to 2% (McDougall and Anniss 2005), although most authors have not shown an effect on new infections. A 66-78% cure rate was found in another study using the same antibiotics (Poutrel et al. 1997), with no antibiotic residues detected seven days after parturition. Cloxacillin has also been shown to be efficacious (Paape et al. 2001). There are anecdotal reports of severe systemic reactions in goats treated with erythromycin dry cow preparations, so this drug should probably be avoided.
It has been suggested that herds with more than 30 or 40% subclinical mastitis should treat all goats at dry-off, while herds with lower infection rates should treat selectively those animals that are infected (Paape et al. 2001). In herds free of mycoplasma infection, two or more monthly cell counts greater than 2 million/mL have been shown to be indicative of S. aureus infection with a sensitivity of 100% and a specificity of 74%, thus aiding in the selection of goats to be dry treated (Baudry et al. 1999). Teat dipping before and after infusion and partial insertion of the tube are recommended.
Prevention of Bacterial Mastitis
Management decisions that decrease the risk of injury to the udder or teat (such as selecting for improved udder attachment) or that control skin lesions on the teats (including contagious ecthyma, staphylococcal infections, or warts; see Chapter 2) should decrease the risk of mastitis. Genetic aspects of udder conformation also affect the risk of mastitis via ease of machine milking (Barillet 2007).
Attention to sanitation, proper milking procedures, teat dipping, and dry-period antibiotic therapy are also beneficial. Less is known regarding the value of nutritional adjustments or vaccination programs in preventing mastitis in goats.
Environmental Considerations
Dry, clean surroundings are especially important at freshening and at dry-off. When goats are housed and fed dry hay, the dry consistency of their fecal pellets combined with their tendency to bed themselves on wasted hay usually ensures acceptable conditions. Otherwise, slatted floors or elevated sleeping platforms may help to keep conditions sanitary. Teat-end injuries predispose to mastitis and thus should be prevented as much as possible (Ameh and Tari 2000).
Milking Procedures The method of udder preparation for milking is very important in determining the incidence of new cases of mastitis in goats, as it is in cows. For example, herds in which individual towels were used to wash and dry the udder had a decreased prevalence of intramammary infections compared with herds in which common towels were used (East et al. 1987). Hands and udders should be clean and dry. Disposable nitrile gloves are recommended. Goat udders are usually cleaner than cow udders. If washing is required, only the teats should be washed. It is better not to wash at all than to leave the udder and teats wet. Sanitizer solution for washing teats should be delivered from a hose or spray bottle, rather than from an open bucket. Animals with mastitis or with skin lesions on the teats should be milked last, with appropriate sanitation of hands between affected animals. Careful attention to unit placement to prevent liner slip and teat-end impacts (causing reverse flow of milk into the udder) is important to prevent introduction of bacteria, mycoplasma, and the CAE virus into the gland during milking.
Goats should be milked gently and in quiet surroundings to encourage oxytocin release and milk letdown. The physiology of these events has been reviewed elsewhere (Martinet and Richard 1974). The biological half-life of oxytocin has been calculated to be approximately 22 minutes in goats (Homeida and Cooke 1984). The premilking stimulation afforded by udder washing is not necessary for goats to milk out completely. Research, then, has demonstrated no effect of udder washing on milking time or milk yield (Ricordeau and Labussiere 1970). This is because the goat holds nearly 80% of its milk in the cistern rather than in the alveoli, and means that the machine can be attached immediately if the teats are clean (Ohnstad 2006). The satisfied goat often ruminates while being milked. Vigorous stripping, by hand or machine, should be avoided. Overmilking of late-lactation does may contribute to the risk of mastitis (East et al. 1987). Restraining goats during milking by pulling on the teats has been proposed as one reason for a high incidence of gangrenous staphylococcal mastitis in Cyprus (Petris 1963). When machine milking, it is important to use a vacuum cut-off valve before removing the teat cups, to avoid teat-end impacts (Bergonier et al. 2003).
Milking should occur at regular times, but equal 12-hour intervals are not necessary. The goat has a relatively large gland cistern for holding milk. One study found no difference in yield with milk intervals of 16 : 8 hours and 12 : 12 hours (Henderson et al. 1983). Yield is increased by milking three times a day. French workers have also investigated the effects of omitting the Sunday-evening milking and have found a reduced milk yield of 4.5% if this practice is begun one month into the lactation, and only 1.2% if begun after five months. An increase in mastitis has not been noted, and on some farms the savings in labor costs more than offset the decrease in yield (Le Du 1987).
Preliminary research in France suggests that the speed of milking is under genetic control, with the goats homozygous for the recessive gene “hd” having the most rapid milk flow (Ricordeau et al. 1990). How this gene might affect the incidence of mastitis is uncertain, although another French study indicates that high milk flow rates correlate with higher SCCs (Palhiere et al. 2014). A later study found that milk flow is not well correlated with production, such that farmers are reluctant to cull high- producing does that milk slowly (Blasco et al. 2016).
Milking Parlor Design
A raised platform is the most basic equipment for milking goats, and most owners of small herds use individual milking stands. When herd size justifies construction of a parlor, several different designs are satisfactory and have been described (Le Du 1987; Mottram et al. 1991). These include a side-by-side parlor with milking from behind, herringbone parlor with milking from the side, inverted herringbone with milking from the front, and tunnel parlor with milking from the side. To additionally increase throughput, the goats, stalls, and milking units can be mounted on a rotating platform.
Milking Machine Function
When a commercial goat dairy installs or modifies a machine milking system, attention should be given to choosing an efficient system that milks goats under low vacuum with minimal vacuum fluctuation. Low-line systems, in which the milk line is just below the edge of the pit or elevated milking platform, are generally preferred. Vacuum levels of 10.0-12 in. Hg (Menzies et al. 2016) are appropriate for low-line systems, but a higher vacuum may be needed for high-line systems. Machines available for milking goats in France are operated at vacuum levels (gauge pressures) of 30-38 cm Hg (Darracq 1974). Yet another vacuum unit in use in the literature is the Pascal, which equals 10 dyne/cm2 or 7.5 ? 10-3 mm Hg; a kPa (kilopascal) equals 0.75 cm Hg. In Canada the recommendation for goat milking systems is 35-41 kPa (Menzies et al. 2016).
The vacuum pump should have a capacity of 30 cubic feet per minute (CFM; ASME standard) for the pipeline system, 1.5 CFM per unit, and 3-4 CFM reserve air flow. Bucket milker systems require 10 CFM reserve and 1 CFM per unit (East and Birnie 1983; Spencer 1984).
Pulsation rates of 60-120 per minute and pulsation ratios of 50 : 50 to 70 : 30 (milk : rest) have been recommended for goats (Le Du 1987; Menzies et al. 2016). In a study that attempted to optimize milking rate and SCCs, a pulsation ratio of 60 : 40, a pulsation rate of 90 per minute, and a vacuum level of 45-52 kPa were judged to be optimal (Lu et al. 1991). Another recommendation is for a vacuum of 37-38 kPa, a pulsation rate of 90-120 per minute, and a 50 : 50 pulsation ratio (Ohnstad 2006).
Inflations should be replaced before they become worn and cracked. Some authors propose changing inflations on the same schedule used for cows (every 1000-1500 milkings for molded rubber liners; East and Birnie 1983). In Europe, allowances are apparently made for the very short milking time (one to two minutes) per goat. One producers’ guide from France recommends changing inflations twice a year (Cardoen and Delahaye 1977). Silicone liners are more durable than rubber liners. Because liners tend to deteriorate with time, washing, and use, they should not be used for longer than the manufacturer’s recommendation. Rapid pulsation rates, frequent washings, and excessive chlorine will dictate more frequent replacement (Menzies et al. 2016).
Teat Dips
Although few studies have been conducted in goats, it is generally accepted that teat dipping or spraying with a properly mixed and uncontaminated solution is of economic benefit via the prevention of bacterial mastitis (Plommet 1974; Bergonier et al. 2003; Contreras et al. 2007). One French study documented a 62% decrease in new infections in early lactation and a 41% decrease over the entire lactation when the right teat was dipped but the left teat was an undipped control (Baudry et al. 2000). Some studies have found a beneficial effect on SCCs (Paape et al. 2001) while others have not (Poutrel et al. 1997). Products with evidence of efficacy for preventing mastitis in dairy cows (e.g., 0.5% iodine or 0.5% chlorhexidine) are commonly used. Nisin, a bacteriocin protein synthesized by the bacterium Lactococcus lactis subsp. lactis and long used as a food-grade preservative in dairy products, has also been shown to be effective in goats (Paape et al. 2001). Other non-conventional teat dips may be ineffective or even contaminated, as occurred when a home-made dip containing essential oils resulted in Pseudomonas mastitis (Kelly and Wilson 2016). Recently concerns have been raised that use of teat dips increases selection for bacteria that are resistant to disinfectants, which might impact human health (Contreras et al. 2007).
In small herds, purchasing large quantities of teat dip at one time should be discouraged, because settling of the product may occur and cause teat irritation. Even a newly purchased supply may cause problems because of past freezing or prolonged storage. When concentrates are used, they should be mixed with clean water; some pathogens such as Pseudomonas or even the common saprophyte Serratia can survive and even multiply in the teat dip (Van Damme 1982). Owners should also empty and sanitize the dipper after every milking. Hand pumps or aerosol sprays (e.g., chlorhexidine; Fightbac®, Deep Valley Farm, Brooklyn, CT, USA) help to avoid contamination of the teat dip, but the milker must take the time to ensure that the teat ends are adequately covered. Teat dipping for one week after dry-off or before kidding probably is of no value.
Dry-Period Therapy
Infusion of an antibiotic into the udder at time of dry-off, as discussed previously, helps to prevent new cases of mastitis in addition to curing some preexisting infections.
Vaccination
Staphylococcal toxoid vaccinations have been used in herds experiencing clinical mastitis caused by S. aureus (Petris 1963; Lerondelle and Poutrel 1984). An adjuvanted cell-toxoid vaccine (formolized cells and toxoid adjuvanted with aluminum hydroxide gel) has been used in studies using goats as a model for cows (Derbyshire 1960). These vaccines do not lower the prevalence of infection, but do decrease severity. In contrast, a polyvalent somatic antigen vaccine did not prevent mastitis or decrease severity of clinical signs (Lepper 1967). Field experiments with sheep vaccinated twice with oil adjuvanted alpha and beta staphylococcal toxoids demonstrated a reduced rate of clinical mastitis when compared with unvaccinated control sheep (Plommet and Bezard 1974). Recent studies on vaccination of goats for this organism or its toxins are lacking, although in one small study a commercial somatic antigen vaccine (Lysigen®, Boehringer Ingelheim, Ingelheim, Germany) tended to reduce the infection rate with non-aureus staphylococci and increased the self-cure rate (Kautz et al. 2014).
An attempt to increase resistance by gene therapy, causing expression of Iysostaphin in the goat udder, failed because of adverse immune reactions to the molecule (Fan et al. 2004).
Although E. coli mastitis is relatively rare in goats and vaccination as a substitute for hygiene is not justified, goats have been proposed as a model for coliform vaccination research in cattle. A J5 vaccine moderated the clinical signs and decreased shedding in the milk after experimental challenge (Aslam et al. 1995).
Nutrition
Although it seems reasonable that nutritional deficiencies should increase an animal's susceptibility to mastitis and other infectious diseases, few studies in goats are available. However, it has been shown that selenium deficiency is associated with reduced neutrophil function in goats (Aziz et al. 1984; Aziz and Klesius 1986). Also, SCC (by Fossomatic) was decreased and milk production increased in Finngoats with a high glutathione peroxidase activity when compared with goats with decreased selenium status judged by this enzyme's activity (Atroshi et al. 1985). This study did not include cultures of milk samples. In a selenium-deficient region in Spain, an injection of slow-release barium selenate before mating to half of the goats in four herds was associated with a significant decrease in SCCs and the incidence of clinical mastitis in the subsequent lactation of the supplemented goats. There were 10 clinically affected goats out of 260 treated animals, compared with 40 clinical mastitis cases in the 260 controls (Sanchez et al. 2007). Improved bactericidal activity of neutrophils in selenium-supplemented cows is believed to moderate the severity of E. coli mastitis in that species (Erskine et al. 1989). Vitamin E status is probably important for resistance to mastitis as well. One study that supplemented both selenium and vitamin E saw a decrease in SCCs in the treated goats relative to controls (Tufarelli and Laudadio 2011).
Mycoplasma Mastitis
When repeated efforts to isolate bacteria from udders affected with clinical mastitis yield no growth or only nonhemolytic staphylococci, the possibility of mycoplasmal involvement should be investigated. The simultaneous presence of mastitis with other clinical signs such as arthritis, pneumonia, or conjunctivitis also warrants consideration of mycoplasma.
Etiology
Mycoplasma is a genus of small and fastidious bacteria that lack a cell wall, but instead are enclosed in an outer cell membrane. They belong to the class Mollicutes. Numerous species of mycoplasma have been isolated from the milk of goats (DaMassa et al. 1992; Bergonier and Poumarat 1996), sometimes with more than one species present in the same animal (Gil et al. 1999b) or the same herd (Kinde et al. 1994; De la Fe et al. 2005). Others have been infused experimentally into goat udders to test pathogenicity. The various organisms cannot be distinguished on clinical grounds.
Mycoplasma agalactiae
Contagious agalactia of sheep and goats is a specific disease common in Mediterranean countries, much of Europe, the Middle East, and South Africa. The causative agent is classically Mycoplasma agalactiae, although some authors now use the term contagious agalactia for almost any mycoplasmal mastitis of small ruminants (Corrales et al. 2007; OIE 2018). As discussed in Chapter 4, M. agalactiae, Mycoplasma capricolum subsp. capricolum, Mycoplasma putrefaciens, and M. mycoides subsp. capri (previously M. mycoides subsp. mycoides LC type) are recognized by the World Organisation for Animal Health (OIE) as causes of contagious agalactia for regulatory purposes. M. agalactiae is generally considered to be exotic to the United States, although it has been isolated from goats in California (DaMassa 1983; Kinde et al. 1994). In many regions this condition must be reported to regulatory authorities.
Septicemia occurs in infected animals, and the organism may then localize in the udder, joints, or eyes. M. agalactiae is shed for months via milk, urine, feces, and ocular and nasal discharges. Infection can be by either ingestion or inhalation. The environment becomes contaminated, and infections may spread via communal browsing areas or driving routes (Dhanda et al. 1959; Corrales et al. 2007). Asymptomatic carriers for the various mycoplasma species are common in goat herds (Gomez-Martin et al. 2013).
Mycoplasma mycoides subsp. capri; Mycoplasma mycoides subsp. mycoides (Large Colony)
M. mycoides subsp. capri is the current name of this organism that is now considered to be one cause of contagious agalactia (Manso-Silvan et al. 2009). M. mycoides subsp. capri has been isolated from goats with mastitis in France (Perreau et al. 1972; Perreau and Breard 1979) and in the Mediterranean region in general (Corrales et al. 2007). In India, M. mycoides subsp. capri has produced a purulent mastitis after experimental inoculation (Misri et al. 1988). California goat dairies have experienced mastitis outbreaks and polyarthritis in kids due to the same species, although it was classified as M. mycoides subsp. mycoides (LC type; East et al. 1983). Its role in respiratory disease is discussed in Chapter 9. In Israel, udder inflammation and agalactia in does and conjunctivitis and polyarthritis in kids have been reported to be caused by M. mycoides subsp. mycoides (ovine/caprine) serogroup 8 (Bar-Moshe and Rapapport 1978, 1981), which is possibly the same organism.
Mycoplasma putrefaciens
M. putrefaciens has caused outbreaks of mastitis, agalactia, abortion, and arthritis in a large California dairy (DaMassa et al. 1987) and in Europe (Gaillard-Perrin et al. 1986; Mercier et al. 2000) and the Middle East. Subclinical mastitis can occur also. Some goats infected with M. putrefaciens have no visible changes in the milk nor palpable inflammation or fibrosis (although milk leukocyte percentages are increased). Even when agalactia develops, fibrosis is absent (Adler et al. 1980). The organism does not seem to induce a febrile response (DaMassa et al. 1992).
Other Mycoplasmas
M. capricolum subsp. capricolum has been isolated from goats with mastitis in France (Perreau and Breard 1979; Picavet et al. 1983). Intramammary inoculation of several M. capricolum strains produced severe mastitis (thick yellowish secretion, increased cell count, agalactia, enlargement of the supramammary nodes) in does, and pneumonia, polyarthritis, and keratoconjunctivitis in nursing kids (Taoudi et al. 1988). M. capricolum has also been isolated from California goats.
Mycoplasma arginini has produced natural cases of purulent mastitis in goats in India (Prasad et al. 1984) and the condition has been reproduced experimentally (Prasad et al. 1985). Leukocyte counts were markedly increased and agalactia developed. In contrast, Jones (1985) was unable to demonstrate pathogenicity of M. arginini to the goat udder. The organism is usually considered to be non- pathogenic (DaMassa et al. 1992). Mycoplasma auris has been identified as the cause of clinical mastitis in goats in Spain (Garcia-Galan et al. 2020).
Experimental inoculation of goat udders with Acholeplasma laidlawii has produced mastitis leading to agalactia and marked fibrosis (Singh et al. 1990). The goat udder has also been used to test other strains of mycoplasmas isolated from other species or body systems for potential pathogenicity (Pal et al. 1983; Jones 1985).
Clinical Signs
Contagious agalactia (M. agalactiae) often appears in a herd in the spring, soon after lactation begins. An incubation period of 7-56 days has been reported. Early signs (during the septicemic stage) include inappetence, depression or malaise (United States Animal Health Association 2008), and an unwillingness to follow the herd. A purulent mastitis and agalactia then develop. The secretion is initially watery, but later turns thick or lumpy. Keratoconjunctivitis or arthritis may occur in the same goats or in kids drinking unpasteurized milk. Mortality of untreated animals can approach 20%. Some herds have animals infected with and shedding M. agalactiae in milk without clinical mastitis or elevation in the bulk tank SCC (Corrales et al. 2004).
Clinical signs with other mycoplasma infections are variable. The classic mastitic mycoplasma milk sample is one that separates into a granular sediment and a greenish- yellow watery supernatant. The milk is said to have a putrefactive odor when M. putrefaciens is the cause of the mastitis. In acute, severe cases, both mammary gland and supramammary lymph node are enlarged. Both halves of the udder are often but not always affected, and there is no response to treatment. Milk production ceases quickly, with does essentially agalactic in two to three days. The udder atrophies, but may be completely functional after the next parturition. Some does die during the acute stage of the disease (East et al. 1983; Gil et al. 1999a). Some mycoplasmas also may be associated with respiratory disease or abortion.
Diagnosis
Mycoplasma should be suspected if blood agar cultures of milk samples from a herd outbreak of mastitis are negative. Appropriate cultures for mycoplasma (for instance on Hayflick’s medium) should then be initiated. In herds with M. mycoides subsp. capri, it has been noted that most milking does are asymptomatic with normal appearance to the milk, though large numbers of mycoplasma are present. This species is somewhat unique in that it can be isolated on sheep or calf blood agar, where colonies resemble alpha- hemolytic streptococci but no bacteria are seen on Gram stain (Rosendal 1994). When contagious agalactia is suspected, other samples from septicemic animals can also be positive by culture, including ocular swabs, ear swabs (De la Fe et al. 2005), joint fluid, blood, liver, spleen, feces, and urine. As with respiratory disease, the identification of the species of mycoplasma involved in a mastitis outbreak can be hastened and simplified by using appropriate PCR tests (Nicholas 2002; Corrales et al. 2007). Serologic testing using ELISA can also be helpful if vaccination is not part of the control strategy (Corrales et al. 2007). Commercial ELISA kits for M. agalactiae are available in Europe (OIE 2018).
Histopathologic examination of the mammary gland reveals marked interstitial infiltration with mononuclear leukocytes, especially around acini and ducts. Mononuclear cells and desquamated epithelial cells are seen in ducts. Giemsa stain can be used to demonstrate the mycoplasma (Dhanda et al. 1959), but immunochemistry is more specific and preferred (Corrales et al. 2007).
Treatment
Treatment is generally ineffective. Improvement in systemic signs is usually noted with drugs generally used against mycoplasma (such as tetracycline, tylosin, erythromycin, spiramycin, lincomycin, tiamulin, florfenicol, or fluoroquinolones where legal), but the goat is apt to become an inapparent carrier (Perreau 1974; Bergonier and Poumarat 1996; Nicholas 2002; Gomez-Martin et al. 2013). Thus, slaughter of all infected goats is recommended unless the herd is in an endemic region. Practitioners should particularly avoid infusion into the udder of preparations of tylosin or erythromycin meant for systemic administration. The irritating nature of these drugs often ensures destruction of milk-secreting tissue, even if the infection can be eliminated. It has been reported that tia- mulin at 10 mg/kg intramuscularly can maintain concentrations in the udder inhibitory for M. agalactiae for 12 hours (Ziv et al. 1983). Spectinomycin penetrates the udder poorly. In endemic herds, using an anti-mycoplasma treatment for all animals at dry-off has been recommended (Corrales et al. 2007).
Control
Because mycoplasma mastitis is usually introduced into the herd by a carrier goat or sheep (Ruhnke et al. 1983), it is very important to investigate the health status of the herd of origin before buying or boarding an animal. Serologic tests have been undertaken in some countries with the aim of eradicating infection from herds and preventing reintroduction. The variety of species possibly involved complicates this approach. Serology using ELISA tests for M. agalactiae and M. mycoides subsp. mycoides LC (M. mycoides subsp. capri) has shown promise for identifying individual carrier goats (Davidson et al. 1989). Culture tests of bulk tank samples appear to be a starting point in regions where the problem occurs. An outbreak of mastitis may be delayed until several months or years after the introduction of carrier animals (Picavet et al. 1983). Stress, as is associated with parturition or with transport and adjustment to a new herd, appears to trigger shedding of the organism.
As with all cases of mastitis, affected animals should be milked last and hands or milking machines disinfected before milking other goats. Common udder towels should be avoided. In dairy herds undertaking an eradication program for M. mycoides subsp. capri, one approach is to cull all positive animals to slaughter based on an initial herd culture. Then colostrum is cultured from each doe at freshening. The eradication efforts are monitored by frequent culturing of tank milk from each milking string (East et al. 1983). Because feeding of raw colostrum and milk can be the source of serious joint and lung infections, a pasteurizer should be used if goat milk is to be fed to kids.
M. agalactiae and related organisms are shed in urine and feces, making the environment an important source of infection to other sheep and goats. Stalls should be disinfected and litter removed. Mycoplasma are inactivated by many routine disinfectants, including sodium hypochlorite (30 mL of household bleach in 4 L of water), cresol, 1% formalin, and ionic and non-ionic detergents (United States Animal Health Association 2008). A variety of vaccines against M. agalactiae, both killed and attenuated, have been evaluated. Although some provide protection from clinical disease and are thus very useful in endemic areas, carrier states may still develop (Foggie et al. 1970, 1971; Arisoy 1973; United States Animal Health Association 2008; OIE 2018). In regions where vaccination is routine, leaving a small population of unvaccinated sentinel animals in the herd permits monitoring of disease activity by serologic screening (Corrales et al. 2007). Goats previously inoculated with M. putrefaciens showed resistance to subsequent challenge for at least one year (Brooks et al. 1981), suggesting that a vaccine might also help to control this organism.
Retroviral Mastitis (Hard Udder)
Goat owners in the United States and Australia have been frustrated for many years by a condition known as “hard udder.” More recently a milder form of the condition has been recognized in many countries.
Etiology and Epidemiology
Undoubtedly, the diagnostic characteristics of a firm udder at parturition with scanty milk flow are not specific enough to limit “hard udder” to a single etiology. However, it has become clear since the discovery of CAE that the condition as a herd problem tends to disappear when CAE is eradicated from the farm (Kapture 1983). Interstitial mastitis has been recognized in two goats experimentally infected with CAE virus (Cork and Narayan 1980). A similar hard udder syndrome has been recognized in sheep infected with the closely related ovine progressive pneumonia and maedi-visna viruses (Cutlip et al. 1985; van der Molen and Houwers 1987). A more recent histologic study of 62 agar gel immunodiffusion (AGID)-positive native goats in Japan found non-suppurative mastitis in 80% of the animals (Konishi et al. 2006). Infection is readily spread and histologic lesions created by introducing infected cells into the udder (Lerondelle et al. 1995).
It is not clear if CAE is involved in the etiology of cystic hyperplasia of the caprine mammary gland described in the older literature from India (Singh and Iyer 1973; Sharma and Iyer 1974). Periductal and perilobular fibrosis infiltrated by lymphocytes was associated with dilated ducts in the cystic lesions. “Udder edema” accompanied by decreased milk flow is another poorly described condition that might be related to CAE virus (Sedgman 1982). When true udder edema is present (as described earlier in this chapter), the skin pits on pressure.
There is a recent suggestion that the scrapie agent could be excreted in the milk of sheep with retroviral interstitial mastitis (Ligios et al. 2005). Scrapie is not common in goats (see Chapter 5), but the possibility of horizontal spread of scrapie via milk of CAE-infected goats is intriguing. The prion has been demonstrated in the udder of scrapie- infected goats that also had a lymphoproliferative mastitis caused by the CAE virus (Gonzalez et al. 2010).
Clinical Signs
When the acute form of retroviral mastitis appears at parturition, the udder is very firm, almost like a rock, but the overlying skin is loose and free of edema. Heat and erythema are also absent. Almost no milk can be obtained, even with the aid of oxytocin and warm compresses. What milk is obtained appears normal, but has an elevated cell count (Lerondelle 1988). Signs of systemic illness are absent. Some affected goats come gradually to milk over a period of several weeks, which has allowed numerous medical or herbal treatments to appear to be effective. In other animals, palpable induration of the udder or udder half persists (Zwahlen et al. 1983; Gregory et al. 2009). Supramammary lymph nodes are enlarged. Clinical signs may be less severe and cell counts lower in subsequent lactations (Le Guillou 1989; Lerondelle 1989).
Careful udder palpation reveals increased firmness in additional does that appear to be milking normally. A Swiss study based on palpation of the udder of 1517 animals found palpable changes (diffuse or focal induration of the parenchyma) in 23% of ELISA seropositive goats, 19% of suspicious goats, and only 7% of seronegative animals (Krieg and Peterhans 1990). Bacteriologic cultures were not undertaken.
Reported effects on milk production and quality have been inconsistent. Some but not all studies have shown total milk production to be higher on average in seronegative animals than in seropositive goats. This was the case in 3913 Marciana-Granadina does in Spain, where the negative goats had longer lactations, higher milk yield as well as milk fat and lactose, and lower SCCs. However, the higher milk yield observed in all 10 herds was statistically significant in only 3 of them (Martinez-Navalon et al. 2013).
Diagnosis
Diagnostic evaluation should include a physical examination to detect other problems such as metritis, udder edema, and teat obstructions. Udder biopsy might be performed (Gregory et al. 2009), but microscopic examination is more commonly performed at necropsy. Histologic changes reported for retroviral mastitis in goats and sheep include accumulation of mononuclear cells (lymphocytes, macrophages, and plasmacytes) in the parenchyma and around ducts in the udder (Zwahlen et al. 1983). These mononuclear cells are sometimes organized into lymphoid follicles, a histologic change that has been seen in a 3-month-old doeling infected naturally with CAE and in adults (Kennedy-Stoskopf et al. 1985). These cellular infiltrations may externally compress ducts or protrude into ducts, preventing the passage of milk (Post et al. 1986). Lobular atrophy and prominent corpora amylacea are also reported in CAE-affected udders.
Bacterial and mycoplasmal cultures and herd testing for CAE are performed if the owner or veterinarian is unsure of the diagnosis, but dual infections are possible. Not every animal infected with the CAE virus has detectable serum antibody, especially at parturition when circulating antibody has passed into the colostrum. Many goats with CAE infection (including many shedding virus in their milk) do not develop a hard udder. Thus, serology is inconclusive at best, as is demonstration of the virus in the milk by PCR. However, if the entire herd is free of serologic evidence of the virus, the diagnosis becomes very unlikely.
Treatment and Control
No cure for the interstitial mastitis has been identified, and culling is indicated. Cortisone administered two days before expected parturition has been reported to cause regression of clinical signs in some goats (Lerondelle 1988). Control is through a CAE eradication program, as discussed in Chapter 4. Kids should be removed from the affected doe and fed virus- free colostrum and milk. Infected animals, if left in the herd, should be separated and milked last, and milk or whey should not be fed back to any goats in the herd without proper heat treatment.