Infectious causes of small intestinal disease
5.3.2.1 Viral infections
5.3.2.1.1 Canine parvovirus enteritis
Canine parvovirus (CPV) is a small, non-enveloped DNA virus that is highly resistant in the environment. Disinfection of contaminated areas must be performed with sodium hypochlorite (i.e., household bleach).
There are two known5 strains of CPV: CPV-1 and CPV-2.1,2 For the most part, clinically important disease is caused by CPV-2 infection in dogs below 6 months of age. In the 1980s, CPV-2 evolved into two different strains, CPV-2a and CPV-2b.2 During this evolution, the virus became more pathogenic and developed a higher capacity to replicate in susceptible tissues. CPV-2 is a highly contagious virus that is transmitted predominantly by contaminated feces. The incubation period in the field is 7-14 days. Rottweilers, Doberman Pinschers, Labrador Retrievers, American Staffordshire Terriers, German Shepherd dogs, and Alaskan Sled dogs have been reported to be at an increased risk for infection.3
The virus enters through oronasal lymphoid tissue and spreads by way of the lymphoid system to other organs with rapidly dividing cell lines, mainly intestinal crypt epithelium and the bone marrow. The virus destroys intestinal crypt cells, which leaves the epithelium more susceptible to secondary bacterial infections, especially with gram-negative bacterial organ- isms.4,5 After contact with CPV-2, most older puppies and adult dogs undergo a subclinical infection. Puppies with severe infections are usually under 12 weeks of age at the time of infection. Vomiting, foul-smelling and often bloody diarrhea, anorexia, and dehydration develop 2-5 days after infection. Fever associated with secondary bacterial infection due to leukopenia and the breakdown of the intestinal barrier is also frequently seen.6 Myocarditis can be observed in puppies that have been infected in utero or up to 8 weeks after birth.7 A preliminary clinical diagnosis of CPV-2 infection is likely when the typical signs of acute vomiting, bloody diarrhea, and dehydration are seen in a young dog with an uncertain vaccination history.
An in-house fecal ELISA test is available to diagnose CPV infection. The ELISA test is only positive during the time of viral shedding, which is up to 10-12 days post infection. However, the test can be falsely positive if the dog has been vaccinated with an attenuated live vaccine.8 The only possibility to differentiate between an infection and a vaccine strain in these cases is by PCR-based detection of viral DNA in feces.9
Table 5.2: Fluid therapy. This table shows guidelines for designing fluid therapy in patients with acute gastrointestinal disease.78 Please note that for every patient all three components need to be estimated. The total volume of fluids given per hour is the sum of volumes given for each of the three components on an hourly basis.
Replacement of deficit
Dehydration (%) x body weight (kg) x 10 = ml of fluid to be administered over 4-6 hours
Maintenance fluid requirement
40-60 ml/kg body weight/24 hours
Ongoing losses
Estimate ongoing losses through vomiting and/or diarrhea and replace with maintenance fluids
Table 5.3: Potassium supplementation. Guidelines for potassium supplementation in patients with acute gastrointestinal disease.78
| plasma K | mmol | mmol | mmol | maximum fluid | ||||||||||||||||||||||||
| (mmol/L) | KCl/250 ml | KCl/500 ml | KCl/1000 ml | rate ml/kg/h | ||||||||||||||||||||||||
| and gastrointestinal tracts, which are followed by neurological signs. Maternal antibodies can persist in puppies up to 14 weeks after birth.15 Vaccination schedules for CVD therefore should include booster vaccinations every 3-4 weeks until the puppies are 16 weeks of age. 5.3.2.1.3 Feline coronavirus infection Feline coronavirus (FeCoV) infection can manifest itself as two different syndromes: a transient, most often mild diarrhea or as a disseminated granulomatous disease, feline infectious peritonitis (FIP). The disseminated disease is believed to be caused by a mutation of the FeCoV resulting in increased tropism for macrophages.16 It has also been speculated that repetitive infection with large doses of the virus associated with stress and a crowded environment may lead to FIP in young cats.17 The virus is transmitted by ingestion or inhalation. It primarily infects intestinal epithelial cells, but can spread to macrophages if it carries a gene that encodes a specific spike protein. This may then lead to FIP by initiating an immune-complex disease.16 The intestinal infection is mainly seen as a mild, transient disease. It is sometimes associated with vomiting, and is usually self-limiting with supportive care alone.every 3-4 weeks until 16 weeks of age, followed by a booster at one year of age are recommended. Thereafter, revaccinations every 3 or more years are protective. 5.3.2.1.5 Feline leukemia virus (FeLV) and feline immunodeficiency virus (FIV) Cats infected with FeLV or FIV predominantly show signs of immune-suppression, lymphoma, leukemia, and non-regen- erative anemia. Diarrhea is often a sign of general immunosuppression associated with secondary infections with enteral viruses, bacteria, or fungal organisms.20 Aggressive symptomatic therapy may control the clinical signs, but the long-term prognosis in these patients is poor. 5.3.2.2 Bacterial Infections
5.3.2.1.4 Felinepanleukopenia Feline panleukopenia is caused by the feline parvovirus (FPV), a very stable virus without an envelope that survives in the environment for up to 1 year. However, disinfection can be achieved with sodium hypochlorite (i.e., household bleach, undiluted), 4% formaldehyde, and 1% glutaraldehyde. The virus is shed in the feces for up to 6 weeks after infection. Most infections with FPV are subclinical. The virus usually spreads from the tonsils to other lymphoid tissues, the bone marrow, and intestinal crypt cells. The most severe clinical signs are seen in 3- to 5-month-old unvaccinated kittens. Fever, depression, anorexia, vomiting, severe dehydration, bloody diarrhea, and oral ulcerations are most commonly seen. In pregnant queens, the clinical signs can include infertility, mummified fetuses, and abortions. If the infection occurs during late pregnancy, the developing kittens can suffer cerebellar damage causing a typical hypermetric gait and intention tremors in neonates.18A presumptive diagnosis of FPV infection is made based on the clinical signs along with a severe leukopenia (50-3000 leucocytes/ml). An ELISA test similar to the one available for CPV is useful to confirm infection.19 Treatment is mostly supportive, with parenteral fluid therapy as a mainstay. Broad-spectrum antibiotic treatment in febrile neutropenic kittens is important and amoxicillin, cephalosporins, and /or gentamycin have been recommended. However, gentamycin should be used cautiously and should be avoided in patients that are dehydrated. In addition, antiemetic therapy with metoclopramide, dolasetron, or thi- ethylperazine is often necessary. Colostral antibodies against FPV persist in kittens for 12 to 14 weeks, and vaccination regimens with vaccinations as early as 6 weeks of age, then The small intestinal lumen naturally harbors a limited number of a variety of bacteria. This resident bacterial flora has important functions in preserving anatomical structures and enhancing the physiological processes necessary for the proper digestion and absorption of dietary components. The small intestinal flora also plays a role in preventing colonization by pathogenic bacteria, and positively influences the development of the enteric immune system. The composition of the resident bacterial flora can be modulated by diet and /or pre- and probiotic agents. Although not the most common etiology of small intestinal disease, bacterial infections with pathogenic bacterial species have been documented in small animals. Responsible enteropathogens include Campylobacter spp., Clostridium perfringens and difficile, Salmonella spp., Yersinia spp., and some strains of E. coli. However, some of these bacterial species have not only been isolated in feces of dogs and cats with diarrhea, but also in healthy animals.21 To further complicate matters, pathogenic bacteria may just be opportunistic in patients with intestinal diseases due to an unrelated cause. If enteropathogenic bacteria are not the actual source of the animal’s clinical signs and it is assumed that they represent an incidental finding, indiscriminate use of antibiotics is not recommended as it may lead to the development of resistant strains with possible public health relevance. Even though the pathogenicity of many of these bacteria is subject to controversy, a risk for the development of zoonotic infections in humans after contact with an infected pet does exist. More importantly, such a risk also exists when the infected pet is healthy, but is shedding enteropathogens. These facts often make diagnostic and therapeutic decisions difficult. Additional research is needed to more clearly establish the role of the small intestinal microflora in general, and enteric pathogens in particular, in both canine and feline intestinal disease.
Figure 5.3: Campylobacter spp. This figure shows an electron-microscopic image of a Campylobacter spp. organism. Note the spiral shape of the flagellated organism (12,000x; image courtesy of Dr. Mary Parker, Institute of Food Research, Norwich, UK). 5.3.2.2.1 Campylobacter spp. Campylobacter spp. are slender and curved gram-negative rods with polar flagella that typically appear in spiral shapes (Figure 5.3). These microorganisms are motile, and grow under microaerophilic conditions. Campylobacter spp., such as C. jejuni may attach to and invade host enterocytes and produce soluble components with enterotoxin-like activity.22 Numerous reports have shown that C. jejuni, C. upsaliensis, and other enteric Campylobacter spp. may be present in the feces of healthy as well as diarrheic dogs and cats.21,23 Campylobacter infections appear to be less frequent in cats than in dogs.24,25 Interestingly, studies performed in Europe yielded a higher incidence of Campylobacter spp.-positive pets in the investigated populations than those reported in studies from North America.26 Based on a recent epidemiological study from Switzerland, Campylobacter spp. could be detected in the feces of approximately 42% of healthy dogs and cats presented for vaccination.27 A longitudinal study of healthy 3-month-old pet dogs in Denmark revealed that 60% of the dogs evaluated carried Campylobacter spp. in their fecal matter. At one year of age, nearly 100% of the dogs were shown to be positive. At 2 years of age, the microorganisms could be isolated in 67% of the population.28 Moreover, 21% of healthy dogs < 12 months of age were reported to shed Campylobacter spp., and shedding was more than twice as common in young dogs with diarrhea as in healthy dogs.28Clinical signs in dogs and cats, if present, may vary widely. Diarrhea can be mild with occasional loose stools, moderate, or severe with watery or bloody feces with or without mucus. Clinical disease may be precipitated by stressful situations (i.e., boarding, concurrent diseases, etc.). Cytological evaluation of a rectal swab may reveal Campylobacter-like organisms with their typical slender curved rod or seagull-shaped appearance (Figure 5.3). Moreover, the presence of leukocytes indicates intestinal inflammation. Diagnosis is made by cultural identification of Campylobacter spp. in fresh fecal samples or rectal swabs. Shipping of fecal samples is usually not a problem as Campylobacter spp. remain stable for at least 3 days at room temperature, and 1 week if refrigerated. Alternatively, PCR-based assays for the detection of pathogenic Campylobacter strains in fecal samples are available (www.cvm.tamu.edu /gilab). The therapeutic approach to dogs with proven fecal shedding of Campylobacter spp. depends on the health status of the patient (i.e., healthy vs. showing signs of GI disease). Healthy patients that are found to be positive and are sharing a home with immune-compromised people or with infants should probably be treated. For all other situations, the necessity of antibiotic treatment in healthy dogs is controversial. In animals showing diarrhea, vomiting, and/or other signs compatible with small intestinal disease, appropriate antibiotic therapy is recommended, even though the causal relationship of Campylobacter spp. infection and the clinical signs may be difficult to establish. The antibiotics of choice for treating campylobacte- riosis in dogs and cats are erythromycin or fluoroquinolones (Table 5.4). The prognosis for full recovery is generally good. If an infection occurs secondary to another underlying intestinal disease, recovery may also depend on the identification and treatment of that condition. Campylobacter spp. can also infect humans, and cause abdominal discomfort, fever, and diarrhea, which may be bloody. Recovery frequently occurs spontaneously but antibiotic treatment may be required. In several countries, Campylobacter infections have now become the most common intestinal infection observed.27 Based on recent studies, risk factors for human infection include eating poultry cooked at home, drinking water from a well, lake or river, and daily contact with a dog.29 Therefore, fecal shedding of Campylobacter spp. by healthy infected pets may represent a source of infection in people. Dogs and cats seem to function as reservoir hosts for C. upsaliensis and C. helveticus (with 30% and 35% prevalence, respectively) with an increased risk of fecal shedding in animals < 3 years of age. However, the role of these organisms in the epidemiology of C. jejuni infections is deemed to be negligible as the prevalence of isolates is low.27 5.3.2.2.2 Clostridium spp. Clostridia are large gram-positive bacteria that produce endospores. Most pathogenic Clostridia are strict anaerobes. Some Clostridia are part of the normal intestinal microflora; however, Table 5.4: Antimicrobials. Recommended antimicrobials for the treatment of small intestinal bacterial infections.
5 1 Vomiting is a relatively frequent side effect after administration of erythromycin to dogs and cats. 2 First choice for therapy of Campylobacter spp. infections. 3 Tetracyclines are also frequently effective for the treatment of Campylobacterspp. infections if erythromycin or fluoroquinolones cannot be used. 4C. difficile-associated diarrhea is best treated with metronidazole. 5 Antimicrobial treatment should be based on the results of in vitro sensitivity testing. C. perfringens type A as well as C. difficile may be responsible for GI disease and enterotoxemia in dogs or cats.30-31 Clostridium perfringens. C. perfringens is widespread in the environment and can be present in feces of healthy animals. The two main toxins produced by C. perfringens type A are major toxin α and enterotoxin (also called C. perfringens enterotoxin or CPE). Enterotoxigenic C.perfringens are commonly associated with food poisoning in humans. CPE can be detected in fecal samples using immunoassays. Although C. perfringens could be cultivated from canine fecal samples in 76-86% of healthy and 71-75% of diarrheic dogs, only 5-14% of isolates from healthy dogs and 15-34% of those from dogs with diarrhea were enterotoxigenic.30 Enterotoxigenic strains have been associated with nosocomial diarrhea, hemorrhagic enteritis, and acute or chronic large and/or small bowel diarrhea.32 Since CPE may also be present in the feces of healthy, non-diarrheic dogs, it is possible that enteritis only develops if large enough concentrations of CPE are present in the intestinal lumen. However, currently available immunoassays do not allow for a quantitative assessment of fecal CPE. Isolation of C. perfringens in feces is not sufficient for the diagnosis of C. perfringens-associated disease. Endospore counts performed on fecal smears are also unreliable. The clinical value of CPE assays as an accurate marker of pathogenicity of C. perfringens remains to be determined, but, as mentioned above, fecal CPE has been detected in a larger proportion of diarrheic than healthy dogs. Options for antimicrobial treatment are summarized in Table 5.4. Clostridium difficile. Clostridium difficile produces two major toxins (toxins A and B). Infections with toxin-producing species are a common cause of nosocomial and antimicrobial- associated enteric infections in human beings and may lead to a potentially fatal pseudomembranous colitis, even though asymptomatic carriage has also been reported in humans. In various studies, C. difficile was cultured from the feces of healthy puppies and their dams, healthy adult dogs and cats, and di- arrheic dogs and cats presented to veterinary clinics. C. difficile has also been isolated from the feces of dogs with nosocomial diarrhea, and was recovered during environmental surveys of veterinary hospitals where nosocomial clostridial infections had occurred.32,33 Also, toxins A and /or B were detected significantly more frequently in diarrheic pets than in healthy pets. Therefore, a causal relationship between enterocolitis and C. difficile should only be suspected if toxins A and/or B can be detected in a fecal sample. Recommendations for antimicrobial therapy are summarized in Table 5.4. 5.3.2.2.3 Enterobacteriaceae This family of enteric gram-negative rods contains numerous genera and species. The major gastrointestinal pathogens in small animals that belong to this family are Escherichia coli and Salmonella serovars. 5.3.2.2.4 Pathogenic E. coli Shortly after birth, E. coli from environmental sources colonize the mammalian intestinal tract where they persist as an important member of the normal flora. Most strains have a low virulence and may occasionally cause infections in extra-intestinal locations such as the urogenital tract. Pathogenic E. coli have a variety of virulence factors such as adhesins, which allow their adhesion to mucous membranes; capsular polysaccharides that interfere with phagocytosis by host cells; and endotoxin, a lipopolysaccharide cell wall component.34 Shiga-toxin-producing E. coli (STEC) could be isolated with a similar frequency from healthy and diarrheic dogs, which suggests that they are not pathogenic in dogs. Canine entero- pathogenic E. coli (EPEC) have been described in young dogs with diarrhea, but their actual clinical significance remains un- known.35 In a study of 122 dogs with diarrhea at the time of death, 44 dogs had EPEC. Of those dogs, 29 were affected by concurrent enteric pathogens such as parvovirus.35 In contrast, enterotoxin-producing E. coli (ETEC) could only be isolated from young dogs with diarrhea, and not from healthy animals. Based on the paucity of published reports, intestinal infections with E. coli do not seem to play an important role in canine and feline patients. Theoretically, asymptomatic canine carriers of STEC could be a source for human infections. However, the general risk of zoonotic transmission appears to be low. 5.3.2.2.5 Salmonellae Salmonella serovars occur worldwide and may infect mammals, birds, and reptiles. The majority of Salmonellae of veterinary importance are serotypes of S. enterica subspecies enterica. In humans, the most common route of infection is by ingestion of contaminated food, especially chicken eggs and other egg products, but also meat products from pigs and chickens. Recently, serotype infantis cultured from dried pig ears marketed as dog treats was determined to be the cause of an outbreak of human disease in Canada and the USA.36 In humans, the disease is characterized by diarrhea, fever, and abdominal cramps, often with a mild to moderate and self-limiting course. Generally, healthy adult carnivores are considered resistant to salmonellosis. In recent prevalence studies, Salmonella serotypes could only very rarely be cultured from the feces of healthy or diarrheic dogs and cats. Only up to 2.3% of dogs and 1% of cats shed Salmonella spp. in their feces. However, in a study from Belgium, the frequency of Salmonella spp. isolation was much higher.37 This study evaluated group-housed kittens (isolation frequency: 51.4%) and cats that had died or were euthanized due to incurable disease (isolation frequency: 8.6%).37 Although pets are rarely confirmed as the source of human salmonellosis, occasional outbreaks of Salmonella infections may be associated with visits to a veterinary clinic.38 Thus, the practice of good hygiene is strongly recommended, especially when dealing with highly susceptible individuals such as infants, the elderly, and immune-compromised people.39 Clinical signs in dogs and cats with salmonellosis include fever, vomiting, diarrhea, anorexia, weight loss, and lethargy. Sepsis was reported as a complication of clinical salmonellosis in two cats fed a raw meat diet.40 In another report, several kittens died of systemic salmonellosis, shortly after vaccination with a modified live panleukopenia vaccine.41 Diagnosis is made on the basis of fecal isolation of Salmonella serotypes in a patient with compatible clinical signs. The CBC may reveal changes suggestive of sepsis. Treatment consists of fluid therapy and other supportive measures. Administration of antimicrobials is only recommended in pets with systemic infection, and is based on the sensitivity results of the isolated Salmonella strain (Table 5.4). In pets recovering from clinical salmonellosis, chronic carriage of Salmonella over several weeks post recovery may occur as a result of organisms remaining in the local lymph nodes. This may require long-term parenteral administration of an appropriate antibiotic. Because they are resistant to many environmental factors, Salmonella organisms may survive for long periods of time in the environment.42 5.3.2.2.6 Other bacteria Ileocolitis associated with Anaerobiospirillum infection was reported in six cats from California.43 This organism belongs to a genus of small, spiral, gram-negative motile bacteria that had been previously isolated from the throat and feces of normal dogs and cats. Three infected cats had gastrointestinal signs, two of which had diarrhea, one cat was anorectic and lethargic, and two cats had clinical signs unrelated to the GI tract. All six cats were euthanized or died, and ileitis and /or colitis were confirmed histologically. Using light and electron microscopy as well as PCR amplification, Anaerobiospirillum spp. was demonstrated in the intestinal lumen of all six cats.43 The exact role of these bacteria in the pathogenesis of intestinal disease remains to be elucidated.
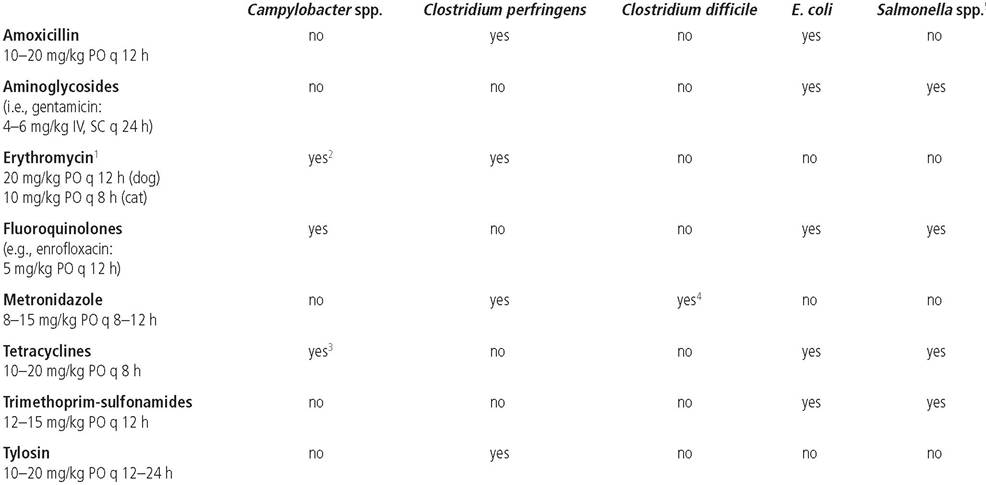
Figure 5.4: Histoplasma capsulatum. The image shows a single macrophage with several phagocytized Histoplasma organisms from a rectal scrape in a dog. Please note that only one of the phagocytized organisms (see arrow) shows the typical eccentric location of the nucleus (Wright's stain, 165x; image courtesy of Dr. Steve Gaunt, Louisiana State University, Baton Rouge, LA).
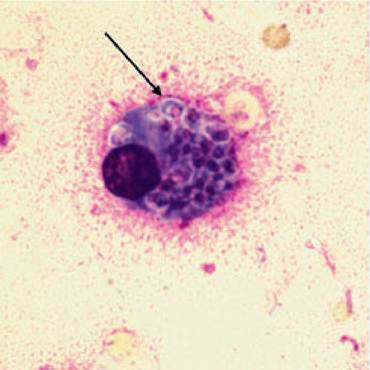
Figure 5.5: Pythiosis. This figure shows a histological image of the intestinal wall from an 18-month-old Boxer presented with a 1-month history of vomiting and weight loss. A jejunal mass was palpated on abdominal palpation and was surgically resected with a 15- to 20-cm piece of small intestine. The image shows three hyphal structures (two hyphal structures are marked by arrows), one of them septate (large arrow). A severe mixed inflammatory response with macrophages, granulocytes, and necrotic material in the background can be appreciated. The granulocytes were identified as eosinophils with H&E staining. An infection with Pythium insidiosum was diagnosed. (Immunohistochemistry with polyclonal anti-P insidi- osum antibody, 600x; image courtesy of Dr. Andrew David, Louisiana State University, Baton Rouge, LA.)
5.3.2.3 Fungal and algae infections 5.3.2.3.2 Pythiosis 5.3.2.3.1 Histoplasmosis Histoplasma capsulatum is a dimorphic soil-borne fungus that can be found throughout the world in temperate and subtropical climates. Infection occurs mostly in young dogs and cats through the inhalation or ingestion of microconidia. Localized H. capsulatum infection in dogs can affect the respiratory tract, but if the disease is disseminated, it typically involves the GI tract.44 Common signs include large-bowel diarrhea and tenesmus, hematochezia, and mucus in the feces. The small bowel may be infiltrated as well, with signs such as weight loss, intractable diarrhea, and sometimes protein-losing enteropathy (PLE). Histoplasmosis is most reliably diagnosed by identifying the organism on cytologic smears (Figure 5.4) from lymph node aspirates, rectal scrapings, or histological samples. Treatment consists of itraconazole (10mg/kg PO q 24 h), which should be continued for 4-6 months and at least 2 months beyond the resolution of clinical signs. 44 Pythiosis is caused by the aquatic pathogen Pythium insidiosum that belongs to the class Oomycetes. Large breed male dogs are affected most commonly, probably because of their increased risk of exposure. In some areas of the USA, the GI form of the disease predominates in the dog, while in other areas the skin form is more prevalent.45,46 The history can be suggestive of upper GI obstruction with a palpable abdominal mass or chronic diarrhea and weight loss, or sometimes also be suggestive of lower bowel disease. Histologically, eosinophilic granulomatous to pyogranulomatous enteritis can be found in the deep layers of the intestinal wall (Figure 5.5). The diagnosis is confirmed by isolation of the organism. Serology using ELISA or immunoblot has been shown to be very sensitive and specific. Antibody titers can be monitored during therapy and should significantly decrease in dogs that respond to treatment.45 However, the prognosis is poor, unless complete resection of the affected GI area is possible during sur- gery45,47 If resection is incomplete, medical therapy can be attempted with itraconazole (10 mg/kg PO q 24 h) and ter- binafine (5-10 mg/kg PO q 24 h), but treatment is not often successful.45
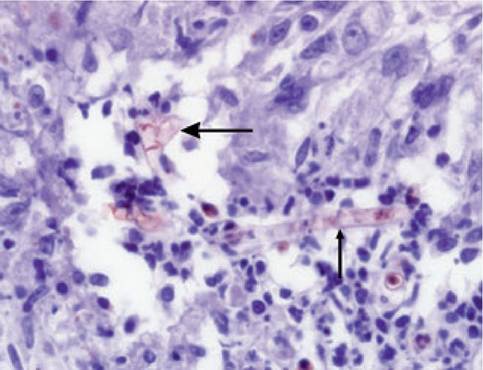
Figure 5.6: Helminths. This figure shows ova and adult helminths commonly found in fecal samples from dogs and cats. Upper left: Dipylidium canisegg; upper right: Echinococcus sp. egg; middle left: Ancylostomaegg; middle right: Ollulanus tricuspisadult; lower left: Toxascaris Ieonina egg; lower right: Toxocaraegg. 5.3.2.4 Parasitic diseases 5.3.2.4.1 Helminths Parasitism is common in both dogs and cats. All dogs with acute vomiting and /or diarrhea should be evaluated for parasites. The diagnosis of a helminthic infection is based on the demonstration of ova during fecal flotation (Figure 5.6). Several anthelminthics may be considered, with some being more effective than others for specific helminths (Table 5.5). Ces- todes, Taenia spp., and Echinococcus spp. are not very pathogenic in small animals, but can pose a significant zoonotic threat (especially Echinococcus infection in humans). Nematodes are more likely to cause clinical disease in dogs and cats. Ollulanus tricuspis The feline stomach worm is transmitted by infectious vomitus. These worms are usually located in the fundic area of the stomach in cats and may cause inappetence, vomiting, weight loss, and diarrhea.48 Ancylostoma caninum The hookworm, Ancylostoma caninum, causes significant disease in puppies in temperate climates. In subtropical areas, A. braziliense and A. ceylanicum may also infect the small intestine. Other hookworms such as Uncinaria spp. are mainly found in the colon, but can also sometimes cause small intestinal disease. After oral infection with Ancylostoma larvae, the parasite develops into the adult stage in the stomach and duodenum. The larvae can also penetrate into blood vessels and travel to the lungs, where they are coughed up and swallowed back into the GI tract. Percutaneous infections occur mainly in puppies. The larvae can travel to different organs, where they can persist in a hypobiotic state. These dormant stages can be reactivated during pregnancy and can then be secreted in the milk.49 Typical clinical signs in young puppies are blood loss, diarrhea, dehydration, PLE, and anemia. Effective anthelminthics are listed in Table 5.5. Milbemycin-oxime at 0.5-1 mg/ kg PO every 30 days may be used for chemoprophylaxis in areas with a high infectious pressure. Ascarids Toxocara canis and Toxocara mystax. Both of these parasites may cause significant disease in puppies and kittens, respectively. As is the case with hookworm infections, the parasite can travel from the wall of the GI tract into blood vessels and to the lungs or other organs and can also be transmitted through the colostrum. In fact, the lactogenic route is epide- miologically most important. Possible clinical signs include Table 5.5: Treatment for helminth infections. This table shows commonly used anthelminthic agents used for the treatment of helminth infections in dogs and cats
vomiting; diarrhea, sometimes with hematochezia and the presence of mucus in the feces; a distended and painful abdomen; dehydration; anemia and fever. In puppies, T canis infection may also cause clinical signs due to larval migration to different organs, and clinical signs due to pneumonia and /or hepatic disease may also be seen. Toxascaris leonina. Toxocara leonina causes small intestinal disease in dogs and cats. The development of the parasite occurs entirely in the intestinal tract. Clinically, enteritis can be seen, but the symptoms are rarely as severe as with Toxocara infections. Treatment options for ascarid infections are summarized in Table 5.5. Strongyloides spp. Strongyloides stercoralis and S. planiceps infect dogs, while S. felis and S. tumefaciens are seen in cats. Most infections are sub- clinical, but the presence of a high worm burden in puppies or kittens may be associated with hemorrhagic enteritis. 5.3.2.4.2 Protozoal infections The two main protozoal parasites affecting the intestinal tract in dogs and cats are Giardia spp. and Cryptosporidium spp. Recently, another protozoal organism, Tritrichomonas foetus (see
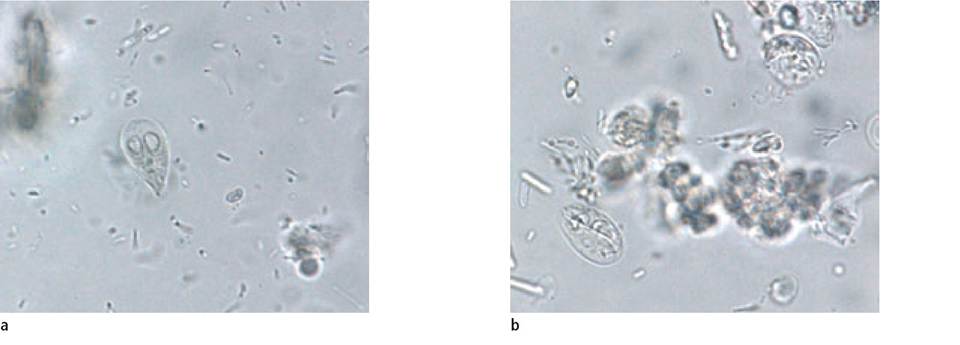
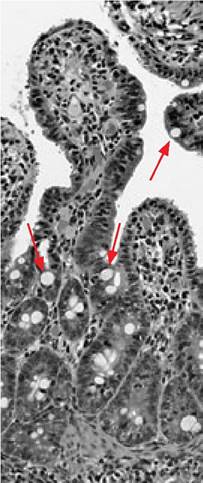
Figure 5.7: Giardia. a. Giardia trophozoite in a smear from canine feces. b. Giardia cysts in a fecal flotation specimen from a dog. (Images courtesy of Dr. Heinz Sager, Institute for Parasitology, University of Bern, Switzerland.) 6.4.2.3), has been described as a pathogenic organism in the GI tract in cats, but this organism mainly affects the large intestines. Giardia spp. Giardia duodenalis exists in two forms, a motile trophozoite of piriform to ellipsoidal shape with two nuclei, four pairs of flagella, and one pair of median bodies (Figure 5.7a), and a cyst form that is highly resistant in the environment (Figure 5.7b). The cysts are absorbed with contaminated food or water, and release trophozoites into the small intestinal lumen where they attach to the mucosal epithelium and cause disease by affecting epithelial permeability. Trophozoites multiply by cell division and become encysted in the large bowel. Giardia cysts have four nuclei, a thin envelope, and are surrounded by a convolute of flagella. Under favorable conditions, they can persist for 3 weeks or even longer in the environment.50 Giardia spp. are globally distributed and are responsible for approximately 280 million cases of human giardiasis per year worldwide.51 Symptoms of giardiasis in humans include acute or chronic diarrhea, dehydration, abdominal pain, and weight loss. Giardiasis is one of the most common parasitic diseases diagnosed in people living in North America. This protozoan is also encountered in dogs and cats, where the infection may remain subclinical, or may cause GI signs similar to those observed in humans. Consumption of water contaminated with Giardia cysts is the main origin of infection in people; however, the zoonotic potential of giardiasis in pets remains a subject of controversy. Giardia isolates are further divided into several different genotypes or assemblages with specific host ranges. Although assemblages infecting humans and pets are different, several anecdotal reports describe infections with similar genotypes in pets and people sharing a common environment.50 Several diagnostic tests are available for the diagnosis of Giardia infections in dogs and cats. These diagnostic tests include the direct examination of fecal smears for motile trophozoites (low sensitivity); concentration techniques including centrifugation with zinc sulfate (ZSFC), sodium acetate /acetic acid / formaldehyde (SAF), or merthiolate / iodine/formaldehyde (MIF) for detecting cysts (moderate to high sensitivity); fecal immunoassays such as ELISA or IFA for group specific antigens (moderate to high sensitivity); and fecal polymerase chain reaction (PCR; highly sensitive, but not recommended for routine diagnosis). Successful detection of Giardia using fecal flotation is operator-dependent. The retrieval of cysts significantly increases from 70% to more than 90% if two or more fecal samples collected at 2-3 days intervals are examined.52 The SNAP Giardia Test Kit (Idexx Laboratories) has a comparable accuracy to fecal immunoassays, and can be helpful for in-clinic screening of dogs with compatible clinical signs.53 Studies concerning the prevalence of giardiasis in the canine and feline population report different rates in healthy pets, pets presented for veterinary care, and cats and dogs kept in shelters. Using ZSFC, Giardia cysts were detected in 7.2% of dogs presented to a veterinary clinic in Canada.54 In another study, Giardia cysts were found in 12% of feline and 16% of canine fecal samples submitted to a laboratory in Germany.55 The frequency of fecal ELISA-positive cases in dogs from shelters in Rome, Italy, was reported to be between 21% and 74%.56 The prevalence is greatest in patients that live in high density group housing, especially when recommended disinfecting protocols are not carried out optimally. In such cases, Giardia cysts can easily survive in the environment and continuously infect new animals or re-infect animals after they have been treated. Several pharmaceutical agents have been successfully used for the treatment of giardiasis in dogs and cats. In dogs, metronidazole at 25-30 mg/kg PO q 12 h for 5-8 days and fenbenda- zole at 50 mg/kg PO q 24 h for 3 days are most commonly used.57 Albendazole (25 mg/kg PO q 12 h for 4 doses) can also be used successfully, but may lead to bone marrow toxicity in both dogs and cats.58,59 In cats, metronidazole benzoate given at a dosage of 25 mg/kg PO q 12 h for 7 days was well tolerated and eliminated cyst shedding within 7-10 days of treat- ment.60 Results of another study in cats about the use of fen- bendazole were less convincing.61 An increased rate ofresistance of Giardia spp. to metronidazole and other antigiardial agents has been reported in human patients. However, no published data concerning drug resistance in canine or feline giardiasis are currently available. Dogs kept in group housing should be removed from their runs, shampooed, and rinsed with quaternary-ammonium-based disinfectants. The runs should be cleaned and disinfected before reuse. Quaternary-ammonium- containing disinfectants have shown an excellent efficacy for inactivating Giardia cysts in a short period of time. Figure 5.8: Cryptosporidium parvum. This image shows small intestinal villi infected with Cryptosporidium parvum. The organisms can be seen on the immediate surface of the villi (see arrows). Cryptosporidium oocysts are difficult to see on direct fecal smears as they are translucent and very small. (H&E; image courtesy of Dr. Jody Gookin, North Carolina State University, Raleigh, NC.)
Vaccines against Giardia spp. are commercially available for dogs and cats in North America. The prophylactic efficacy of vaccination was shown in kittens and puppies, but routine vaccination is not recommended at this time.62 The vaccine may be useful in kennels and catteries with recurring infections. In some studies, investigators have attempted to use the vaccine therapeutically in infected dogs and cats. However, the results were not convincing, particularly in cats.63 Cryptosporidium spp. Cryptosporidium spp. are obligate intracellular parasites that infect enterocytes. The cycle of the parasite is complex and consists of asexual and sexual stages. Oocysts are produced during the sexual stage and enclose four sporozoites protected by a wall that is resistant to many environmental factors, but sensitive to desiccation and heat above 60 °C. Sporulated oocysts are passed with the feces and are infectious to appropriate hosts.64 In humans, immunocompetent people develop a selflimiting infection that typically lasts for 4-7 days, characterized by voluminous and watery diarrhea, possibly accompanied by other GI signs. The parasites are usually restricted to the lower small bowel. However, in immunocompromised patients, infections may spread throughout the whole bowel and become chronic and/or life-threatening. In a seroprevalence study conducted in cats from different regions of the USA, 8.3% cats were positive for Cryptosporidium. The lowest prevalence was in the mid-Atlantic states (1.3%) and the highest in the south-eastern region (14.7%).65 Prevalence rates between 0% and 38.5% (median 5.4%) have been reported in different feline populations, while prevalence rates reported in dogs were 0-44.8% (median 7.1%).66 As is the case in humans, cryptosporidial infections may be associated with diarrhea in dogs and cats. In some instances, chronic or intermittent diarrhea, anorexia, and weight loss may occur. However, in many cases, clinical signs go unnoticed. Several diagnostic tests for Cryptosporidium spp. are available and have recently evaluated in kittens.67,68 The oocysts are small (approximately 4-6 mm in diameter; Figure 5.8) and difficult to see in fecal preparations. When only one fecal sample was examined, two of the three investigated commercial enzyme immunoassays were the most sensitive (ProSpecT Cryptosporidium microplate assay, Remel Inc, Lenexa, KS and Premier Cryptosporidium enzyme immunoassay, Meridian Diagnostics Inc, Cincinnati, OH). However, when two consecutive fecal samples were examined, a modified Ziehl-Neelsen acid-fast stain was as sensitive as the immunoassays.67 In addition, a PCR-based test developed for the detection of Cryptosporidium spp. in cat feces has been shown to be more sensitive than the available immunoassays.68 In humans, most infections are water-borne, and many drinking-water-related outbreaks have been reported. However, most of the Cryptosporidium spp. are not strictly species-specific and zoonotic transmission involving pet dogs and cats may represent a serious risk to immunocompromised human patients.
Figure 5.9: Intestinal intussusception. Surgical image of a dog with a small intestinal intussusception following severe parvoviral infection. (Image courtesy of Dr. Bennito DeLaPuerta, Royal Veterinary College, London, UK.) Treatment consists of the administration of sulfonamides such as sulfadimethoxine (50 mg/kg PO q 24 h for 10-14 days) or a combination therapy of ormetoprim (11 mg/kg PO q 24 h) and sulfadimethoxine (55 mg/kg PO q 24 h), or trimetho- prim-sulfamethoxazole (30-60 mg/kg PO q 24 h for 6 days).72 The anticoccidial drugs toltrazuril (15 mg/kg PO q 12 h for 3 days) and diclazuril (25 mg/kg PO, single dose) are also effective in the treatment of Isospora spp. in kittens and puppies, although some animals may need to be re-treated 10 days after the initial therapy.73 5.3.2.4.3 Other protozoal parasites Cats are the definitive host for several other enteric protozoa such as Toxoplasma gondii, Hammondia spp., Besnoitia spp., or Sarcocystis spp. These protozoa are of low significance in feline medicine, but may be clinically relevant in intermediate hosts. In humans, nitazoxanide (NTZ), a nitrothiazole benzamide, appears to be the treatment of choice. NTZ was used in laboratory cats naturally infected with Cryptosporidium at a dosage of 25 mg/kg PO q 12 h. The drug caused vomiting and foulsmelling dark diarrhea. However, Cryptosporidium shedding resolved immediately after the NTZ treatment was initiated.69 Paromomycin (150 mg/kg PO q 12 to 24 h for 5 days in dogs and cats) has also been used in small animals. However, it has been reported to not consistently stop oocyst shedding, and was also associated with severe renal failure in cats.70 Coccidia Coccidial infections are more likely to occur in puppies and kittens than in adult dogs and cats. The general prevalence of coccidiosis in dogs is reported to be between 3% and 38%, and is highest in stray dogs.71 However, it is unclear if coccidia actually cause diarrhea under natural conditions in dogs, as most case reports describe concurrent viral or bacterial infections. Coccidia spp. found in dogs include Isospora canis and the I. ohioensis complex. In cats, between 3% to 36% of individuals are reported to excrete I. rivolta or I. felis oocysts, with the highest prevalence among stray cats. Coccidiosis is not thought to be a common clinical problem in cats. Also, cats develop immunity after infection with coccidia. The diagnostic test of choice for coccidia in dogs and cats is fecal flotation with Sheathers sugar solution. In coprophagic dogs, special attention must be paid to the possible presence of coccidia oocysts from other animals. 5.3.3 More on the topic Infectious causes of small intestinal disease:
-
Veterinarian -
| ||||||||||||||||||||||||||||