Insulinoma
Introduction
An insulinoma is a functional beta cell tumor causing hyper- insulinism. Insulinomas occur infrequently in dogs and are rare in cats.3-5 Insulinoma cells produce a wide variety of regulatory polypeptides, such as insulin, pancreatic polypeptide, somatostatin, glucagon, serotonin, gastrin, and ACTH.6 Despite the variety of polypeptides produced by insulinoma cells, almost all of the patients diagnosed with an insulinoma show only clinical signs of hyperinsulinism.
Insulinomas in humans are sometimes seen in concert with other endocrine neoplastic lesions, a condition known as multiple endocrine neoplasias (MEN). Recently, a cat with MEN has been described.5 This cat was diagnosed with a parathyroid gland adenoma, an adrenal gland cortical adenoma, and an insulinoma.Pathogenesis
The etiology of insulinomas remains unknown and risk factors for insulinomas have not been described. Beta cells take up glucose through an insulin-independent process and the intracellular glucose concentration of the islet cells mirrors the se-
Table 9.10: Gastrointestinal regulatory peptides
This table shows a list of the most prominent groups of gastrointestinal regulatory peptides. It should be pointed out that there are many more regulatory peptides in the gastrointestinal tract; however, their physiological relevance is less well understood.
| Regulatory peptide family | Members of regulatory peptide family |
| Gastrin-cholecystokinin family | ■ cholecystokinin ■ gastrin |
| Secretin/glucagon/vasoactive | ■ gastric inhibitory peptide (GIP) |
| intestinal polypeptide family | ■ glicentine ■ glucagon ■ glucagon-like peptide 1 ■ glucagon-like peptide 2 ■ growth hormone-releasing factor (GRF) ■ oxyntomodulin ■ peptide HI/HM ■ secretin ■ vasoactive intestinal polypeptide (VIP) |
| Pancreatic polypeptide family | ■ neuropeptide Y (NPY) ■ pancreatic polypeptide (PP) ■ peptide YY (PYY) |
| Tachykinin/bombesin family | ■ gastrin-releasing peptide (GRP) ■ GRP decapeptide ■ neuromedin B ■ neuromedin K ■ substance K ■ substance P |
| Opioid peptide family | ■ adrenocorticotrophic hormone (ACTH) ■ β endorphin ■ β neoendorphin ■ dynorphin ■ [leu]-enkephalin ■ Leumorphin ■ melanocyte stimulating hormone (MSH) ■ [met]-enkephalin |
| Insulin family | ■ insulin ■ insulin-like growth factor I |
| Epidermal growth factor | ■ epidermal growth factor |
| family | ■ transforming growth factor a (TGFa) |
| Somatostatin family | ■ somatostatin |
| Calcitonin family | ■ calcitonin ■ calcitonin gene-related peptide |
| Miscellaneous regulatory | ■ endothelin |
| peptides | ■ galanin ■ motilin ■ neurotensin ■ thyrotropin-releasing hormone (TRH) |

Figure 9.16:
Insulinoma.
This figure shows an insulinoma in a dog. Note the small size of the tumor. (Courtesy of Dr. Thomas J. Van Winkle, University of Pennsylvania, Philadelphia, PA.)rum glucose concentration. In normal subjects, insulin secretion from beta cells is suppressed when the blood glucose concentration falls below approximately 60 mg/dl. At the same time, secretion of the counterregulatory hormones (immediate response: catecholamines and glucagon; delayed response: cortisol and growth hormone) increases. Insulinomas do not respond appropriately to a falling blood glucose concentration. This results in hypoglycemia, which in turn can result in central nervous system (CNS) abnormalities. Glucose uptake into the CNS is by facilitated diffusion and is also non-insulin-dependent, so that glucose uptake is low at times of hypoglycemia. In addition, the CNS utilizes glucose as its primary energy source, and cannot utilize fatty acids and ketone bodies as can other tissues, including the peripheral nervous system. Clinical signs of hyperinsulinism also include signs induced by an increased discharge of the sympathetic nervous system, which is part of its counterregulatory response. However, insulinoma patients apparently adjust to repeated or chronic states of hypoglycemia as they can tolerate extremely low blood glucose concentrations without showing any clinical signs.
In addition to the degree of hypoglycemia, the rate of decrease in blood glucose concentration, and the duration of hypoglycemia all determine the extent of the clinical signs.
Table 9.11: Main functions of important gastrointestinal regulatory peptides
This table shows an alphabetical listing of the most important regulatory peptides of the gastrointestinal tract, their location and cell type of secretion, their most important functions, and the stimulatory and inhibitory factors for their secretion.
| Regulatory peptide | Location of secretion | Cell type | Most important functions | Stimulatory factors | Inhibitory factors | |
| cholecystokinin | duodenum, jejunum | I | ■ stimulation of pancreatic enzyme secretion ■ gallbladder contraction ■ regulation of pancreatic growth | ■ fat, fatty acids, proteins, amino acids, H+ ■ bombesin, GRP | ■ | somatostatin |
| gastric inhibitory polypeptide (GIP) | duodenum, jejunum | GIP | ■ inhibition of gastric acid secretion ■ stimulation of intestinal fluid secretion ■ stimulation of insulin release | ■ all major classes of nutrients in the gut ■ bombesin | ||
| gastrin | stomach, duodenum | G | ■ stimulation of gastric acid secretion ■ trophic effect on acid-secreting gastric mucosa ■ stimulation of pepsinogen secretion | ■ stomach distension ■ digested proteins and amino acids ■ bombesin, GRP, Ca++ | ■ ■ | luminal acidification somatostatin |
| glucagon | pancreas | A | ■ stimulation of glycogenolysis ■ stimulation of gluconeogenesis from lactate, amino acids, and glycerol | ■ hypoglycemia ■ high concentration of amino acids or low concentration of free fatty acids in plasma | ■ | hyperglycemia |
| insulin | pancreas | B | ■ stimulation of peripheral glucose uptake ■ stimulation of glycogen synthesis ■ stimulation of lipogenesis ■ stimulation of DNA, RNA, and protein synthesis | ■ hyperglycemia ■ glucagon | ■ | hypoglycemia |
| motilin | duodenum, jejunum | M | ■ initiates phase III of the migratory motor complex | ■ cyclic release during the fasting state ■ intraluminal lipids | ||
| neurotensin | ileum, colon | N | ■ inhibition of gastric acid secretion | ■ intraluminal lipids ■ bombesin | ||
| opioids | entire GI tract | ■ inhibition of intestinal water and electrolyte secretion ■ modulation of GI motility | ■ unknown | |||
| oxyntomodulin | ileum, colon | L | ■ inhibition of gastric acid secretion ■ stimulation of intestinal mucosal growth | ■ intraluminal glucose and lipids | ||
| pancreatic polypeptide (PP) | pancreas | F | ■ inhibition of pancreatic enzyme and fluid secretion | ■ intraluminal proteins ■ vagal stimulation | ||
| peptide YY | ileum, colon | L | ■ inhibition of pancreatic secretion ■ inhibition of gastric acid secretion ■ inhibition of gastric emptying | ■ intraluminal lipids ■ bombesin | ||
| secretin | duodenum, jejunum | S | ■ stimulation of pancreatic bicarbonate secretion | ■ duodenal acidification | ||
| somatostatin | entire GI tract | D | ■ inhibition of gastric and pancreatic secretions ■ inhibition of intestinal amino acid and glucose absorption ■ inhibition of intestinal motility | ■ intraluminal lipid, protein, and bile | ||
| tachykinins | entire GI tract | ■ regulation of GI motility ■ transmission of pain impulses | ■ luminal distension | |||
| vasoactive intestinal polypeptide (VIP) | entire GI tract | ■ relaxation of smooth muscle ■ vasodilation ■ stimulation of pancreatic and intestinal secretion | ■ vagal stimulation | |||
Table 9.12: Breed distribution of dogs with insulinoma
This table shows the breed distribution of 222 canine patients with insulinoma and the breed distribution of the canine population seen at the Veterinary Hospital at the University of Pennsylvania (VHUP) for the period 1991-1992.3 Boxers, Irish Setters, German Shorthaired Pointers, and Weimeraners appear to be predisposed.
The 222 cases compiled were seen at several different veterinary institutions. Thus, the hospital population of VHUP is not a statistically valid reference population and the percentages are shown in parentheses.| Breed | Number of dogs | % of all cases of insulinoma | % of VHUP population |
| Mixed Breed | 62 | 28.6 | (26.5) |
| Boxer | 21 | 9.7 | (1.2) |
| German Shepherd | 18 | 8.3 | (6.6) |
| Irish Setter | 17 | 7.8 | (0.6) |
| Golden Retriever | 10 | 4.6 | (4.9) |
| Miniature Poodle | 9 | 4.1 | (2.5) |
| Labrador | 8 | 3.7 | (6.2) |
| German Shorthaired Pointer | 7 | 3.2 | (0.4) |
| Collie | 6 | 2.8 | (0.9) |
| Standard Poodle | 6 | 2.8 | (1.1) |
| Weimaraner | 6 | 2.8 | (0.4) |
| West Highland WhiteTerrier | 6 | 2.8 | (0.8) |
| Basset | 5 | 2.3 | (0.8) |
| Other breeds | 36 | 16.6 | (47.1) |
(Table re-printed with permission from: Steiner JM, Bruyette DS.
Canine insulinoma. Compend Contin Educ Pract Vet 1996; 18: 13-24.)Pathology and natural behavior
Insulinomas most commonly appear as tan nodules in the pancreas (Figure 9.16). They are generally small (i.e., 1 cm in diameter or less). Most often they appear to be singular, but in a series of 129 dogs, 14% had multiple masses.3 On histopathology, the tumor cells appear as normal islet cells, forming irregular nests and cords with a variable pattern of dense stromal proliferation.
Malignant tumors are defined as tumors which are locally invasive and /or form distant metastasis. In many neoplastic diseases, the malignant potential of a tumor can be successfully predicted by histopathological evaluation. However, this is not the case for insulinomas and other endocrine neoplasias, as these neoplasias often lack many of the typical features of malignancy. Thus, estimation of the malignant potential of insulinomas based on histopathological findings can be misleading and should not be attempted.
Signalment
Insulinomas mainly occur in older dogs and cats. The mean age of 233 dogs reported in the literature was 8.9 years with a range of 3.5 to 14 years in 128 dogs.3 The sex distribution of 133 dogs with insulinoma showed 45% males and 55% females.3 Table 9.12 shows the breed distribution of 222 dogs with insulinoma.3
Table 9.13: Incidence of clinical signs reported in 113 canine insulinoma patients3
| Clinical Sign | Number of patients | % of patients |
| seizures | 77 | 68 |
| collapse | 38 | 34 |
| generalized weakness | 37 | 33 |
| posterior weakness | 37 | 33 |
| depression / lethargy | 21 | 19 |
| ataxia | 21 | 19 |
| muscle fasciculation | 20 | 18 |
| bizarre behavior | 17 | 15 |
| polyphagia | 12 | 11 |
| exercise intolerance | 11 | 10 |
| shaking / trembling | 11 | 10 |
| polyuria / polydipsia | 8 | 7 |
| weight gain | 7 | 6 |
all other clinical signs were reported with a frequency of less than 5%
(Table re-printed with permission from: Steiner JM, Bruyette DS.
Canine insulinoma. Compend Contin Educ Pract Vet 1996; 18: 13-24.)Clinical presentation
Dogs presenting with insulinomas generally present with two types of clinical signs: neuroglycopenic signs, such as weakness, ataxia, depression, or seizures or signs related to an increased discharge of the sympathetic nervous system, such as behavioral changes, shaking, trembling, and muscle fasciculations.3,4 The incidence of clinical signs reported in 113 dogs with insulinoma is shown in Table 9.13.3 Most patients with insulinoma show only intermittent clinical signs, and will have a rather unremarkable physical examination. A few patients will present in status epilepticus or even comatose. Due to the age of the affected population, a number of geriatric abnormalities may be evident that are unrelated to the presence of an insulinoma. Rather rare are those patients presenting with peripheral polyneuropathies. Subclinical polyneuropathy appears to be more common than symptomatic disease.
Diagnosis
A fasting blood glucose concentration should be part of the workup of a patient with clinical signs suggestive of hypoglycemia, preferably during times when the patient is sympto-
matic. Most dogs diagnosed with an insulinoma will present with a low blood glucose concentration, even in the absence of clinical signs. If hypoglycemia is confirmed, the causative relationship between the observed clinical signs and the hypoglycemia needs to be established. This is best accomplished by demonstrating Whipple’s triad, which consists of 1) demonstrating a subnormal blood glucose concentration, 2) presence of clinical signs of hypoglycemia, and 3) cessation of clinical signs with resolution of hypoglycemia. After Whipple’s triad has been established, the cause of hypoglycemia must be identified. A basic workup should include a complete blood count, a chemistry profile, and a urinalysis. In insulinoma patients these basic parameters will usually be within normal limits.
Infrequently reported abnormalities include mild elevations in liver enzymes. Radiographs of the thorax and abdomen are usually within normal limits, but may be helpful to exclude other causes of hypoglycemia. Abdominal ultrasound is a valuable tool in patients with suspected insulinoma. Even though only a small percentage of insulinomas can actually be visualized by this method, it is very helpful for assessing the patient for the presence of organ metastasis or mesenteric lymphadenopathy.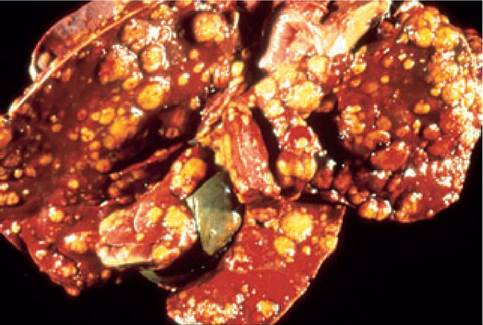
Figure 9.17:
Insulinoma metastases in the liver. This figure shows a liver with diffuse dissemination of metastatic lesions of an insulinoma in a dog. (Courtesy of Dr. Thomas J. Van Winkle, University of Pennsylvania, Philadelphia, PA.)
Many tests have been employed in human and veterinary patients with a suspected insulinoma. The single most reliable test for an insulinoma is the demonstration of an inappropriately high serum insulin concentration in the face of hypoglycemia, also referred to as insulin-glucose pair. Serum for the determination of insulin concentration needs to be collected at the time of the hypoglycemia. This is accomplished by serial blood glucose measurements while food is withheld from the animal. It is best to start early in the morning with the patient being closely monitored throughout the day. Blood glucose concentration is measured every 30-60 minutes. When the blood glucose falls below 60 mg/dl, a sample for the measurement of serum insulin concentration is drawn and the animal is fed. It is important to verify blood glucose concentrations measured by a glucometer through the use of a chemistry analyzer. Interpretation of the insulin-glucose pair is straight forward if the insulin concentration exceeds the reference range (the reference range is dependant on the laboratory used) in the face of hypoglycemia. However, the serum insulin concentration may be within the reference range and still be inappropriately high with respect to the blood glucose concentration. Several ratios have been evaluated to help document inappropriate insulin secretion: glucose-insulin ratio, insulin-glucose ratio, and the amended insulin-glucose ratio. Unfortunately, none of these ratios improve the diagnostic accuracy in either humans or dogs with a suspected insulinoma and the use of these ratios is not recommended. An insulin- glucose pair is the single most reliable test to diagnose an insulinoma as the cause of hypoglycemia.
A variety of provocative tests have been suggested to aid in the diagnosis of an insulinoma. These include the glucagon tolerance test, the IV glucose tolerance test, the tolbutamide tolerance test, the L-leucine test, the oral glucose tolerance test, the epinephrine stimulation test, and the calcium infusion test. All of these tests are time consuming, expensive, and, at least in people, have lower sensitivities than a simple insulin-glucose pair. In addition, some of these tests put the patient at risk for severe hypoglycemia. In cases where the cause for the hypoglycemia can not been determined, and the evaluation of serum insulin and glucose concentrations have been equivocal, the measurement of serum insulin and glucose should be repeated whilst food is withheld from the patient.
Staging
As with any other neoplastic disease, patients with an insulinoma should be staged. Unfortunately, the available modalities to stage canine and feline insulinoma patients are limited. Abdominal ultrasound is inconsistent in detecting the primary tumor, but can be helpful in demonstrating evidence of local extension and distant metastasis of the disease. Currently, the most reliable staging tool in veterinary patients appears to be abdominal exploration.
In a compilation of 129 abdominal exploratories of canine insulinoma patients, 66 (51%) of the dogs had metastatic disease detected during the exploratory laparotomy.3 Of those, 29 (22%) had metastatic lesions in the liver (Figure 9.17), 19 (15%) had metastases to regional lymph nodes, 7 (5%) had metastatic lesions in both liver and lymph nodes, and 11 (8%) had metastatic lesions in other locations.3
Treatment
Emergency treatment
Patients presenting for clinical signs of hypoglycemia need to be treated as quickly as possible. If hypoglycemia has been documented, a dextrose bolus (0.5 g/kg as a 25% solution IV over approximately one minute) should be administered and a dextrose constant rate infusion should be initiated. Suitable infusion solutions are 5% dextrose or balanced electrolyte solutions with added dextrose. It is important to note that the goal of emergency therapy is to eliminate the clinical signs of hypoglycemia rather than to restore euglycemia. If neurogly- copenic signs persist, cerebral edema should be suspected and treatment using mannitol and corticosteroids should be considered. If seizures still persist, diazepam or other anticonvulsants may be indicated.
Pancreatic surgery
Surgical exploration is the treatment of choice for the management of canine and feline patients with an insulinoma. It is crucial to stabilize the blood glucose concentration of the patient prior to surgery. Also, the surgeon should be aware that handling of the tumor can lead to increased insulin release. In contrast, removal of the tumor may suddenly lower plasma insulin concentrations. Therefore, blood glucose must be monitored closely throughout the procedure.
In order to stage the disease, a careful abdominal exploratory should be performed, and biopsies of suspicious lymph nodes or areas within the liver should be obtained.
Identification of the insulinoma can be difficult. In a compilation of 129 abdominal exploratories of canine patients with a suspected insulinoma, a pancreatic nodule could not be identified in 26 patients (20%).3 Even though some of these cases might have had a rarely described diffuse infiltration of the pancreas, further evaluation of localization techniques seems warranted in canine insulinoma patients. Some investigators have suggested the intravenous infusion of methylene blue.7 However, this procedure has only been described in five patients and the drug can cause a Heinz body hemolytic anemia, so further investigation of this technique is necessary. In human medicine, a variety of localization techniques have been described and compared. Currently, endoscopic ultrasonography and somatostatin receptor scintigraphy (SRS) are considered the most sensitive modalities in human insulinoma pa- tients.8 Othermodalitiesinclude intraoperativeultrasonography, CT, MRI, selective arteriography, intraoperative quick frozen sections, and transhepatic venous sampling.
The majority of localization techniques reported in the human literature are either very expensive or of limited availability in veterinary medicine. Thus, intraoperative inspection and palpation remain the primary mode of localization of an insulinoma in veterinary patients. However, other modalities may be employed. Intraoperative ultrasonography is technically feasible and relatively inexpensive, but has never been systematically evaluated for the localization of insulinomas in small animals. However, the author believes that it should be considered in cases where intraoperative visualization and palpation are unsuccessful. It also can be utilized to scan the liver for possible metastasis. The use of CT has recently been evaluated for the localization of insulinomas in dogs and was able to visualize the primary tumor in 10/14 (71%) patients.9 This was superior to transabdominal ultrasound, which was successfully used to identify the primary tumor in 5/14 (36%).9
Somatostatin receptor scintigraphy, that is the intravenous administration of 111In-DTPA-D-Phe1-octreotide (OctreoScan, Mallinckrodt Medical) followed by planar scintigraphy or single-photon emission CT, has also been evaluated in canine insulinoma patients.9-11 In one study, the primary lesion was identified in all five dogs evaluated.10 However, in two other studies the insulinoma was only identified in 6/14 (43%) and 4/17 (24%) dogs.9,11 This discrepancy can be explained by the fact that the tumor was positive for somatostatin receptor subtype 2 (sst2), one of the somatostatin receptor subtypes to which octreotide preferentially binds to, in all five dogs in the first study, but only in 7/17 (41%) dogs in one of the other two studies.10,11 Thus, while SRS may be useful to identify and /or localize an insulinoma in some cases, if the tumor does not express sst2, the tumor may not be able to be visualized with this modality.
Extreme care should be exercised at all times when handling the pancreas. After localization of the insulinoma, it can be removed by enucleation, partial pancreatectomy, and total pancreatectomy +/- duodenectomy. While the surgical technique for total pancreatectomy has been described for the dog, this procedure is associated with a high postsurgical morbidity and mortality, and should thus only be considered if there are no other options. Local enucleation has been shown to result in shorter survival times than partial pancreatectomy, and should therefore only be considered if the tumor is in the body of the pancreas, or very proximally in the right lobe.12 Thus, the surgical procedure of choice is partial pancreatectomy (Figure 9.18). If the tumor cannot be localized on abdominal exploratory, a small pancreatic biopsy should be taken to evaluate the pancreas for diffuse infiltration histopathologi- cally. Since the right and left lobes are involved with equal frequencies and occult insulinomas are probably most common in the pancreatic body, random removal of pancreatic tissue should not be performed.
The most common postoperative complication of pancreatic surgery is acute pancreatitis. However, the risk of postoperative pancreatitis can be minimized by aggressive fluid therapy during anesthesia and gentle handling of the pancreas during surgery. Other common postoperative complications are hypoglycemia and hyperglycemia. Persistent hypoglycemia indicates that the insulinoma has not been completely removed. The patient either has to be re-explored, or medical therapy has to be instituted. Hyperglycemia, if present, is most often transient, but some patients may require insulin therapy to control the hyperglycemia.
Chemotherapy
If surgical exploration is not an option or if it does not lead to removal of the entire insulinoma, chemotherapy can be considered. Streptozotocin is a nitrosurea compound isolated from Streptomyces achromogenes. The drug has been used in approximately 20 dogs with insulinoma.13,14 Streptozotocin is highly nephrotoxic and can also be hepatotoxic. Therefore, pre- and post-treatment diuresis is crucial. In addition, the mean duration of normoglycemia in treated dogs was not significantly longer than in untreated controls in one study of 17 dogs. Thus, further studies are needed to evaluate the clinical usefulness of streptozotocin for the treatment of canine insulinoma.
Alloxan is an unstable uric acid derivative that has two effects, selective cytotoxicity of islet cells and stimulation of hepatic gluconeogenesis. The use of alloxan has been described in five canine insulinoma patients.15 Two of the five patients developed hyperglycemia for several months without any additional medical therapy. Alloxan, like streptozotocin, is also nephrotoxic and concurrent fluid therapy should be instituted for several days in order to minimize renal toxicity. The use of several other chemotherapeutic drugs has been reported in the human literature, but no data are available for veterinary species.
Radiation therapy
Successful treatment of insulinomas with radiation therapy has been described in isolated human patients. However, to date, data for canine or feline patients are not available.
Symptomatic therapy
Antihypoglycemic therapy
Symptomatic therapy should be instituted in insulinoma patients when surgical exploration is not an option or is not successful. The dog should be fed a high protein, high fat, high complex carbohydrate diet divided into multiple small feed-

Figure 9.18:
Insulinoma. An insulinoma after surgical removal by partial pancreatectomy. Size and appearance of this tumor are typical. (Re-printed with permission from Steiner JM, Bruyette DS. Canine insulinoma. Compend Contin Educ Pract Vet 1996; 18: 13-24.)
ings (4-6 per day). If the patient shows signs of weakness, a small amount of food should be offered immediately. Owners should also be familiarized with the clinical signs of hypoglycemia and instructed that if signs occur, dextrose solution (e.g., Karo-Syrup or honey) should be applied onto the gums of the patient. Excitement should be avoided and exercise should be limited to short leash walks.
Glucocorticoids should be administered if frequent feedings alone will not control the clinical signs. Cortisol is an endogenous counterregulatory hormone to insulin. It increases peripheral lipolysis and protein catabolism, increases hepatic gluconeogenesis and glycogenolysis, and decreases peripheral glucose utilization. It also decreases the sensitivity of insulin receptors in the periphery. Prednisone or prednisolone can be started at an oral dose of 0.25 mg/kg twice a day. If clinical signs of hypoglycemia cannot be controlled, the dose can be increased up to 2-3 mg/kg twice per day. The development of iatrogenic Cushing’s and GI side effects (e. g., gastritis, gastric ulceration, or colitis), may warrant the discontinuation of steroid therapy, and additional medical therapy may be required.
Antihormonal therapy
Another therapeutic option for insulinoma patients is the treatment with agents that depress insulin secretion. Several such agents are available. Diazoxide is a non-diuretic benzothiadiazine that has anti-hypertensive as well as hyperglycemic properties. Its hyperglycemic action is due to a depression in
insulin release from beta-cells. Diazoxide does not impair insulin synthesis and it is not cytotoxic to beta cells. Survival times in insulinoma patients treated with diazoxide are rather short. However, this might be due to the fact that in most reports, diazoxide was only administered after previous medical and surgical therapy had failed. A few long-term responders have been reported, the longest being 18 months.16 The recommended starting dose is 5 mg/kg orally twice per day, but the dose can be gradually increased to 30 mg/kg twice a day. Since the drug is metabolized in the liver and excreted by the biliary system and the kidneys, dosing should be carefully evaluated for patients with hepatic or renal disease. Also, care should be taken to avoid hyperglycemia. Thiazide diuretics enhance the effects of diazoxide and hydrochlorothiazide can be added to the therapeutic protocol (2-4 mg/kg PO q 24 h). In order to decrease the frequency of GI side effects, the drug should be administered together with a meal.
Somatostatin (i.e., octreotide acetate) decreases several polypeptides of the gastroenteropancreatic system, including insulin. Octreotide consistently suppresses plasma insulin concentrations in canine insulinoma patients, while it has no effect on counterregulatory hormones, suggesting that it maybe useful in the treatment of canine insulinoma.17 However, of approximately 20 dogs described in the literature that have been treated with octreotide only 50% showed a clinical response.11,18 As with SRS, the limited response of canine insulinoma patients to octreotide may be due to a lack of sst2 expression of the insulinoma cells. Doses of 20-100 μg octreotide SC q 8-12 h have been described in the literature.11,18
Prognosis
The long-term prognosis for dogs with insulinoma is grave, although the short-term prognosis is good. In a compilation of 114 dogs with an insulinoma, which had been treated with surgery and with symptomatic therapy after recurrence of clinical signs, the mean survival was 11.5 months.3 Results may be more favorable as 31 dogs were alive and asymptomatic at their last follow-up visit, and time to relapse or death could not be determined. It should also be noted that the mean age of dogs presenting with an insulinoma is 9 years, and therefore many patients may die for other reasons. In one study, the mean survival of canine insulinoma patients without metastatic disease at the time of diagnosis was 17 months, while it was only 8.4 months for dogs that did have metastatic disease.19 Thus, detection of distant metastases at the time of the abdominal exploratory may serve as a prognostic indicator. Age and serum insulin concentrations at the time of diagnosis have also been proposed as prognostic indicators, but supportive data are not available.19
9.4.3