Gastrinoma
Introduction
A gastrinoma is a rare tumor in small animals, having been reported in only 25 dogs and 5 cats, compared to approximately 250 dogs and four cats with an insulinoma.20-22
Gastrinomas are most commonly single nodules of small size (Figure 9.19).
However, multiple masses have also been reported. In humans, gastrinomas are ultimately malignant, but most grow slowly. When gastrinomas were first described in humans, most were localized in the pancreas, but to date over 50% of gastrinomas in humans have been found outside the pancreas, with most of those being found in the duodenum.23 This is probably due to improved localization techniques. By sharp contrast, gastrinomas have not been localized in the duodenum in either dogs or cats, although tumors could not be accurately located in many cases. Recently, a bile duct carcinoma in a cat was shown to stain positive for gastrin.24Gastrinomas synthesize and release excessive quantities of gastrin (Figure 9.20), leading to gastric acid hypersecretion, hypertrophy of the gastric mucosa, and eventually gastric and duodenal ulceration (Figure 9.21).23,25 Persistent hyperchlor- hydria also leads to a decrease in duodenal pH, which in turn leads to mucosal injury and inactivation of digestive enzymes with subsequent maldigestion.
Clinical presentation
Gastrinomas usually develop in middle-aged to older dogs (age range 3.5-12 years in 21 dogs reported) and cats (age range of five reported cats: 8-12 years).22 In dogs, females are anecdotally more commonly affected than males (69% vs. 31%), but this may be a reflection of the small number of cases reported.
The most common clinical signs observed in 25 of the reported cases included vomiting (92%), weight loss (88%), anorexia (72%), lethargy (64%), and diarrhea (60%).
In addition, polydipsia, melena, and abdominal pain were noted in approximately 25%, and hematemesis, hematochezia, fever, and ravenous appetite in approximately 10% of cases each. Clinical signs in cats are similar with vomiting, weight loss, and poor body condition being reported most consistently.Figure 9.19:
Gastrinoma. This figure shows a small tumor (arrow) in the pancreas of a dog. This tumor is barely visible and was identified as a gastrinoma by immunohistochemistry. (Courtesy of Dr. Kenneth W. Simpson, Cornell University, Ithaca, NY.)
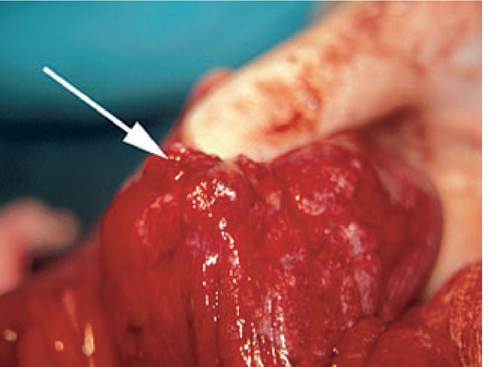
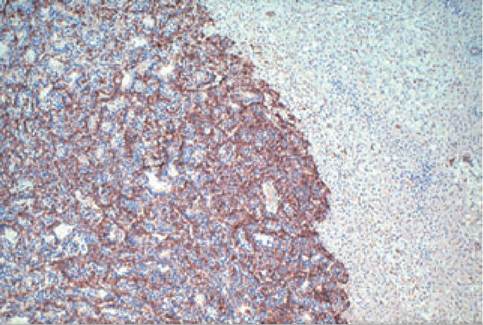
Figure 9.20:
Immunohistochemistry of a gastrinoma. This image shows a pancreatic tumor that was stained for gastrin. Note the massive degree of brown staining on the left side of the picture. The brown stain shows the presence of gastrin, identifying this pancreatic tumor as a gastrinoma. (Courtesy of Dr. Kenneth W. Simpson, Cornell University, Ithaca, NY; magnification: 10?.)

Figure 9.21:
Duodenal perforated ulcer. This figure shows a perforated ulcer in the duodenum of a dog. This dog was diagnosed with a pancreatic tumor that stained positive for gastrin, identifying it as a gastrinoma. (Courtesy of Dr. Kenneth W. Simpson, Cornell University, Ithaca, NY.)
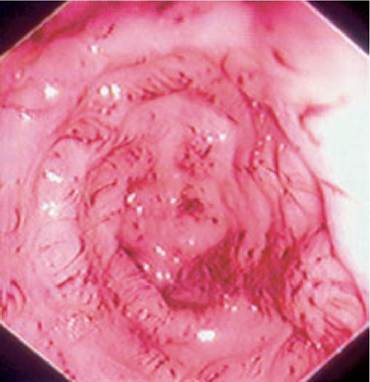
Figure 9.22:
Esophageal ulceration. This image shows an endoscopic view of severe ulceration of the distal esophageal mucosa in a dog with a gastrinoma. (Courtesy of Dr. Kenneth W. Simpson, Cornell University, Ithaca, NY)
Routine laboratory tests do not reveal any specific changes, but up to 50% of affected dogs and cats have a regenerative anemia, indicating ongoing blood loss.
Many patients also show a neutrophilia with a left shift. Hypoproteinemia with hypoalbuminemia, hypokalemia, increased serum hepatic enzyme activities, hypochloremia, and hyperglycemia are also common. More serious changes may occur if complications, such as pyloric obstruction due to mucosal hypertrophy, or ulcer perforation with peritonitis occur.Survey abdominal radiographs are unremarkable in most cases. Upper GI contrast radiography, which is rarely performed these days, may reveal plaque-like defects in the stomach or duodenum, indicating ulceration. In the small number of dogs described, abdominal ultrasonography failed to locate the primary lesion, but abdominal ultrasound may be useful for identifying metastatic lesions. Of the five cats diagnosed with a gastrinoma, two were evaluated by transabdominal ultrasound and in one of these cases the tumor was identified during a repeat ultrasound examination.22 Gastroduodenoscopy allows for direct visualization of esophageal (Figure 9.22), gastric, and duodenal lesions, but cannot identify the underlying cause of these lesions. In human gastrinoma patients, sensitivities and specificities of different localization techniques for gastrinoma have been compared. Abdominal ultrasonography, CT, MRI, or selective angiography all have a rather low sensitivity for the diagnosis of the primary lesion.23 However, these modalities are all useful in identifying metastatic lesions. Much more promising for localization of the primary lesion are endoscopic ultrasonography and SRS, which successfully identify the primary lesion in almost all human patients. SRS is the most sensitive technique for localization of both the primary tumor and metastatic lesions in human gastrinoma patients.23 Currently, endoscopic ultrasonography is not routinely available in veterinary practice. The diagnosis of a gastrinoma by SRS using 111In-DTPA-D-Phe1-octreotide (OctreoScan, Mallinckrodt Medical) has recently been reported in a single dog.26
Diagnosis
Although rare, gastrinomas should be ruled out in all patients with a history of chronic vomiting, weight loss, anorexia, or diarrhea when an alternative diagnosis cannot be arrived at.
Also, a gastrinoma should be considered in patients with severe peptic ulcer disease without any predisposing risk factors.A definitive diagnosis of gastrinoma, short of histopathological confirmation, is difficult. A species-specific assay for gastrin is not available, but several assays developed for use in humans have been validated for dogs and cats.27 Few veterinary laboratories currently offer serum or plasma gastrin measurements (current reference range for dogs: 10-40 ng/L). According to the diagnostic recommendations for humans, a presumptive diagnosis of a gastrinoma can be made when the 24-hour fasting serum gastrin concentration is ten times the upper limit of the reference range. This recommendation is rather conservative and reflects the high prevalence of chronic atrophic gastritis in humans, which can cause severely elevated serum gastrin concentrations in humans. In dogs and cats, differential causes of elevated serum gastrin concentrations are chronic renal failure, gastric outlet obstruction, small intestinal resection, immunoproliferative enteropathy of Basenji dogs, gastric dilation/volvulus, and administration of proton-pump inhibitors. All of these differential diagnoses are considerably more easy to rule out than atrophic gastropathy in humans.2 Therefore, in dogs and cats, a less than 10-fold elevation of serum gastrin concentration may be sufficient to diagnose a gastrinoma if other differential diagnoses have been carefully ruled out.
In cases where serum gastrin concentrations are less markedly elevated, provocative testing may be useful. Secretin can be injected intravenously at a dose of 2 U/kg after withholding food from the patient for a 24-hour period. Blood samples are collected at 0, 2, 5, 10, 15, and 20 minutes. An increase of serum gastrin concentration to greater than 200 ng/L or a twofold increase of the serum gastrin concentration at any time point is considered diagnostic for a gastrinoma.20 Alternatively, calcium is administered intravenously at a dose of 5 mg/kg/h, followed by serial measurements of serum gastrin concentrations at 0, 15, 30, 60, 90, and 120 minutes.
A two-fold increase at any time point is diagnostic for a gastrinoma. In humans, thecalcium challenge test is less sensitive than the secretin challenge test.
Treatment
Symptomatic therapy is started in most cases before a definitive diagnosis can be established and should be continued for several weeks after definitive therapy. The mainstay of symptomatic treatment of human gastrinoma patients are protonpump inhibitors. The proton-pump inhibitor omeprazole has also been successfully used in the management of canine and feline patients with a gastrinoma (0.7 mg/kg PO q 24 h).20,22,28 Initially, sucralfate, a mucosal protectant that adheres to the exposed proteins of the ulcer, should be added to the treatment protocol (1 g per dog PO q 8 h; 0.25-0.5 g per cat PO q 8 h). Histamine2 antagonists, such as ranitidine or famotidine, at double the standard dose are used if omeprazole is ineffective. Octreotide, a long-acting somatostatin analogue, acts by inhibiting gastrin release and by decreasing gastric acid secretion directly and may inhibit tumor growth, thus affording more than just symptomatic relief. It has been used successfully in two canine gastrinoma patients (2-20 μg∕kg SC q 8 h).18,20 These two dogs survived for 10 and 14 months, respectively, compared to a reported mean survival time of
5.5 months for other dogs with gastrinoma.20
Before initiating definitive treatment, the patient should be staged, which involves the localization of the primary lesion and the search for metastatic disease. Metastatic lesions serve as a long-term prognostic indicator, and approximately 85% of all dogs and cats with a gastrinoma have metastatic disease at the time of diagnosis. After localization of the primary tumor and after widespread metastatic disease has been excluded, an exploratory laparotomy should be performed. Even if the primary tumor can be identified easily, the rest of the pancreas and abdominal cavity should be carefully inspected for additional primary or metastatic lesions.
This should include careful palpation of the duodenum. If a primary lesion cannot be identified, intraoperative ultrasonography or illumination of the duodenal wall with an endoscope may be useful. In cases where a primary lesion can still not be identified, biopsy samples of pancreas, lymph nodes, and the liver should be collected. Some authors have recommended partial pancreatectomy of the right lobe of the pancreas if a primary lesion can not be identified, as 60% of all gastrinomas in small animals have historically been identified in the right lobe and only 7% in the left lobe of the pancreas.2 However, this statistic is based on only 15 dogs and may not reflect the true localization distribution.If the primary tumor can be identified, it is removed by partial pancreatectomy. The tumor should be submitted for histopathological examination and immunohistochemical staining for regulatory peptides most commonly found in GI NETs. Metastatic lesions, which are present in most cases, should only be removed if this is possible without radical excision. Postoperatively, the patient should not be given anything per os for 24 to 48 hours, followed by the gradual re-introduction of water and an easily digestible low-fat diet.
If the primary tumor cannot be localized and removed during surgery or if extensive metastatic disease is present, an alternative therapeutic approach should be considered. The use of chemotherapy has not been reported in dogs or cats with a gastrinoma and it has a low success rate in human patients. Radiation therapy using OctreoScan® has been successfully used in humans with a response rate of up to 50%, but has not been attempted in veterinary species.23 Also, medical therapy as described above may prove useful.
Prognosis
The long-term prognosis for dogs and cats with a gastrinoma is grave. However, with appropriate medical management the short-term prognosis and quality of life can be good. Several canine and feline gastrinoma patients have been successfully managed for more than 1 year after diagnosis.22 With increasing awareness leading to earlier diagnosis, improved localization and staging techniques, and advanced treatment options, survival times are likely to increase further.
9.4.4