Interventionalprocedures
1.5.9.1 Foreign body removal
Esophagus
Esophageal foreign bodies (FB) can often be removed with flexible equipment.19,25 However, the use of a rigid colono- scope and rigid forceps is superior to flexible endoscopy in many cases.26 The length of the rigid scope is the major limiting factor.
Fortunately, most dogs with esophageal FB are small to medium-sized. Plain radiographs are taken immediately before endoscopy to look for pneumothorax, pneumomediastinum, or pleural effusion, which may all be indicators for esophageal perforation (contrast procedures are rarely appropriate). The rigid endoscope is carefully advanced to the FB. Although not obvious, the edges of the FB will often have eroded into the mucosa. Thus, simply pulling on the FB can cause perforation. Instead, the operator must gently manipulate the FB so that the edges are no longer caught in the erosions before pulling with any force. In the case of bones (especially poultry bones), one can advance the scope until the tip of the scope is putting slight pressure against the bone. One may then use the rigid grasping forceps to grasp the bone, pull it snugly against the end of the rigid endoscope, and then tear off pieces or break it, thus facilitating removal. Once the FB is freed from the erosions, it may be pulled partially or completely inside the scope while being removed, thus protecting the rest of the esophagus and making it easier for the remaining fragments to be pulled through the cricopharyngeal sphincter.Fishhooks can often be removed, depending on the size of the barb and the location of the hook.19,27 Small barbs can easily be torn out of the mucosa with a rigid scope, but hooks with large barbs often cannot. If the hook has passed completely through the esophagus, it can still be removed endoscopically by tearing it back out of the esophagus, as long as the hook is not in the vicinity of any important vessels.
If the point of the hook is directed caudally, then the bend of the hook is tightly grasped with rigid forceps, and the hook is pulled cranially while keeping the hook as straight as possible. If the point of the hook is directed cranially, a rigid scope is passed until the edge of the scope is against the bend of the hook. The eye of the hook is grasped with the forceps so as to keep the shaft of the hook straight, and then the scope and forceps are pushed about 1 cm further into the esophagus. This action will push the hook out of the esophageal mucosa.In some cases when a FB cannot be removed, it may be pushed into the stomach, where it can either be removed or, in the case of bones, allowed to dissolve.19,26 This must only be done if one can be certain that there are no sharp edges on the FB, as pushing a FB with sharp edges may lead to esophageal perforation. In the case of a textured FB (e.g., racket ball), one may need to apply lubrication around the FB so that it can be pushed through the LES.
The operator should be extremely careful when insufflating air during endoscopic removal of an esophageal FB. If one causes gastric distension by insufflating air into the esophagus but one cannot enter the stomach with the scope, one may have to trocharize the stomach to relieve the pressure. Also, insufflating too much air may cause a severely ulcerated esophagus to rupture and produce a tension pneumothorax. In any case, a lateral thoracic radiograph should always be taken after removing an esophageal FB that has caused deep ulceration to look for evidence of pneumothorax as a sign for perforation. If the esophagus is severely diseased, endoscopic placement of a gastrotomy tube may also be valuable.
Stomach and intestines
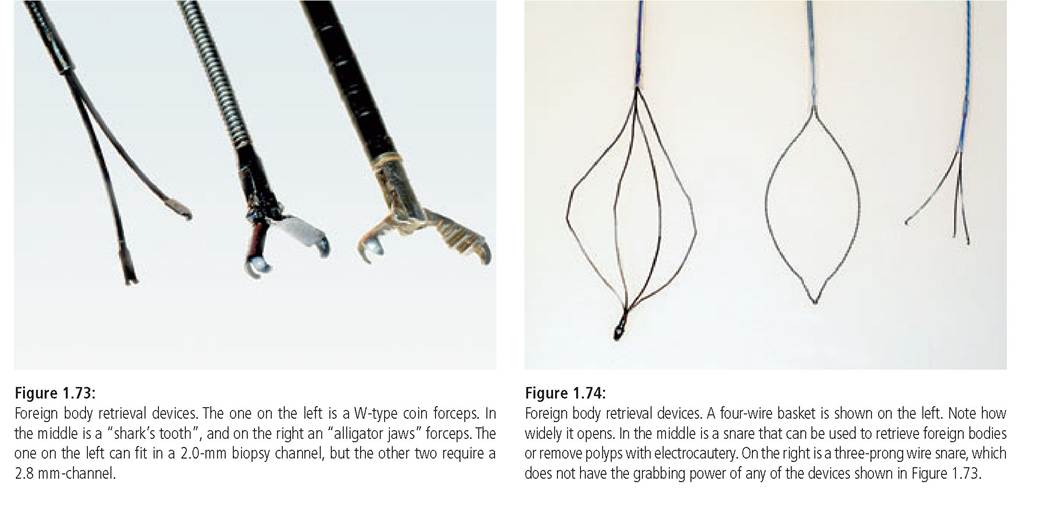
It is important to have several good FB retrieval devices.25 Some of the more useful devices require a 2.8-mm working channel (i.e., shark’s tooth, alligator jaws; Figure 1.73), although some fit through a 2.2-mm channel (i.
e., W-type coin forceps). A W-type coin forceps is useful for many objects besides coins. Objects that create a lot of resistance when being pulled across the mucosa require obtaining a substantial “grip” in order to remove them, and a “sharks tooth” and /or an “alligator jaws” forceps allows perhaps the most tenacious hold possible (Figure 1.73). A four-wire basket is very useful for balls and rocks. However, the wires should be very soft and pliable, and must open widely (i. e., at least 2 cm) in order to reliably snare most FB (Figure 1.74). A simple snare is also useful. Three wire graspers are often supplied with endoscopes, but are poor substitutes for the preferred instruments (Figure 1.74).When a FB is located, it should first be studied in order to consider the best way to remove it. Pulling a FB through the LES is usually the most difficult task, and one must carefully decide which side should be grasped and pulled into the esophagus first. Objects with sharp points should be grasped so that sharp points or edges are oriented away from the mouth. It sometimes helps to a) partially deflate the stomach and b) gently rotate the scope as one is pulling the object through the LES.
An overtube can also be helpful for removing FBs.25 The endoscope is passed through the larger diameter overtube. After snaring a sharp FB, one may pull the endoscope and the sharp FB into the overtube, thus protecting the esophagus. Additionally, because the overtube is larger than the endoscope, one may also use it to dilate the LES more than the endoscope alone would. By opening the LES those few additional millimeters, one may be able to pull a FB through the LES that would not otherwise pass. Also, administering ketamine or xy- lazine will relax the LES, which sometimes helps to pull a FB through the LES.
Linear foreign bodies
Linear FB, which have lodged at the pylorus and trail down the duodenum present a particular challenge.
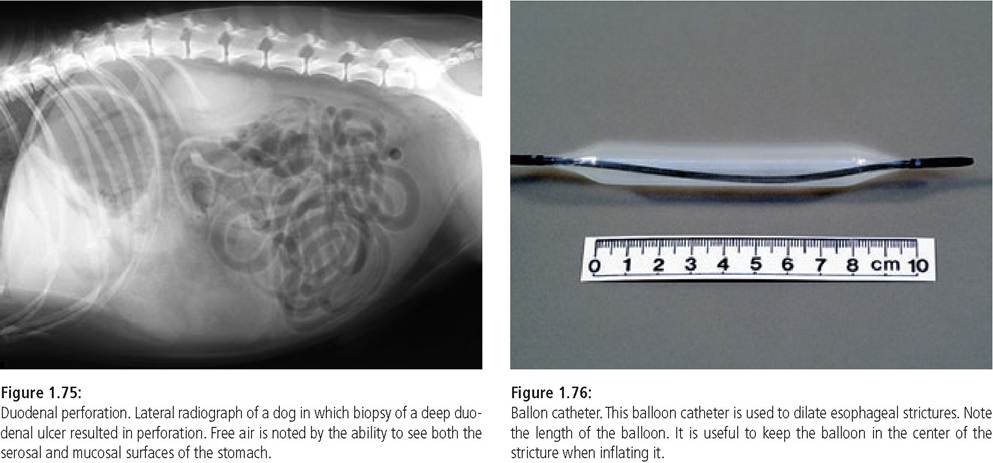
In the author’s experience, about 20% of these linear FB can be removed via endoscopy. First, the duodenum should be entered. Then the endoscope tip should be carefully advanced to as near the end of the FB as possible. This can be very tedious, and may require the endoscope tip to repeatedly be advanced and pulled back. The goal is to grab the FB as near the distal (i. e., aborad) end as possible and then pull it out of the duodenum and into the stomach. In rare cases, one may be able to push the orad end of the linear FB (which has lodged at the pylorus) into the duodenum. Doing this often alleviates the problem because a linear FB only causes a problem if one end is lodged (usually at the base of the tongue or at the pylorus) and the rest is trailing off into the intestines. Because of the risk for perforation, one should perform a lateral abdominal radiograph after endoscopically removing a linear FB to look for free air as evidence for perforation (Figure 1.75).1.5.9.2 Percutaneous gastrostomy tube
There are many techniques for placing percutaneous endoscopic gastrostomy tubes (PEG tubes), including devices that do not require endoscopy. Endoscopy is advantageous as PEG tubes can easily be placed incorrectly (i. e., too near the LES or too far caudally) or the mesentery or other organs can be damaged or impaled when using “blind” devices.
1.5.9.3 Dilation of esophageal strictures
Benign esophageal strictures can be dilated using either bougienage or balloon dilation.19,20 It has been suggested that balloon dilation is associated with less shearing effects and therefore causes less unnecessary trauma, but studies in humans have shown that both bougienage and balloon dilation are effective if the operator is well trained. To date, balloon dilation is performed more commonly in small animals and will thus be discussed here. One needs to have balloon catheters specifically designed for this purpose. Round balloons as found on Foley catheters and endotracheal tubes do not work well for this purpose.
Balloons of catheters designed for this purpose are long (Figure 1.76), making it easier to position the middle of the balloon at the stricture so that the balloon will not migrate as it is being inflated. First, a transfer wire is placed through the endoscope and the stricture. Then, the endoscope is removed while the wire is held in place by continually feeding it into the scope as the scope is removed. Next, the endoscope is replaced into the esophagus so that the stricture can be visualized with the transfer wire running alongside the scope. An over-the-wire balloon catheter is passed down over the wire and through the stricture, so that the stricture is at the middle of the balloon. First, a small diameter balloon is chosen and then the size is progressively increased for repeated ballooning. The balloon is maximally inflated for a few seconds. If the stricture is being torn, the patient typically shows increased heart or respiratory rates and some bleeding. How much to dilate the stricture is debatable and is a matter of personal choice. The goal is not necessarily to restore the esophagus toits former size, but rather to make the patient able to consume regular or softened food. For most cats and small dogs, 15- to 20-mm balloons provide more than adequate dilation.
It is important to avoid causing excessive trauma in order to prevent restricturing. When aspirating blood and fluid from the esophageal lumen, one should be careful not to also aspirate strips of esophageal mucosa. The more esophageal mucosa that is damaged, the more likely is a reformation of a stricture. Some patients are permanently cured after one ballooning procedure. However some patients, especially those with concurrent esophagitis or with very dense, mature strictures, have recurrent strictures, and repeat ballooning procedures are necessary. Anywhere from 1 to 20 ballooning procedures may be needed, but most patients require with 16 different biopsy forceps designed for upper gastrointestinal endoscopy.
Gut 1985;26:227-231.12. Woods KL, Anand BS, Cole RA et al. Influence of endoscopic biopsy forceps characteristics on tissue specimens: results of a prospective randomized study. Gastrointest Endoscop 1999; 49: 177-183.
13. Jergens AE, Moore FM. Endoscopic biopsy specimen collection and histopathologic considerations. In: Tams TR (ed.), Small Animal Endoscopy, 2nd ed. Philadelphia, Mosby, 1999; 323-340.
14. Mansell J, Willard MD. Biopsy of the gastrointestinal tract. Vet Clin NAm 2003; 33: 1099-1116.
15. Willard MD, Lovering SL, Cohen ND et al. Quality of tissue specimens obtained endoscopically from the duodenum of dogs and cats. J Am Vet Med Assoc 2001; 219: 474-479.
16. Wilcock B. Endoscopic biopsy interpretation in canine or feline enterocolitis. Sem Vet Med Surg 1992; 7 (2): 162-171.
17. Willard MD, Jergens AE, Duncan RB et al. Interobserver variation among histopathologic evaluations of intestinal tissues from dogs and cats. J Am Vet Med Assoc 2002; 220: 1177-1182.
18. Hall JA, Watrous BJ. Effect of pharmaceuticals on radiographic appearance of selected examinations of the abdomen and thorax. Clin Rad 2000; 30: 349-375.
19. Gualtieri M. Esophagoscopy. Vet Clin N Am 2001; 31: 605-630.
20. Sellon RK, Willard MD. Esophagitis and esophageal strictures. Vet Clin N Am 2003; 33: 945-967.
21. Melendez LD, Twedt DC, Weyrauch EA et al. Conservative therapy using balloon dilation for intramural, inflammatory esophageal strictures in dogs and cats: a retrospective study of 23 cases. Eur J Com Gastroenterol 1998; 3: 31-36.
22. Leib MS, Dinnel H, Ward DL et al. Endoscopic balloon dilation of benign esophageal strictures in dogs and cats. J Vet Intern Med 2001; 15: 547-552.
23. Leib MS, Saunders GK, Moon ML et al. Endoscopic diagnosis of chronic hypertrophic pyloric gastropathy in dogs. J Vet Intern Med 1993;7:335-341.
24. Peterson PB, Willard MD. Protein-losing enteropathies. Vet Clin N Am 2003; 33: 1061-1082.
25. Tams TR. Endoscopic removal of gastrointestinal foreign bodies. In: Tams TR (ed.), Small Animal Endoscopy, 2nd ed. Philadelphia, Mosby, 1999; 247-295.
26. Houlton JEF, Merrtage ME, Taylor PM et al. Thoracic oesophageal foreign bodies in the dog: a review of ninety cases. J Small Anim Pract 1985; 26: 521-536.
27. Michels GM, Jones BD, Huss BT et al. Endoscopic and surgical retrieval of fishhooks from the stomach and esophagus in dogs and cats 75 cases 1977-1993. JAm Vet Med Assoc 1995; 207 (9): 1194-1197.
28. Kochhar R, Makharia GK. Usefulness of intralesional triamcinolone in the treatment of benign esophageal strictures. Gastrointest Endoscop 2002; 56: 829-834.
1.6