Appearance of the upper gastrointestinal tract
The normal esophagus has a smooth texture, except in the cat where the distal esophagus has a ribbed texture where the striated muscle is replaced with smooth muscle.1,7 Black pigment is usually visible in Chow Chows or Shar Peis.
The LES may have a reddened area protruding slightly into the esophageal lumen, which is normal. The stomach should have a smooth texture.2 One may see numerous dots on the mucosa in some patients. The duodenum has a definite, fine texture due to the villi.3 One can typically see the duodenal papilla (Figure 1.57) as well as depressions that represent lymphoid follicles (Figure 1.58). When using a video endoscope the examiner can often appreciate individual villi.1.5.8.1 Abnormal findings
Esophagus
Although endoscopy may help to detect a grossly distended esophagus (i.e., megaesophagus), endoscopy is often a poor diagnostic tool for the diagnosis of esophageal weakness.7 Only patients with marked esophageal dilation will be obvious during endoscopy; fluoroscopy is a much more sensitive (and less invasive) way to diagnose esophageal weakness. Also, some preanesthetics (e. g., ketamine or xylazine) can cause the esophagus, stomach, and intestines to become flaccid.18

Figure 1.60:
Esophagitis. Note obvious areas of hyperemia.
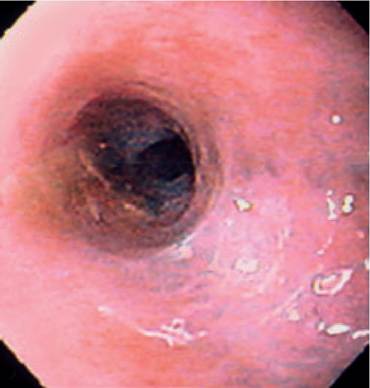
Figure 1.61:
Esophageal stricture. Note the narrowing of the lumen and the white tissue (scar tissue) at the 4-o'clock position.
Some esophageal tumors present as distinct masses while others cause strictures.7,19 Sarcomas may be caused by Spirocerca lupi. Spirocerca lupi granulomas appear as nodules with some having a small “crater” or “nipple” from which a red worm may occasionally protrude.
Sarcomas, carcinomas, and melanomas are all easily diagnosed by biopsy. Leiomyomas are typically submucosal and are covered with normal mucosa (Figure 1.59). It is often impossible to diagnose these tumors with flexible endoscopic forceps because such forceps cannot cut through the stratified esophageal mucosa. In some cases leiomyomas at the LES may only be visible through the retroflexed position from inside the stomach. Finally, esophageal polyps are rare, and if found may represent an underlying malignancy that has produced a benign, adenomatous growth over it. A deep biopsy (i.e., surgical or performed with a rigid biopsy forceps) that includes the submucosa is necessary for diagnosis.Esophagitis is usually obvious; the operator can find a roughened, hyperemic, bleeding mucosa (Figure 1.60).19,20 Care should be taken to not further damage the esophagus by excessive or rough endoscopic technique. The esophageal mucosa may be biopsied in order to confirm the diagnosis. Rare patients may have fungal infections. The clinician should always seek to identify the cause of esophagitis, and carefully examine the stomach and intestines in affected patients for concurrent lesions. Hiatal hernias are sometimes responsible and may be obvious or occult at endoscopy. Obvious hiatal hernias can have a wide opening at the LES with gastric mucosa protruding into the opening. However, not all patients with a hiatal hernia have esophagitis.
Strictures secondary to esophagitis are usually obvious (Figure 1.61).21,22 They may occur anywhere, but are more common near the LES. Larger animals may have their esophageal lumen decreased by ≥75% and still allow the endoscope to easily pass through it. Strictures adjacent to the LES may be mistaken for the LES, especially if the endoscope readily passes through it.
Stomach
Many animals with moderate to severe gastritis have a grossly normal appearing gastric mucosa. Therefore, the gastric mucosa should be biopsied in any vomiting or anorexic patient undergoing gastroduodenoscopy.
Most gastric lesions are not uniformly distributed throughout the entire gastric mucosa; therefore, one must carefully inspect and biopsy the entire gastric mucosal surface.7 Any food or water in the stomach should be aspirated, and hairballs or other foreign material removed so that the entire mucosal surface can be examined. If blood is present, one should aspirate as much as possible so that all bleeding lesions may be identified and more closely examined. The operator can also infuse water into the stomach through the tip of the endoscope to help wash out the stomach. The inside of the pylorus is perhaps the hardest place to adequately visualize, but ulcers and Physaloptera organisms are sometimes found there.
Figure 1.62:
Gastric tumor. This is a leiomyoma on the greater curvature of the stomach.

Figure 1.63:
Antral mucosal hypertrophy. Endoscopic view of a dog's pyloric area. The pylorus is obscured by a mass. This lesion is non-neoplastic and represents antral mucosal hypertrophy.

Figure 1.64:
Neoplastic ulcer. Endoscopic view of a large ulcer near the LES. This is a neoplastic ulcer caused by a scirrhous carcinoma. It was not possible to diagnose this tumor with an endoscopic biopsy because the tissue was too tough and dense to collect a biopsy from it.
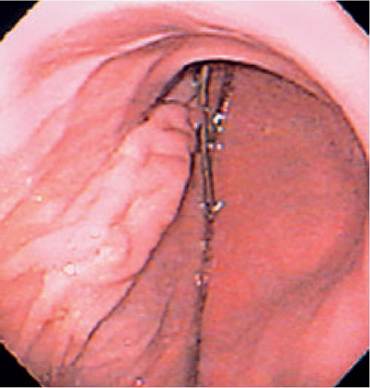
Figure 1.65:
Greater curvature and antrum. Endoscopic view of the greater curvature and entrance to the antrum with an incision line extending into the antrum. The incision line is raised and could be mistaken for an infiltrative lesion.
Tumors can cause obvious proliferations (Figure 1.62).
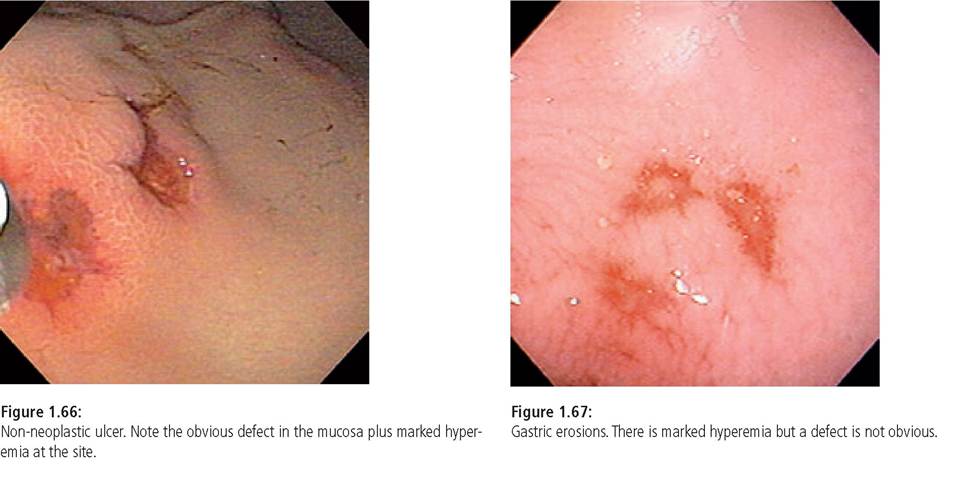
However, gastric antral mucosal hypertrophy (Figure 1.63) and benign gastric polyps can closely mimic their appearance.23 Tumors can also cause mucosal ulcerations without any obvious pro liferation (Figure 1.64). Lymphosarcoma is usually easily diagnosed by collection of biopsies with flexible biopsy forceps, but scirrhous tumors, leiomyomas, or pythiosis may be impossible to diagnose with flexible biopsy instruments. Prior gastric surgery can be seen as an elongated mucosal mass that could be mistaken for a tumor (Figure 1.65). Sometimes areas which have diffuse submucosal infiltrates are detected because they remain collapsed and cannot be distended by air insufflation - this may be more obvious in the gastric antrum.Ulcers and erosions can be surprisingly easy to miss. Digested blood is dark brown-black and absorbs light, making it difficult for the operator to critically examine the mucosa. Also, debris often accumulates on top of erosions or ulcers, making the aspiration of debris necessary. Unless the stomach is adequately distended, erosions and ulcers can also be hidden in between rugal folds. Ulcers are deep mucosal defects that often are discolored (Figure 1.66), while erosions are hyperemic areas, which sometimes can be seen to have a minor mucosal defect (Figure 1.67).2 Healed ulcers may cause a “stellate” appearance in which “rays” seem to radiate out from a central flat area. Submucosal hemorrhage (Figure 1.68) may be caused by coagulopathies or may signify areas of ulcer formation. Linear gastric lesions can be caused by over-inflating a diseased stomach or pushing an endoscope into the stomach wall with too much pressure.
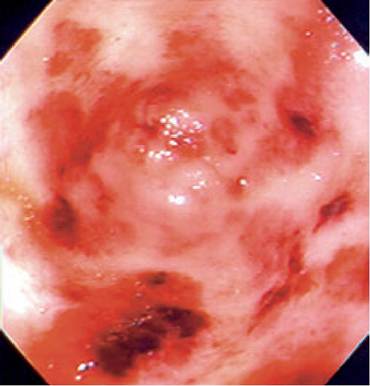
Figure 1.68:
Submucosal hemorrhage. Endoscopic view of submucosal hemorrhage. This lesion was caused by a coagulopathy, but could also represent a site that will soon ulcerate.
Rarely, a previously unsuspected, non-distended gastric torsion will be diagnosed when the endoscopist cannot find the entrance to the antrum.
Duodenum
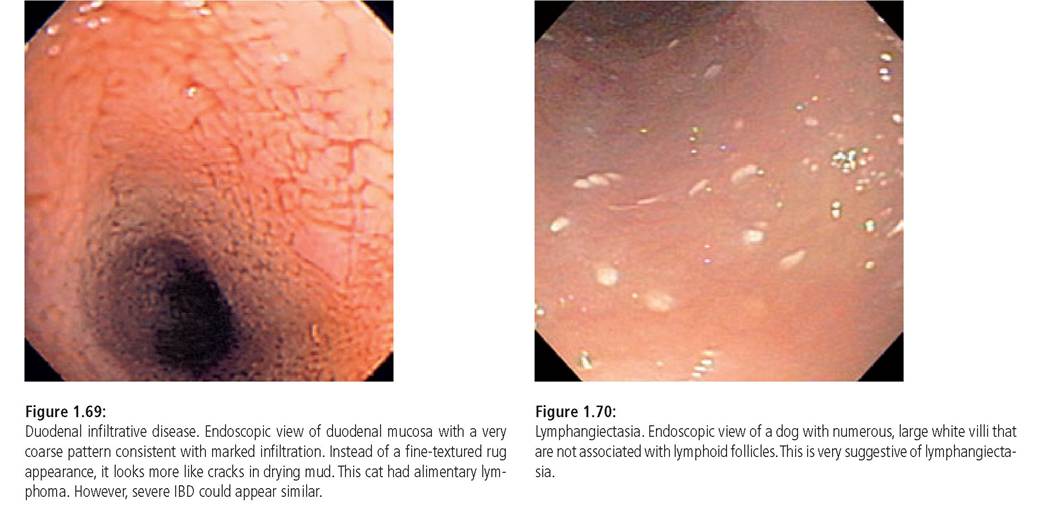
The duodenal mucosa typically has a fine texture. Infiltration can cause the texture to be coarser, and severe infiltrates may cause the mucosa to resemble dried mud with cracks (Figure 1.69). Duodenal ulcers may have obvious craters or may appear as focal areas of exudate or spots of hemorrhage. Large, deep ulcers that occur near the pylorus may represent damage due to excessive gastric acid secretion. Extensive, eroded areas can have a smooth appearance, due to lack of villi. Areas of hyperemia may indicate infiltration, erosion, or coagulopathy. Masses and strictures may be obvious, although sometimes the only hint of a focal infiltrative lesion (e.g., tumor or fungal granuloma) is a roughened section of mucosa that does not smooth out when the rest of the bowel distends. However, the operator must ensure that such findings are not due to inadequate insufflation.
Finding large white dots scattered over the mucosa (Figure 1.70) is suggestive of lymphangiectasia.24 The white dots represent dilated lacteals and are different from the generalized, delicate, fine textured white villi that can be seen in any normal animal that has recently had a fatty meal. Large white lacteals are often seen in the area of lymphoid follicles, but are not diagnostic of lymphangiectasia. Finding a substantial amount of white froth in the duodenum during and after biopsy also suggests lymphangiectasia because biopsying disrupts dilated lymphatics, allowing chyle to escape into the lumen.
Colon
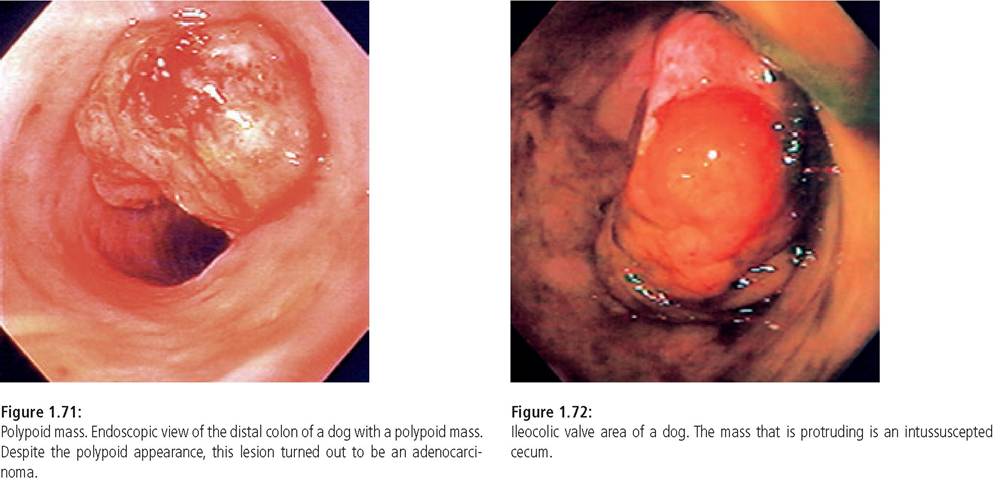
Occasionally areas of obvious colonic inflammation (e. g., histoplasmosis, pythiosis) or ulceration are seen (e.g., histiocytic ulcerative colitis). However, most of the dramatic colonic lesions are seen near the anus, where tumors and polyps are most common (Figure 1.71).4 Tumors are occasionally seen further up the colon. One cannot distinguish benign polyps from malignant tumors based upon gross appearance alone. Sometimes, polyps can be multiple and small, resembling inflammatory disease. Occasionally, unsuspected whipworm infestation is noted. Intussusception of the ileum or cecum into the colon can occasionally be found (Figure 1.72).
1.5.9