Intestinal tumors in cats
Background
Adenocarcinoma is by far the most common non- hematopoietic tumor of the intestinal tract in cats; sarcomas are rarely described. Intestinal adenocarcinoma is more common in cats than in dogs.
The majority of intestinal adenocarcinomas occur in the small intestine of affected cats. The ileum or jejunum is most often affected, whereas the duodenum is rarely involved. Adenocarcinoma of the large intestine is less common and usually involves the colon, although the cecum and rarely rectum may be affected.Intestinal adenocarcinoma primarily affects old cats; the mean age of affected cats is 10 to 11 years, although they may be as young as 2 years of age. The vast majority of affected cats are Siamese, which constitute 152 (68%) of 225 reported cases. Other purebreds are rarely affected. In one study all 22 adenocarcinomas of the large intestine occurred in domestic short hairs, although no other study addressed this association. Cats with colonic adenocarcinoma typically are older, with a mean age of 16 years.There seems to be no gender predilection for intestinal adenocarcinoma with the exception of one report in which male cats predominated. Feline leukemia virus (FeLV) is unlikely to play a role in this disease. Only two studies reported the FeLV status of affected cats; all 28 cats studied tested negative for FeLV antigenemia.
Although benign tumors of the intestinal tract are rare and the duodenum is not usually affected, 18 cats with adenomatous polyps of the duodenum have been described. Signalment was similar to that in cats with adenocarcinoma in that older, primarily Oriental-breed cats are most often affected. The cats in this study were predominantly castrated males. Most cats were tested for FeLV and feline immuno-
deficiency virus (FIV), and all had negative results.
All polyps occurred within 1 cm of the pylorus.For colonic neoplasia in particular, one study found that adenocarcinoma followed by lymphoma, mast cell disease, and neuroendocrine carcinoma were the most common tumors found in this location.
Clinical Parameters
The most common presenting clinical signs for cats with alimentary lymphoma are as follows: vomiting, diarrhea, and interestingly a large portion of cats will present with only weight loss and anorexia. Some cats actually have increased appetite because of poor absorption of nutrients through the tumor of the intestinal tract. Most cats have a palpable abdominal mass. The World Health Organization’s classification scheme for lymphoma appears in Table 11-6.
The most frequent presenting signs in cats with intestinal adenocarcinoma reflect involvement of the proximal small intestine. In decreasing order of frequency, vomiting, weight loss, and anorexia predominate. Hematochezia is occasionally described in cats with colonic or rectal tumors. Clinical signs often have been present for a considerable time (median, 2 months, but up to 2 years). Cats with tumors involving more proximal intestinal tract tend
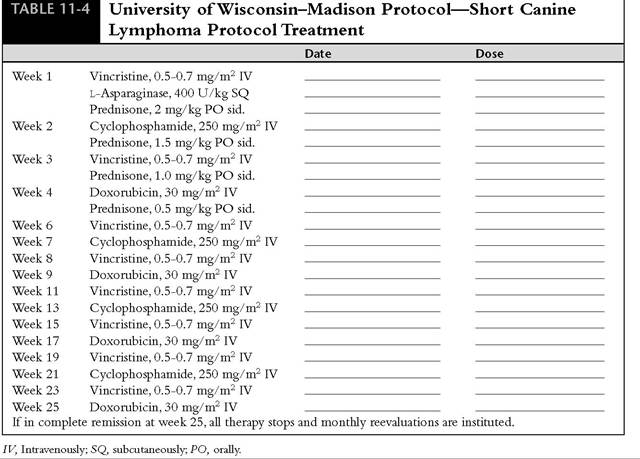
TABLE 11-6
World Health Organization’s Classification for Lymphoma
Stage I. Involvement limited to a single node or extranodal site, or lymphoid tissue in a single organ, including cranial mediastinum and excluding bone marrow
Stage II. Involvement of many lymph nodes in a regional area, a resectable gastrointestinal tract tumor or extranodal site with regional lymph node involvement
Stage III. Generalized lymph node involvement, nonresectable intraabdominal disease or epidural tumor
Stage IV. Liver and/or spleen involvement associated with stages I-III
Stage V. Manifestation in the blood and involvement of bone marrow involvement with stages I-IV Each stage is subclassified into:
a.
Without systemic signs, orb. With systemic signs to present more rapidly (1 month) than cats with tumors of the lower small intestine (3.5 months) or large intestine (4.5 months), presumably because owners more easily perceive the clinical signs of vomiting and anorexia.
On physical examination, affected cats with intestinal tumors are often cachectic and usually dehydrated and an abdominal mass is frequently palpable. Peritoneal carcinomatosis is common and may produce marked ascites.
Cats with intestinal mast cell tumors have a history of vomiting, diarrhea, and anorexia.These cats usually have a palpable abdominal mass that can be localized with ultrasound and rarely have circulating mast cells.
Cats with duodenal adenomatous polyps usually present with a history of acute or chronic vomiting.Vomitus will contain blood only in the acutely affected cat.
Clinical Work-up
In addition to survey abdominal and thoracic radiography, cats with intestinal tumors should have abdominal ultrasonography performed, because metastatic disease is usually abdominal. A complete blood count and biochemical panel, urinalysis, viral serologic study, bone marrow aspiration (lymphoma and mast cell disease), and biopsy of lymphomatous tissue (lymphoma) should be performed on all cats with suspected intestinal tumors.
Intestinal adenocarcinomas in cats spread by intramural (rather than intraluminal) extension and thus generate an annular (“napkin ring”) constriction rather than a mass lesion. Constriction of the intestinal tract causes obstruction. Abdominal radiographs may confirm the presence of a palpable abdominal mass, and plain or barium contrast radiographs may reveal evidence of obstruction of the small intestine (Figure 11-11). Osseous metaplasia may cause the intestinal tumor to mineralize. Endoscopy may help identify lesions of the upper intestinal tract (although duodenal tumors are rare) or of the rectum and colon. Ultrasonography provides a simple and reliable method to perform a biopsy on intestinal tumors in cats, as well as to image abdominal structures for evidence of metastasis.
Because of the localized and obstructive nature of the lesion, however, exploratory laparotomy followed by a resection and anastomosis is often both diagnostic and therapeutic.Ascites from peritoneal metastases is common, and cytologic examination of ascitic fluid may reveal malignant cells. Different histopathologic descriptions have been used to classify intestinal adenocarcinomas as tubular, mucinous, or undifferentiated, but the prognostic significance of these subclassifications is negligible. All types have a high metastatic rate.
Metastasis occurs to the peritoneum, mesentery, omentum, and regional lymph nodes in approximately 50% of affected cats with intestinal adenocarcinoma. Less common sites of metastasis are the liver, spleen, uterine stump or uterus, urinary bladder, and other areas in the intestinal tract. Metastasis to the lung is rarely reported.
Cats with suspected mast cell disease or lymphoma should have a similar staging regimen performed. Both of these diseases warrant bone marrow evaluation, as well as a similar work-up as described for adenocarcinoma. Retroviral status should always be evaluated. On thoracic radiographs it may be possible to appreciate a mediastinal mass or pleural effusion. Lymphadenopathy, GI thickening,and hepatomegaly may be observed on abdominal ultrasound. Ultrasound-guided biopsy, particularly in cats with GI tract involvement of lymphoma, has proven to be efficacious in obtaining diagnostic samples. Endoscopy can be used to obtain superficial biopsy specimens and is diagnostic in many cases. However, surgical full-
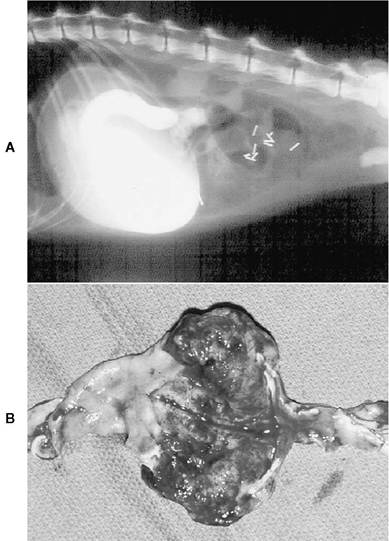
FIGURE 11-11 Intestinal adenocarcinoma in a cat. A, Radiograph of a cat with explosive vomiting of short duration.A biochemical profile revealed hypochloremia, hypokalemia, and hyponatremia, and blood gas levels confirmed the presence of a metabolic alkalosis. These findings are classic for a high gastrointestinal obstruction and vomiting of acidic gastric contents.The radiograph shows a high duodenal obstruction.
Surgical removal of a “napkin ring” lesion, histologically proven to be an intestinal adenocarcinoma, resolved the problem. This cat remained free of disease 2 years after surgery. B, Intestinal adenocarcinoma of the cat noted in A. Note the proximal intestine was dilated due to the “napkin ring” obstructive lesion.thickness biopsy specimens may be necessary for a definitive diagnosis.
In one series 65% of cats with intestinal mast cell tumors had metastases to regional lymph nodes, spleen, liver, lung, or bone marrow.
Anemia in cats with lymphoma is common but is usually low grade and characterized as normocytic and normochromic, which is compatible with anemia of chronic disease. Occasionally a moderate to severe anemia may be present due to GI blood loss secondary to lymphoma. Anemia is rarely a consequence of bone marrow involvement. Lymphocytosis requires evaluation of lymphocyte morphology and could indicate bone marrow involvement and a worse prognosis for remission.
Complete response rates to chemotherapy are as follows: stage I (93%), stage II (48%), stage III (52%), stage IV (42%), and stageV (58%). Cats with stage I and II disease have median survival times of 7.6 months compared with 3.2 months for cats with stage III and IV disease and 2.6 months for those in stage V.
Cats that are positive for the FeLV antigen have shorter survival times, but viral status does not influence response to therapy. In another study, response to therapy, FeLV status, and clinical substage were predictive of outcome. FeLV-negative cats that achieve a complete response following induction therapy are likely to have durable (greater than 6 months) responses, particularly when doxorubicin is included in the chemotherapy protocol.
Therapeutic Approach
Nutritional support is a crucial prerequisite for the successful management of intestinal tumors. Whenever chemotherapy or surgery is indicated, assisted tube feeding with esophageal, gastrostomy, or jejunostomy tubes is a must.
Resection of the intestinal mass is the only reported primary treatment for intestinal adenocarcinoma in cats, and there is only one report of a cat that was treated with adjuvant therapy.That cat received levamisole (2.3 mg/lb orally 3 days per week) for 2 months and lived 28 months before developing widespread metastases. The contribution of this treatment to survival is doubtful, because similar long survival times have been reported following surgery alone. Early studies that included some cats that died periopera- tively had median survival times of 5 weeks and 10 weeks, respectively; however, both studies included some cats that lived for 2 years. In more recent studies the average survival ranged from 6 to 15 months and some cats lived more than 4 years. These figures are significant because seven cats with confirmed lymph node metastasis at the time of surgery lived for an average of 12 months, and two cats with carcinomatosis lived 4.5 and 28 months. The finding of metastatic disease at surgery should not be a disincentive to treat cats surgically for intestinal adenocarcinoma.
Resection of duodenal adenomatous polyps is predictably associated with a good surgical outcome, although anorexia is a postoperative complication in more than half of feline patients.
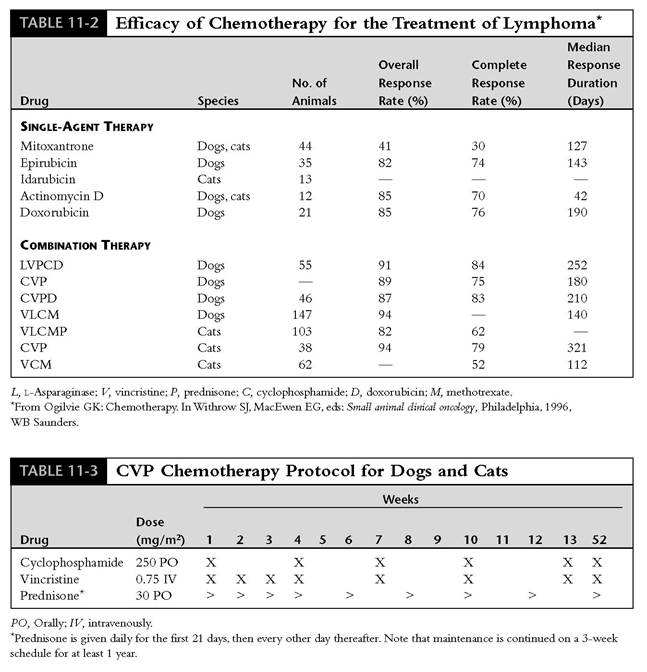
Chemotherapy is the mainstay of treatment for cats with alimentary lymphoma. Generally cats with lymphocytic lymphoma do substantially better than cats with large or intermediate lymphoblastic lymphoma. Single agents that have been used include prednisolone, cyclophosphamide, and chlorambu- cil.Varying responses have been seen with the use of each of these drugs, and in one report a cat had a complete response to cyclophosphamide for 14 months. The use of vincristine alone has produced long-term responses. L-Asparaginase, idaru- bicin, and mitoxantrone have been used with varying responses.
Combination chemotherapy, for example, the cyclophosphamide, vincristine, prednisone (CVP) protocol (see Table 11-3), still provides the basis for most chemotherapy protocols for feline lymphoma. In one study, median survival of 27 cats with alimentary lymphoma treated with vincristine (0.75 mg/m2 intravenously weekly for 4 weeks, then every 3 weeks thereafter), cyclophosphamide (300 mg/m2 orally every 3 weeks), and prednisolone (0.9 mg/lb/day) was 50 days. Although most cats responded poorly to chemotherapy, 9 cats achieved a complete remission. Survival times were not influenced by extent of GI involvement, sex, FeLV status, hematocrit, serum total protein concentration, and clinical stage. Response to therapy is probably the single most important prognostic factor for cats with GI lymphoma.
In another study 14 cats with alimentary lymphoma were treated with vincristine, cyclophosphamide, and methotrexate. The protocol was as follows: week 1, vincristine (0.01 mg/lb) administered intravenously; week 2, cyclophosphamide (4.5 mg/lb) administered intravenously; week 3, vincristine, same as week 1; week 4, methotrexate (0.36 mg/lb) administered intravenously. The median survival of these cats was 2.75 months.
In a different study 21 cats with alimentary lymphoma were treated with combination chemotherapy consisting of prednisolone, L-asparaginase, vincristine, cyclophosphamide, doxorubicin, and methotrexate (see protocol at end of this section). Median survival for these cats was 40 weeks, and overall median duration of first remission was 20 weeks. The only significant prognostic factor associated with duration of first remission was whether cats had a complete response following induction chemotherapy. Duration of first remission was significantly associated with survival time. Cats tolerated this protocol well.
In another study 38 cats with lymphoma were treated with induction COP chemotherapy. After induction, cats were randomized to receive either maintenance COP chemotherapy or single-agent doxorubicin. The median remission duration for the cats continuing on COP chemotherapy was 83 days, which was significantly shorter than the median remission for the cats that received doxorubicin as maintenance, which was 281 days. Therefore doxorubicin should be considered an efficacious agent for the maintenance treatment of cats with lymphoma. It is, however, a drug that is poor at inducing a complete remission. There was minimal toxicity noted in the cats in this report. It should be noted that the dose of prednisolone used in this study was 40 mg/m2 daily and the doxorubicin dose used was 25 mg/m2 every 3 weeks. The other drug dosages used are as printed above.
Finally, another study involved 67 cats with GI lymphoma that were treated with chemotherapy. Twenty-nine cats with lymphocytic lymphoma were treated with chlorambucil and prednisolone. The chlorambucil dosage we use is the total cumulative dosage of 6 mg/m2 body surface area (BSA). This works out to 2 mg every other day or on a Monday-Wednesday-Friday every week basis, depending on how small the cat is. The rule is to never break a tablet.The prednisolone dose is 0.5 to 1 mg/lb/day. Complete remission was obtained in 69% of these cats,with a median disease-free interval of 16 months. The cats with lymphoblastic lymphoma of the GI tract treated with the same chemotherapy did not do nearly as well, with a survival time of only 2.7 months and a complete remission rate of 18%.
Obtaining clean margins at surgery seems to increase survival time in cats with malignant colonic neoplasia. Data from this particular study indicate that survival time of cats with colonic lymphoma may not be affected by chemotherapy. Cats with an unidentified colonic mass should have a subtotal colectomy to increase survival time. Cats with colonic adenocarcinoma should have surgery, and adjunctive chemotherapy, using doxorubicin, should be considered as well.
Intestinal mast cell disease is best treated with large surgical resection.Prednisolone may have some efficacy. The following combination chemotherapy has demonstrated some success: week 1, vinblastine (2 mg/m2) administered intravenously every 3 weeks; week 2, cyclophosphamide (300 mg/m2) administered orally over 3 to 5 days every 3 weeks; and oral prednisolone (0.54 mg/lb) administered daily.
Supportive therapy is very important for cats with GI neoplasia. Often these cats will require feeding tubes. For patients with frequent vomiting a jejunostomy tube may be necessary; otherwise an esophagostomy or gastrostomy tube may be appropriate. Subcutaneous fluid administration, antiemetics (metoclopramide at 0.09 to 0.18 mg/lb orally three times a day and ondansetron at 0.23 to 0.45 mg/lb orally one to two times a day), and appetite stimulants (cyproheptadine at 0.9 to 1.8 mg/lb orally two to three times a day) may be necessary for use in conjunction with chemotherapy. A complete blood count should always be performed 1 week after cyclophosphamide and doxorubicin administration, because both of these agents can be myelosuppressive. If the segmented neutrophil count is less than 1000 cells/pl, the next dose should be decreased by 10% to 25%. Doxorubicin-induced cardiotoxicity and cyclophosphamide-induced hemorrhagic cystitis are rare in the cat.