intestinal tumors in dogs
Background
In dogs, adenocarcinomas are the most common tumor in the intestine and the stomach. Leiomyosarcomas are less common than adenocarcinoma and occur more frequently in the intestine than in the stomach (Figure 11-9).
Intestinal leiomyomas are uncommon. All reported cecal tumors have been of smooth muscle origin (i.e., leiomyosarcoma or leiomyoma). Epithelial and smooth muscle tumors both occur in other areas of the intestinal tract. Lymphoma may be found anywhere within the GI tract but is usually associated with systemic disease. In one study of 144 dogs with lymphoma, 6.9% had GI involvement.Intestinal tumors generally occur in older dogs. The median age is 11 to 12 years, although the average age of dogs with lymphoma is younger. There are no obvious breed predilections. Males are more frequently affected by intestinal tumors than females, although this trend is most marked for adenocarcinoma and is less obvious for smooth muscle tumors.
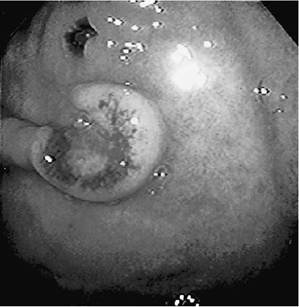
Figure 11-8 Ulcer and thickening of the pylorus of a 4-year-old, FeLV-negative cat with a history of intermittent vomiting, diarrhea, and weight loss. Endoscopic biopsy specimens were used to confirm the presence of small cell lymphoma.Vincristine, chlorambucil, and prednisone therapy was used to resolve all endoscopic abnormalities and clinical signs for a 2-year period. (Courtesy Dr. David Twedt.)

Figure 11-9 Small intestinal duodenal tumor causing partial obstruction of the bowel, vomiting, and diarrhea in a 10-year-old poodle. Resection of this leiomyosarcoma resulted in immediate resolution of clinical signs. Doxorubicin chemotherapy was initiated to treat any microscopic metastatic disease.The dog did extraordinarily well, and the owners were very happy with the patient’s 2-year, disease-free interval.
(Courtesy Dr. David Twedt.)Clinical Parameters
Clinical signs give very little indication as to the type of neoplasm in a dog with an intestinal tumor. Symptoms may, however, direct the clinician to a particular area of the intestinal tract. For example, vomiting is most often associated with tumors of the duodenum or jejunum, whereas weight loss and diarrhea are usually seen in dogs with jejunal or ileal tumors. Tenesmus or hematochezia most often occurs with colonic or rectal tumors. Distal rectal tumors are mostly palpable as a single pedunculated mass; tumors located rostrally are more likely to be multiple (“cobblestone appearance”) or appear as an annular constriction. Dogs with rectal leiomyomas may be asymptomatic, presumably owing to slow growth of these tumors; however, these tumors may become very large (up to 12 cm in one study). Anorexia, depression, and lethargy may accompany tumors in any location. Hypochromic anemia is a less common sign; it may be due to melena and iron deficiency. Ascites, abdominal pain, and peritonitis from intestinal rupture may occur; the last condition is mainly seen with cecal leiomyosarcomas. Clinical signs have often been present for weeks to months, although dogs that are vomiting are usually presented by their owners more rapidly.
On physical examination an abdominal mass may be palpated, particularly if the tumor is in the upper small intestine. Rectal examination may reveal a stricture, mass, or irregular rectal wall in more than 60% of affected dogs.
Clinical Work-up
In addition to routine blood work and urinalysis, thoracic and abdominal radiographs, endoscopy, and ultrasonography should be used to image the tumor and to identify metastasis. Plain radiographs may help delineate an abdominal mass and may also reveal other abnormalities, such as gas-filled and fluid-filled dilated loops of bowel, which are suggestive of obstruction. Pneumoperitoneum may indicate tumor rupture or a septic peritonitis.
Contrast radiography most often shows an “apple-core” lesion for tumors of the small intestine but also may show irregular filling defects or leakage caused by perforation. Ultrasonography is a noninvasive and rapid means of identifying intestinal tumors and provides a guide for obtaining biopsy specimens, as well as a method of staging for abdominal metastases. Ultrasonography is the staging method of choice for dogs with intestinal tumors.Endoscopy can be used to obtain biopsy specimens, which may provide a definitive diagnosis for duodenal or colonic and rectal tumors; however, multiple biopsy specimens should be taken, because lesions deep to the mucosa may escape detection, and tumors that create ulcerated lesions may be obscured by inflammatory changes (Figure 11-10). In one study, endoscopic biopsy of intestinal lymphoma was confounded by the presence of inflammatory infiltrates in nearly 50% of the dogs. Endoscopy of the entire large bowel is particularly important when a distal rectal tumor is palpated, because dogs may have additional proximal lesions that could otherwise remain undetected and continue to cause clinical signs after surgery. Biopsy of small intestinal tumors often requires exploratory laparotomy, but biopsy of rectal tumors may be performed via proctoscopy or by prolapsing the rectum manually or with stay sutures.
Metastasis is more commonly described for intestinal adenocarcinoma than for leiomyosarcoma, and the most common sites of metastasis are the regional lymph nodes. In 22 (71%) of 31 dogs with small intestine adenocarcinoma, there was evidence of metastases to regional lymph nodes. In contrast, metastasis occurred to liver and lung in only four (13%) of these 31 dogs. Leiomyosarcoma
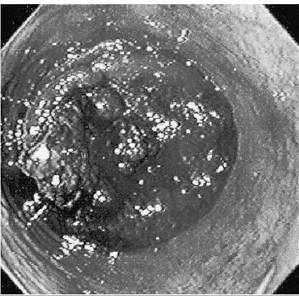
Figure 11-10 Colonic carcinoma of a 7-year-old castrated male dog with a 5-week history of straining to defecate. Results of blood work, abdominal and chest radiographs, and abdominal ultrasound were normal.
Colonoscopy was used to obtain a diagnosis of colonic carcinoma. Resection of the colon resulted in control of this tumor for 24 months. (Courtesy Dr. David Twedt.)does not usually metastasize; metastases occur in less than 30% of affected dogs, often long after definitive surgery. Metastasis of colorectal adenocarcinoma is considerably less common.There was no evidence of metastasis in 78 dogs with this disease even after long survival times following surgery.
Carcinoid is a term used to describe intestinal tumors of neuroendocrine derivation that may be hormonally active. Of five reported intestinal carcinoids, all had metastases to regional lymph nodes and liver at the time of diagnosis and there were additional sites of metastasis in two dogs.
Prognostic Factors
In one study of colorectal adenocarcinomas, dogs with annular tumors had the shortest average survival (1.6 months). Dogs with tumors that comprised multiple “cobblestone” nodules had an average survival of 12 months. Dogs with a single pedunculated polyp had the longest survival (32 months) after surgery. These prognostic factors are probably related to the ease with which complete surgical excision may be performed.
In one group of dogs with adenomatous polyps or carcinoma in situ of the colon and rectum, malignant transformation was documented in 18% of the cases. Higher rates of recurrence and malignant transformation occurred in dogs with multiple masses or diffuse disease and in dogs initially diagnosed with carcinoma in situ.
Diffuse intestinal lymphoma carries a poor prognosis in dogs. Prognostic factors for GI lymphoma are those that have been previously described for multicentric lymphoma.
Therapeutic Approach
There is little information regarding survival after surgical resection of small intestinal adenocarcinomas. Four dogs with small intestinal tumors that had not metastasized at the time of surgery had survival times of 3 days, 6 months (two dogs), and 2 years.
In another study five dogs with surgically treated cancer of the small intestine had an average survival of 55 days. In another study, dogs with surgically treated epithelial tumors had a mean survival of 6.9 months and local recurrence was the cause of death in all dogs. In one study, dogs with large intestinal adenocarcinoma treated only with fecal softeners had a mean survival of 15 months.Surgical excision of intestinal or cecal leiomyosarcoma carries a better prognosis. Thirteen (57%) of 23 dogs with leiomyosarcoma survived the perioperative period and had median survivals of 8 to 13 months (ranging from 2 months to 7 years). Only 3 of these 13 dogs developed metastases. One dog had evidence of metastasis at the time of surgery and without explanation survived 3 years without adjuvant therapy. Cecal rupture may occur and lead to death in some dogs as a result of peritonitis. Perioperative mortality was 60% in 10 dogs in one study. Four dogs survived for 19 months, 28 months, 36 months, and 48 months. Two of these dogs died due to recurrence (28 months) or metastases (36 months).
The median survival after surgical resection of colorectal leiomyoma was 26 months. Only one of five affected dogs died from tumor-related causes. Colorectal adenocarcinomas have a low rate of metastasis, and treated dogs may have long survival times following diagnosis. Of multiple treatment modalities, local excision gave the longest average survival (22 months) with the lowest complication rate. Recurrence after local excision of a solitary mass occurred in 11 (52%) of 21 dogs. In contrast, radical surgical excision of annular colorectal adenocarcinoma resulted in wound dehiscence and septic peritonitis in all four dogs treated.
Cryosurgery prolonged survival in 11 dogs with colorectal adenocarcinoma (average survival of24 months). Recurrence was similar to that after local excision; however, additional complications, including stricture (5 of 11 dogs), rectal prolapse, and perineal hernia followed treatment.
Other techniques, such as electrocoagulation and neodymium: yttrium-aluminum-garnet (Nd:YAG) laser-assisted surgery, provide control similar to that of local excision.Radiation therapy using a single high dose (15 Gy to 25 Gy) of orthovoltage teletherapy may provide reasonable control for recurrent distal rectal adenocarcinomas. In six dogs, median tumor control duration was 6 months and no complications were reported. One dog treated with radiation therapy suffered a rectal perforation and died from peritonitis 2 months after treatment.
Results of chemotherapy have not been reported for intestinal tumors in dogs. Doxorubicin has been suggested by some as a good adjunctive therapy. Few data exist quantitating its efficacy.
Surgery is indicated in obstructive intestinal lymphoma or when bowel perforation has occurred. Chemotherapy protocols for lymphoma can be employed as adjuvant therapy or as the major form of therapy in diffuse disease (Tables 11-2 to 11-5). For the dog the longest remission and survival times have been reported with the University of Wisconsin-Madison protocol noted in Table 11-5. This protocol is complex but gratifying because of consistently improved responses.The University of Wisconsin-Madison short canine lymphoma protocol appears in Table 11-4. Diffuse GI canine lymphoma is associated with a variable response to chemotherapy, although solitary or nodular lymphoma does respond better.