Laminitis
MicheUe C. Coleman
■ Definition Laminitis, defined as inflammation of the laminae of the hoof wall, results in degeneration, necrosis, and inflammation of the dermal and epidermal laminae in the hoof wall of equids and ruminants.
The economic and welfare impacts of laminitis are high because of the associated poor prognosis, severe pain, and frequency of recurrence. Recognizing the impact of laminitis on horses and horse owners, veterinarians desire an improved understanding of laminitis, as evidenced by a 2009 survey (personal communication, Keith Kleine, AAEP Foundation) by the American Association of Equine Practitioners in which members identified laminitis as the highest priority for research funding and investigation.■ Etiology and Pathogenesis Laminitis has a complex and multifactorial etiology, ultimately resulting in lamellar degradation of the suspensory apparatus of the distal phalanx.
Disease states thought to be associated with laminitis include sepsis and systemic inflammation, equine metabolic syndrome (EMS), pituitary pars intermedia dysfunction (PPID), and mechanical or traumatic overload. Septic processes including endotoxemia, gastrointestinal disease, pneumonia, and septic metritis are frequently associated with the development of laminitis. Laminitis has also been noted secondary to systemic inflammation resulting from an overload of carbohydrates, such as from overgrazing lush pastures or unrestricted access to concentrates. Excess weight bearing as a result of a contralateral limb lameness and trauma to the distal phalanx following exercise on hard ground can also result in laminitis. Exposure to a water-soluble toxin in black walnut shavings1 and administration of corticosteroids have also been associated with the development of laminitis.2
In cattle, overweight heifers fed excess concentrates and housed on concrete surfaces appear to be at increased risk.
■ Pathophysiology The pathophysiology of laminitis has not been fully elucidated; however, it appears to involve a combination of events that lead to lamellar degeneration, impaired biomechanical function, and debilitating pain. Several experimental models for induction of laminitis have been developed, including carbohydrate overload,3 fructan overload,4 black walnut extract administration,1,5 and hyperinsulinemic models.6,7 Distinct pathophysiologic differences between these models exist, emphasizing the complexity of the pathophysiology of disease. Together, these models support several similar and interconnected theories on the pathophysiology of laminitis, including digital hemodynamic, enzymatic, inflammatory, endocrinopathic, and mechanical or traumatic events.
The bounding digital pulses and increased hoof wall temperature in acute laminitis gave rise to one of the earliest mechanisms to receive research support, which suggests a vascular component of the disease. Early research evaluated the role of hypertension8 and the angiographic appearance of the laminitic equine digit,9 with the thought that increased capillary pressures secondary to venoconstriction of the digital microvasculature resulted in laminar edema, increased arteriovenous shunting, and capillary collapse.10 Further research has implicated the role of thrombosis,11 vascular supply,12-15 and insulin16 on vascular dysfunction and lamellar ischemia, with increasing interest in endothelial dysfunction.17
Alteration of enzymatic activity within the lamella has been proposed as another potential mechanism of laminitis. Matrix metalloproteinase enzymes (MMP-2 and MMP-9) have been isolated in increased quantities from lamellar tissue affected by laminitis,18 affected lamellar tissue has been shown to increase transcription of MMP,19 and MMPs have been associated with neutrophil migration into the lamellae.20 The activation of MMPs is thought to result in separation of lamellar cells from their basement membranes; however, the mechanism by which activation occurs has yet to be elucidated.
Importantly, differences in MMP 2122 activity in the various models of laminitis have been noted.21,22Experimental models of equine laminitis have displayed a number of inflammatory events. The presence of endothelial activation, leukocyte infiltration, proinflammatory cytokines, leukocyte activation and chemotaxis, and activation of degrada- tive enzymes such as MMPs have been reported in the digital lamellae in different models of laminitis. Increased expression of inducible cyclooxygenase, COX-2, suggest that prostaglandins may play a role in laminar dysfunction.23-25
The role of endotoxemia in the development of laminitis remains unclear. Although systemic inflammation is a risk factor for development of laminitis, experimental endotoxin administration fails to induce the disease.26 This could be explained by the fact that endotoxin does not act alone but rather in combination with several factors, including bacterial toxins, necrotic cell products, and proinflammatory cytokines. Endotoxin has been detected in the blood of horses following experimental carbohydrate overload27 and is known to affect digital vascular function and platelet activation. Recent studies have hypothesized that the proinflammatory state of carbohydrate overload models is driven by an immune response to the rapid overgrowth of gram-positive and gram-negative cecal bacteria.28
Experimental models resulting in hyperinsulinemia reliably induce laminitis in ponies and horses.6,7 Many theories on the pathogenesis of hyperinsulinemic laminitis exist, and it is probable that these theories are interconnected. Plasma or serum insulin concentrations can be used as predicitive29 and prognostic30 indicators for ponies at risk of developing laminitis. The role of insulin in glucose deprivation,31,32 glucose excess,33 upregulation of MMPs,21 vascular effects,34 and proinflammatory effects has been considered.
Laminitis has long been associated with mechanical overload on the distal phalanx, such as excessive concussion (road founder) and supporting limb laminitis. The mechanism of insult to the laminae is unknown, and currently models for studying this form of laminitis are poorly developed.
These theories of the pathogenesis of laminitis are complex and likely interconnected. The development of experimental models has accelerated our knowledge and understanding of the complex pathophysiology; however, the relationship of these models to the naturally occurring condition is unknown.
■ Clinical Signs Laminitis can affect a single foot or all four feet but is most commonly noted in the front feet of horses (likely due to an increased load on the forelimbs) and the hind feet of ruminants. Supporting limb laminitis occurs on the supporting forelimb or hindlimb opposite the non-weightbearing limb. The lameness may vary in severity from subtle to prolonged recumbency due to digital pain. Because of this variability, the Obel grading system was developed to better describe severity.35,36 Grade 1, the least severe classification, is characterized by shifting weight with no apparent lameness at the walk but a short-stilted trot. Horses with grade 2 lameness are willing to walk but have a stilted gait and are willing to lift a foot off the ground. Grade 3 is characterized by reluctance to ambulate and resistance to having a foot lifted off the ground. The most severe classification is grade 4, in which the horse refuses to move.35 Shifting of weight to the hindlimbs if laminitis affects the forelimbs results in a characteristic “saw horse” stance and may be accompanied by anxiety, muscle fasiculations, anorexia, or reluctance to move in severe cases. Other clinical signs consistent with laminitis include bounding digital pulses, sensitivity to hoof testers over the sole at the toe, sensitivity to tapping of the hoof wall at the toe, heat over the dorsal surface of the hoof wall, and swelling of the coronary band.
Rotation or distal displacement of the third phalanx within the hoof capsule may occur. With displacement, significant lameness often persists. A dropped sole or depression over the coronary band suggests that displacement has occurred.Chronic laminitis results in lameness and deformation of the hoof capsule, which vary with duration of disease and type of displacement. In these cases, the sole is flat or dropped, the white line is widened, and the hoof wall shows signs of uneven growth. Irregular rings of growth may be noted around the hoof wall, more widely spaced at the heels. The abaxial white line develops apparent hemorrhages, and fissures of the hoof wall may be noted parallel to the coronary band. In ruminants, the sole softens and assumes a light-yellow discoloration.
■ Clinical Pathology and Radiology There are no clinicopathologic findings specific to acute or chronic laminitis, but changes may reflect an underlying disease process such as endotoxemia, enteritis, colitis, pleuropneumonia, or metritis. Changes may also be seen as a result of glucocorticoid and catecholamine release in response to pain and stress. One study showed that horses euthanized for chronic laminitis had higher white blood cell counts when compared to control horses and horses with less severe disease.37 Baseline values for creatinine and total protein should be obtained, as these are important parameters to monitor for NSAID enteropathy.
Radiographic examination is an essential component in evaluating horses with suspected laminitis, for monitoring progress, and for providing therapeutic recommendations and prognostic information. Standard radiographic views, including lateromedial and 65-degree dorsoproximal-palmarodistal views, should be taken of all suspected digits in acute disease to serve as a baseline for subsequent radiographic studies and to determine if prior radiographic changes are present. Using a consistent technique is important to achieve a true lateral image and to allow accurate evaluation of radiographic parameters for comparison of serial studies.
For both views, the foot should be thoroughly cleaned and placed on a wooden block such that the x-ray beam can be centered on the solar margin of the distal phalanx. A radiopaque marker placed on the middorsal hoof wall starting at the coronary band and extending distally can be useful in determining the position of the distal phalanx in relation to the surface marker.Primary radiographic changes in acute laminitis include thickening of the dorsal hoof wall as a result of inflammation, separation of the laminae, and separation of the distal phalanx from the hoof wall. When the suspensory apparatus of the distal phalanx fails, the distal phalanx rotates away from the hoof wall or displaces distally, increasing the distance between structures. This distance can be measured as a line vertical to
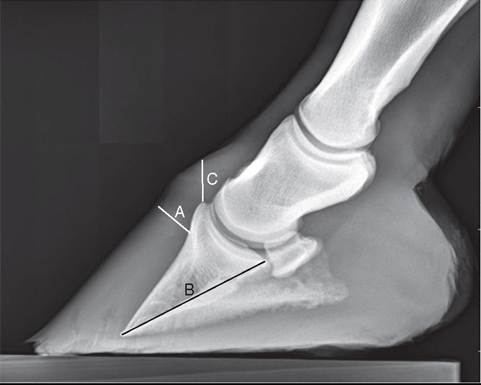
FIG. 38.29 Lateromedial radiograph of a horse with acute Iaminitis. A, Distance from the dorsoparietal surface of the distal phalanx to the dorsal surface of the hoof capsule. B, Length of the palmar cortex of the distal phalanx. C, Distance from the extensor process to the proximal aspect of the hoof wall distal to the coronary band.
the parietal surface of the distal phalanx and distal to the extensor process. In normal horses, this distance should be less than 18 to 20 mm (Fig. 38.29, A). A ratio between this dorsal measurement and the palmar cortical length of the distal phalanx measured from the dorsodistal tip of the bone to its articulation with the navicular bone (Fig. 38.29, B) can be used to account for changes in magnification and size of the foot. This ratio should be less than 28% in normal horses and more than 32% in horses with displacement of the distal phalanx. Sinking of the entire distal phalanx within the horny capsule can be assessed by measuring the vertical distance between the coronary band and the extensor process of the distal phalanx (Fig. 38.29, C). Soft tissue swelling of the coronary band may be apparent. Palmar or plantar rotation of the distal phalanx away from the hoof wall greater than 5 degrees is indicative of capsular rotation (Fig. 38.30, A).
In chronic cases, a radiolucent line may appear between the distal phalanx and the sole or hoof wall due to accumulation of serum between the dermal and epidermal laminae. The angle of the solar margin of the distal phalanx to the ground surface may be a more accurate assessment of rotation in chronic cases (Fig. 38.30, B). Radiographic evidence of a previous episode of laminitis may be evident in clinically normal horses. Changes may include increased thickness of the dorsal hoof wall, a radiolucent line in the dorsal hoof wall, modeling of the toe of the distal phalanx, and/or uncorrected rotation of the distal phalanx.
Positive contrast venography is useful in identifying filling defects in the digital vasculature, including the lamellar vessels, the circumflex area, and the terminal arch. Venographic studies are most valuable in early disease and may reveal damage in the hoof before radiographic changes are evident.38
The availability of MRI in equine medicine is increasing. High-field-strength MRI can provide detailed visualization of the laminae in the equine digit. Studies comparing digital radiography and MRI of horses with initial active laminitis suggest that measurements obtained with MRI were more sensitive and specific predictors of laminitis.39
■ Epidemiology The estimated incidence of laminitis ranges from 1.5% to 34%,40 with an estimated lifetime risk of 15%.41 The term endocrinopathic laminitis has been used to describe
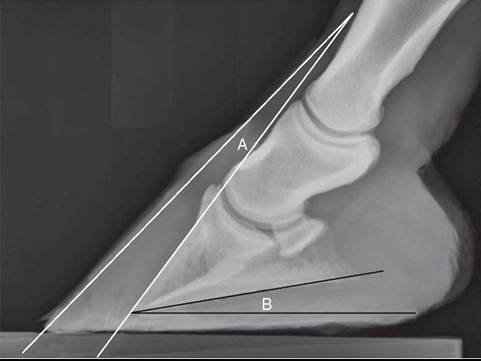
FIG. 38.30 Lateromedial radiograph of a horse with acute laminitis. A, Measurement of the degree of capsular rotation. B, Measurement of the angle of the solar margin of the distal phalanx to the ground surface of the foot.
laminitis in horses with hyperinsulinemia, PPID, or obesity or that have been administered glucocorticoids42 and has been recognized as the most common cause of laminitis in private equine practice.43,44 Further, in the National Animal Health Monitoring System equine study45 performed in 2000, horse owners in the United States reported that pasture-associated laminitis and laminitis of unknown etiology were the most common forms of laminitis.
Epidemiologic studies on the risk factors for naturally occurring laminitis in horses are limited, with inconsistent results. A recent systematic review of publications assessing the risk factors for naturally occurring laminitis revealed only an association between chronic laminitis and increasing age. Results for other horse-level factors, including gender, breed, and body weight, were inconsistent. No consistent associations have been identified with other factors, including exercise and seasonality.46 Associations between health conditions and laminitis in hospitalized horses has been investigated, with endotoxemia the only variable for which an association was noted.47 Several cohort studies48,49 have identified risk factors (e.g., hyperinsulinemia) for endocrinopathic laminitis in ponies, and a recent case control study in North America identified that generalized and/or regional adiposity, corticosteroid administration, and endocri- nopathic disease were risk factors for development of pasture and endocrinopathic laminitis.50 Duration of lameness was a risk factor for development of laminitis in the contralateral limb of horses with unilateral laminitis, and horses that developed this complication were more likely to be euthanized than horses that did not develop laminitis.51 It is apparent that inconsistent and conflicting results regarding horses' risks of developing laminitis exist, supporting the need for well-designed observational studies to improve the strength of evidence.
■ Necropsy Necropsy findings depend on the duration and severity of the disease. Separation of the primary epidermal laminae of the hoof wall and the collagen fibers of the corium occurs as a result of complete degeneration of the secondary epidermal laminae. The distal phalanx may sink, rotate ventrally, or penetrate the sole. Necrotic laminae are prone to abscessation. Severe changes include fractures of the solar margin, osteomyelitis, or resorption of the distal phalanx.
■ Treatment An incomplete understanding of the pathophysiology and progression of laminitis limits our ability to prevent and treat the disease successfully and results in
considerable controversy regarding appropriate treatment regimens. Therapy is often empiric and based on the experience of the clinician. Advancement in our knowledge of the complex pathophysiology of laminitis may result in more effective preventative and therapeutic approaches. Acute laminitis should be considered an emergency, and therapy should be initiated before or immediately following the onset of clinical signs. General principles of therapy include minimizing or eliminating predisposing factors, decreasing pain and inflammation, promoting digital circulation, reducing tension on the laminae, and reducing platelet activation and coagulation.
ELIMINATING CAUSES. Predisposing factors to the development of laminitis should be minimized or eliminated. Following ingestion of large amounts of grain, laxatives or purgatives including mineral oil or activated charcoal may be administered via nasogastric tube. Exhaustion, dehydration, and hypovolemia may be treated with appropriate intravenous fluid therapy. Appropriate therapy for combating the effects of endotoxemia and septic processes, including colitis, enteritis, pleuropneumonia, metritis, and retained placenta, should be initiated and may include intravenous fluids, parental antibiotics, NSAID therapy, polymyxin B, and hyperimmune serum or plasma. Treatment and management of other conditions associated with laminitis such as PPID and EMS are discussed elsewhere in this text.
Preventative measures in suspect cases include placing the horse in a deeply bedded stall, frog support, and corrective shoeing or trimming.
DECREASING PAIN AND INFLAMMATION. Antiinflammatory therapy is recommended to decrease lamellar inflammation, edema, and pain associated with laminitis. The most common NSAID used in horses is phenylbutazone at a dose of 2.2 to 4.4 mg/kg intravenously or orally every 12 hours. Flunixin meglumine can be administered at a dose of 0.5 to 1.1 mg/ kg orally or intravenously every 8 to 12 hours for its antiinflammatory effects, or at a dose of 0.25 mg/kg intravenously every 8 hours to interrupt eicosanoid production associated with endotoxemia. Ketoprofen and firocoxib are also labeled for use in horses. Dimethyl sulfoxide (DMSO) is a free radical scavenger that aids in reduction of edema and may reduce ischemia-reperfusion injury. DMSO is typically administered at 0.1 to 1.0 g/kg intravenously diluted in a polyionic fluid to a concentration of 10% to avoid hemolysis. Pentoxifylline is a phosphodiesterase inhibitor with antiinflammatory and immune regulatory properties. It has been shown to have antiinflammatory effects52 both in vivo and in vitro in horses and has recently been shown to effectively inhibit MMP in horses.53 Further, evidence suggests that pentoxifylline reduces inflammation and blood glucose concentration after diabetes induction in rats by improving insulin sensitivity, making it a potential therapy for laminitis associated with metabolic disease.54,55 In a recent study, the analgesic effects of tramadol hydrochloride administered in combination with ketamine hydrochloride were evaluated in horses with naturally occurring chronic laminitis. Tramadol provided little analgesic effect, but analgesia was enhanced by administration of subanesthetic doses of ketamine.56
PROMOTING DIGITAL BLOOD FLOW. Venous vasoconstriction may be involved in the pathogenesis of laminitis, but several therapeutic agents that have been suggested for increasing blood flow to the digit, including isoxsuprine and nitroglycerine paste, have not proven effective. Acepromazine, a phenothiazine tranquilizer, has been shown to increase digital blood flow in clinically normal horses with a short duration of efficacy of about 30 minutes.57 Acepromazine has been recommended at a dose of 0.03 to 0.06 mg/kg intramuscularly or intravenously every 6 to 8 hours; however, at this dosage interval, the patient should be monitored for hypotension. If this complication is documented or suspected, the dosage interval should be extended or therapy with acepromazine should be discontinued. Caution should be taken in stallions due to the risk of paraphimosis.57
Continuous application of cryotherapy of the distal limb, in which hoof wall surface temperatures are maintained at 5° to 10° C for 48 to 72 hours, has been shown to limit the clinical, histologic, and biochemical abnormalities associated with experimentally induced acute laminitis in the oligofructose model.58-62 The mechanistic effect is unclear, but involvement of the inflammatory61,63 and vascular64 pathways is suspected. Several methods of cooling the digit have been used, including ice water immersion bath, wader boots, ice packs, and 5-L fluid bags, with variation in the hoof wall surface temperature between methods.65
REDUCING TENSION ON THE LAMINAE. Because laminar deformity is likely due to tension placed on the suspensory apparatus of the distal phalanx, reduction of mechanical force and stabilization of the distal phalanx are essential in the treatment of acute laminitis. Horses should be confined to strict stall rest and not be exercised in the acute stages of the disease. The horse should be encouraged to lie down, and bedding in the stall, ideally sand, should be deep. Redistributing weight from the hoof wall to the bars, sole, and frog may decrease laminar tension. Various methods have been suggested, including silicone impression material (EquiFlex-Pak [Sound Horse Technologies, Unionville, Pa.]), styrofoam insulation board, Lily Pads (Nanric Inc., Lawrenceburg, Ky.), the Steward Clog (Equine Digit Support System Inc., Penrose, Colo.), and Soft-Ride boots (Soft-Ride Inc., Vermillion, Ohio). Regardless of the method of weight redistribution, it is important to remember that once the distal phalanx displaces, increased pressure over the sole where the distal phalanx displaces may cause severely increased discomfort. Various methods of distal limb casts have also been used to improve stability to the distal phalanx.
Decreasing tension on the deep digital flexor tendon will also help decrease tension on the laminae. This can be accomplished by elevating the heels with a wedge (i.e., the Redden Modified Ultimate Wedge [Nanric Inc., Lawrenceburg, Ky.]) or transecting the deep digital flexor tendon to reduce caudal pull on the coffin bone.
Depending on the degree of rotation and/or distal displacement in chronic laminitis, various methods of hoof care and shoeing have been used. More radical approaches, including hoof wall resection and coronary band grooving, have been historically used with varying efficacy.
ANTICOAGULANT THERAPY. Heparin has been recommended in the treatment of laminitis to reduce microthrombi and platelet-platelet or platelet-neutrophil aggregates that are thought to form during laminitis. Heparin was recently reported to have potential antiinflammatory effects on equine endothelium exposed to neutrophil-derived myeloperoxidase.66 Unfractionated heparin was shown to reduce the proportion of horses with proximal enteritis that develop laminitis when administered prophylactically,67 and low-molecular-weight heparin reportedly reduced the incidence and severity of laminitis in postoperative colics.68
■ Prognosis There is little evidence-based research on prognosticating laminitic horses; however, it is likely that the prognosis of laminitis depends largely on the severity of the pathology, type of displacement, clinical signs, and underlying diseases or conditions. Prognosis may also be influenced by financial constraints, owner expectations, and owner compliance. In general, rotation is considered to have a more favorable prognosis than distal displacement, which is considered to have a more favorable prognosis than unilateral displacement. The degree of rotation and distance from the proximal margin of the extensor process of the distal phalanx to the proximal margin of the hoof were reported to be important factors in return to soundness and prognosis for survival.69 General guidelines based on degree of lameness and rotation and progression of clinical findings proposed by Redden in 1988 can be found in the previous edition of this text. In one study, 75% of horses referred to a university veterinary hospital with acute laminitis did not return to athletic function, and a majority were euthanized within 1 year due to poor response to therapy or development of complications.70
■ Prevention and Control Preventative measures are aimed at decreasing risk factors for development of the disease, but our poor understanding of the etiology and pathophysiology of the disease make prevention challenging. In general, suspected risk factors such as uncontrolled grazing on lush pastures, unrestricted access to grain or concentrates, factors contributing to gastrointestinal upset including rapid changes in diet, and retained placenta should be avoided when possible.
Despite continued limitations in our understanding of laminitis, it is likely that developments in biomedical research, industrial pressures, and extensive research collaboration will continue to advance our knowledge and understanding of the pathophysiology of laminitis and improve our ability to prevent, manage, and treat the condition.