MEGAESOPHAGUS
Megaesophagus is a syndrome characterized by generalized esophageal dilation and hypoperistalsis, which is often severe. It is differentiated from localized cases of esophageal dilation most of which are caused by mechanical problems with esophageal dilation occurring proximal to the site of obstruction (e.g., vascular ring anomalies, strictures, foreign bodies, neoplasia).
There may or may not be abnormal peristalsis associated with these disorders. Clinicians should be aware that not all patients with esophageal motility disorders have megaesophagus. Some patients have various degrees of esophageal hypomotility (e.g., slow stimulation of secondary waves of esophageal contraction, or “sluggish motility”) that may be segmental or diffuse. Survey thoracic radiographs are often normal in these patients. Mild to moderate esophageal hypomotility is best evaluated with fluoroscopic studies in which both liquid contrast alone and liquid with food are used to study the strength and coordination of esophageal peristalsis.Megaesophagus may be congenital or acquired (adult onset). In most clinical practices, adult-onset idiopathic megaesophagus is seen somewhat more commonly than congenital megaesophagus.A familial predisposition for congenital megaesophagus has been identified for many breeds of dogs (Great Dane, German shepherd, Irish setter, golden retriever, Labrador retriever, greyhound, Newfoundland,
| UABLEfiitf Profiles for Esophageal Disease Based on Signalment | |
| Parameter | Clinical Association |
| Age | |
| Young | Vascular ring anomaly; idiopathic megaesophagus; foreign body |
| Mature | Esophageal neoplasia |
| Breed | |
| Boston terrier | Vascular ring anomaly (PRAA) |
| Bouvier | Dysphagia caused by hereditary muscular dystrophy (oropharyngeal dysphagia and megaesophagus) |
| Cocker spaniel | Cricopharyngeal achalasia |
| Collie | Familial canine dermatomyositis (oropharyngeal dysphagia and megaesophagus) |
| English bulldog | Vascular ring anomaly (esophageal compression by left subclavian artery and brachiocephalic artery) Esophageal deviation cranial to the heart (normal variant) |
| German shepherd | Idiopathic megaesophagus Vascular ring anomaly (PRAA) Acquired myasthenia gravis Giant axonal neuropathy |
| Golden retriever | Idiopathic megaesophagus Acquired myasthenia gravis |
| Great Dane | Idiopathic megaesophagus Vascular ring anomaly (PRAA) |
| Greyhound | Idiopathic megaesophagus |
| Irish setter | Idiopathic megaesophagus Vascular ring anomaly (PRAA) |
| Jack Russell terrier | Congenital myasthenia gravis |
| Labrador retriever | Idiopathic megaesophagus Hereditary myopathy (megaesophagus) |
| Miniature schnauzer | Idiopathic megaesophagus |
| Newfoundland | Idiopathic megaesophagus |
| Rottweiler | Spinal muscular atrophy (megaesophagus) |
| Shar-pei | Idiopathic megaesophagus Hiatal hernia Esophageal deviation cranial to the heart (mild regurgitation) |
| Smooth fox terrier | Congenital myasthenia gravis |
| Springer spaniel | Cricopharyngeal achalasia Polymyopathy (megaesophagus) Congenital myasthenia gravis |
| Wirehaired fox terrier | Idiopathic megaesophagus |
| Siamese cat | Idiopathic megaesophagus |
PRAA, Persistent right aortic arch.
From Johnson SE, Sherding RGiDiseases of the esophagus and disorders of swallowing. In Birchard SJ, Sherding RG,eds: Manual of small animal practice, ed 2,Philadelphia, 2000,WB Saunders.
shar-pei), as well as for Siamese cats (although megaesophagus rarely occurs in cats). Congenital megaesophagus is known to be inherited in wirehaired fox terriers and miniature schnauzers. It is transmitted in wirehaired fox terriers as a simple autosomal-recessive trait, whereas in miniature schnauzers it is transmitted as a simple autosomal- dominant or a 60% penetrance autosomal-recessive trait. The acquired form has been reported in many pure-breed dogs. Breeding of affected animals is not recommended.
Etiology
The pathogenesis of megaesophagus is poorly understood. Physiologic studies in dogs with megaesophagus suggest that a defect exists in the afferent neural pathway. Efferent neuromuscular pathways appear to be intact. It has been shown that dogs with idiopathic megaesophagus do have cyclical migrating motor complex activity and that the upper and lower esophageal sphincter responses to swallowing are intact and normal. Mechanisms may be similar for both congenital and acquired idiopathic megaesophagus. Diminished motor responses of the upper and lower esophageal sphincters to intraluminal stimuli have been identified.
Megaesophagus in dogs was previously incorrectly compared with a human esophageal disorder called achalasia, which is characterized by failure of the lower esophageal sphincter to relax properly and ineffective peristalsis of the esophageal body. Treatment of this human disorder involves cardiomyotomy. Achalasia has never been proven to occur in animals. Esophageal sphincter tone is normal, not increased, in dogs with megaesophagus. Cardiomyotomy is therefore clearly not indicated in dogs with megaesophagus.
Acquired megaesophagus occasionally occurs secondary to other disorders, especially diseases that can cause diffuse neuromuscular dysfunction (e.g., focal or generalized myasthenia gravis, hypoadrenocorticism, and dysautonomia in cats).
Causes of megaesophagus are listed in Box 4-1. Because appropriate management of some of these disorders may lead to resolution of megaesophagus, it is rec-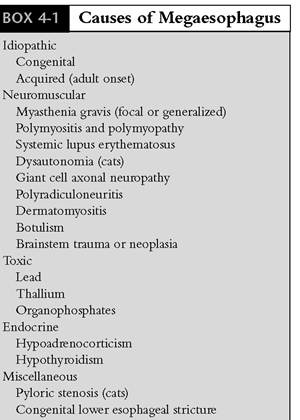
ommended that patients with acquired megaesophagus be evaluated for the presence of a primary disorder. It is emphasized, however, that the majority of patients with megaesophagus have idiopathic disease, and treatment centers on general management principles. Selected primary disorders are discussed in more detail later in this chapter.
Congenital Idiopathic Megaesophagus
Congenital idiopathic megaesophagus involves generalized esophageal dilation of unknown cause, with signs of regurgitation usually beginning at or shortly after weaning. Occasionally, regurgitation does not begin until 2 to 6 months after weaning. Congenital disease should be considered in any young patient with megaesophagus. The incidence is highest in Great Danes, German shepherds, golden retrievers, Shar-peis, Irish setters, wirehaired fox terriers, and miniature schnauzers, although many other breeds can be affected by the disease. A hereditary mechanism has also been suspected in young cats, especially Siamese cats. Multiple animals in a litter can be affected.
The most important differential diagnosis in young dogs and cats with regurgitation that occurs around the time of weaning is vascular ring anomaly. Vascular ring anomalies occur quite uncommonly. Differentiation can often be made on survey thoracic radiographs (generalized dilation of the entire esophageal body is usually readily identified with megaesophagus) (Figure 4-1). Contrast studies are done on patients with suspected vascular ring anomaly to highlight both the presence of an obstruction just cranial to the heart and the severity of dilation proximal to the obstruction. Other important differential diagnoses in young patients with regurgitation include esophageal stricture and foreign body.
Treatment for congenital megaesophagus primarily involves elevated feedings (45 to 90 degrees of upper body elevation). The consistency of the food that is fed depends entirely on what type is associated with the least postprandial regurgitation. Promotility therapy (cisapride) may also be attempted, although this drug is not expected to be useful in dogs because it is a smooth muscle prokinetic agent and the canine esophagus consists entirely of skeletal muscle. Treatment details for megaesophagus are discussed later in this chapter.
A
B
id="Picutre 148" class="lazyload" data-src="/files/uch_group31/uch_pgroup24/uch_uch7225/image/image148.jpg">
FIGURE 4-1 Congenital megaesophagus in a 3-month-old German shepherd. There had been a recent onset of regurgitation. A, Lateral radiograph shows dilated, air-filled esophagus. Note that the entire esophagus is dilated, ruling out vascular ring anomaly. B, The puppy responded very well on an elevated feeding program. (This puppy is also shown in Figure 4-10, at 9 months of age.)
The prognosis for congenital megaesophagus is guarded. Although some patients can be successfully managed for many months to years, others suffer persistent regurgitation with frequent bouts of aspiration pneumonia, as well as wasting disease that results from the inability of the esophagus to transfer adequate amounts of nutrients to the stomach. Factors involved in determining prognosis include degree of dilation of the esophagus, especially that of the proximal thoracic esophagus, and degree of early response to positional feeding and dietary manipulation. Rarely some dogs may show spontaneous improvement. This may in part be due to the fact that the esophagus does not functionally mature until around 6 months of age. Dogs with severe esophageal dilation with pronounced sacculation proximal to the heart (Figure 4-2) often do

Figure 4-2 Severe congenital megaesophagus in a 6-month-old German shepherd.
Note the marked ventral deviation of the esophagus cranial to the heart. There is an accumulation of foreign material in this large sacculated space. Esophagoscopy confirmed that the entire esophagus was dilated, with no evidence of a vascular ring anomaly. With diligent medical management, the dog lived an energetic life. However, because of increasingly frequent bouts of aspiration pneumonia, the dog was euthanized at 2 years of age.more poorly over a period of time and have a shorter life span. Since esophageal function in patients with congenital megaesophagus does not commonly improve over time, owners must be counseled that long-term elevated feeding will be required to help control regurgitation. Breeding of affected patients is not recommended.
Acquired (Adult-Onset) Idiopathic Megaesophagus
Although acquired megaesophagus may occur secondary to many disorders, especially diseases causing diffuse neuromuscular dysfunction, the majority of affected patients have idiopathic megaesophagus. Despite this fact, successful treatment of an underlying cause may lead to complete resolution of the esophageal motility disorder. Therefore diagnostic tests are done to look for a primary cause. The extent of the diagnostic workup that is done in a patient with megaesophagus depends primarily on the signalment, the clinical signs, and the environment (e.g., toxicities such as lead poisoning and thallium and organophosphate intoxication can cause megaesophagus).
Signalment
Acquired megaesophagus has been reported in many pure- and mixed-breed animals. Although the age of onset of adult idiopathic megaesophagus
is frequently 8 years or older, younger patients can be affected. There is no sex predilection.
Clinical Signs
The dominant clinical sign of megaesophagus is regurgitation. Regurgitation may occur minutes to hours after eating. Frequency varies from several episodes per week to many (10 to 20) episodes in a single day in some patients. Most affected dogs are initially presented with the chief complaint of what their owners describe as “vomiting” (which is actually regurgitation).
It is up to the clinician to differentiate vomiting from regurgitation at the outset (see Chapter 1 for differentiation criteria).It must be noted that the degree of esophageal dysfunction does not always correlate with the severity of clinical signs. Some dogs have megaesophagus for weeks to months before the onset of regurgitation episodes, or they regurgitate only infrequently despite the appearance of marked esophageal dilation on radiographs. Conversely, some dogs regurgitate frequently despite radiographic evidence of mild to moderate dilation.
Other clinical signs may include acute or chronic cough that may or may not be associated with dyspnea and fever. These signs are most consistent with aspiration pneumonia, which is the most common complication of megaesophagus. All patients with esophageal dysfunction are at risk for sudden death related to aspiration and subsequent upper airway obstruction. Coughing may also be related to compression of lung tissue and airways by the enlarged esophagus and its contents. Occasionally coughing is the only clinical sign demonstrated by a dog with megaesophagus. It may be weeks to months before regurgitation begins to occur in these cases.
Weight loss and emaciation occur secondary to inadequate food intake. Inappetence or salivation or both may result from discomfort caused by esophagitis.
In patients in which megaesophagus is associated with an underlying disorder, other clinical abnormalities that may be noted include generalized muscle weakness (myasthenia gravis, polymyopathy, hypoadrenocorticism), neurologic deficits (myasthenia gravis, central nervous system disease, polyneuropathy), generalized muscle atrophy or pain with polymyositis, vomiting (hypoadrenocorticism, lead poisoning, obesity and alopecia with hypothyroidism, and oropharyngeal dysphagia with generalized neuromuscular dysfunction).
Physical Examination
The most common physical finding in dogs with adult-onset idiopathic megaesophagus is loss of body condition. In some patients weight loss is pronounced by the time a definitive diagnosis is made (Figure 4-3). Mucopurulent nasal discharge and fever suggest aspiration pneumonia. Pulmonary crackles may be detected on auscultation. A Valsalva maneuver, in which the thorax and the mouth are occluded while the thorax is compressed to increase intrathoracic pressure, often results in a bulging on the left side of the neck caused by a dilated cervical esophagus. Oral examination may reveal the presence of accumulated food particles or thick saliva in the pharynx. The presence of muscle atrophy, weakness, or abnormal gait suggests the possibility of a neuromuscular disorder. A complete neurologic examination should
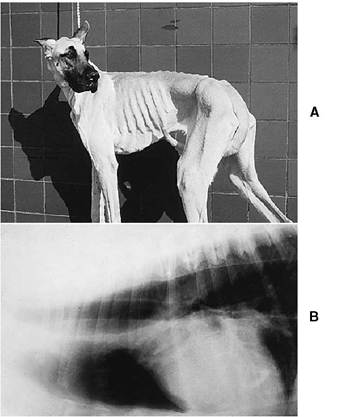
Figure 4-3 Adult-onset idiopathic megaesophagus in a 6-year-old Great Dane. Before referral the dog had undergone an extensive diagnostic work-up for vomiting. The primary problem, however, was actually regurgitation. A, Note the dog’s obvious cachectic condition. B, A thoracic radiograph confirms a diagnosis of megaesophagus (note the dilated, air-filled esophagus).
be performed, with emphasis on cranial nerves IX (glossopharyngeal) and X (vagus).
Diagnosis
Acquired megaesophagus is most commonly diagnosed by the presence of generalized esophageal dilation on survey thoracic radiographs, without evidence of obstruction. If cervical radiographs are obtained, dilation of the cervical esophagus will usually be noted as well. Contrast studies (liquid barium) are occasionally necessary to confirm the presence of a dilated, hypoperistaltic esophagus. In many patients with obvious megaesophagus, it is unnecessary to perform contrast studies. The risk of aspiration of contrast material must always be considered. I most commonly perform a contrast study when I suspect an esophageal motility disorder and when the thoracic esophagus is not readily recognized on survey films. The technique for contrast radiography of the esophagus is discussed in Chapter 2.
Occasionally dogs with megaesophagus are first presented because of symptoms related to aspiration pneumonia. Therefore when evaluating thoracic radiographs from dogs with pneumonia, one must always look closely for any evidence of esophageal dilation.
Once the presence of megaesophagus is confirmed, appropriate ancillary tests should be performed. A complete blood count, a complete biochemical profile (including creatine kinase [CK]), and total serum thyroxine levels should be evaluated in all cases (TT4). Leukocytosis (neutrophilia) with or without a left shift is consistent with aspiration pneumonia. Biochemical tests of particular interest include evaluations of sodium and potassium (hyponatremia and hyperkalemia are present in approximately 90% of dogs with hypoadrenocorticism); CK and aspartate transaminase (AST) (which may be elevated in patients with polymyositis); and cholesterol (hypercholesterolemia may suggest the possibility of hypothyroidism). In addition to baseline serum thyroxine level evaluation, free T4 by equilibrium dialysis (f T4ED) and a canine thyroid-stimulating hormone (cTSH) assay can also be done to more thoroughly examine for hypothyroidism. An acetylcholine receptor antibody titer should also be obtained in all adult dogs with megaesophagus to test for focal myasthenia gravis. Focal myasthenia gravis occurs in the absence of muscle weakness. This is probably the second most common cause of acquired megaesophagus (a greater number of cases are idiopathic). Megaesophagus secondary to acquired myasthenia gravis is described in more detail later in this chapter.
Other tests that the clinician should consider in the evaluation of patients with megaesophagus, depending on clinical course and physical findings, include the following:
Adrenocorticotropic Hormone Stimulation Test for Hypoadrenocorticism. Hypoadrenocorticism is an uncommon cause of megaesophagus. Proposed causes of esophageal dilation include the effects of abnormal sodium and potassium concentrations on membrane potential and neuromuscular function, as well as a physiologic deficiency of cortisol, which may cause muscle weakness.
Hypoadrenocorticism has a predilection for young to middle-aged females. The most common clinical signs include anorexia, vomiting, lethargy, and weakness. Diarrhea also may occur. Most dogs that have megaesophagus associated with hypoadrenocorticism demonstrate one or all of these signs in addition to regurgitation. However, occasionally there may be only regurgitation. In addition, some of these dogs have atypical hypoadrenocorticism, in which sodium and potassium levels are normal. This complicates the diagnosis, so the clinician must maintain a high index of suspicion. An adrenocorticotropic hormone (ACTH) stimulation test is required for diagnosis. ACTH stimulation should also be performed to confirm the diagnosis in patients with characteristic hyponatremia and hyperkalemia. With proper treatment the megaesophagus will most likely resolve.
Tests for Hypothyroidism: fT4ED and cTSH Assay. It has been proposed that megaesophagus may be associated with hypothyroidism. Very few dogs with hypothyroidism appear to develop megaesophagus. Tests including an f T4ED and cTSH assay are warranted if baseline thyroid tests are subnormal. However, it is considered to be a rare occurrence for megaesophagus to resolve in response to treatment for hypothyroidism. Occasionally, a patient may have both hypothyroidism and focal myasthenia gravis. It is possible that the focal myasthenia gravis could resolve either spontaneously or as a result of treatment for hypothyroidism, with megaesophagus resolving as well.
Blood Lead Level for Lead Poisoning. Sources of lead include old paints, toys, lubricants, hobby materials, automotive materials, plaster board, roofing materials, fishing sinkers, and improperly glazed dishes.Young (less than 1 to 2 years), inquisitive patients are most commonly affected. Clinical signs of lead toxicity often include both gastrointestinal (GI) and neurologic abnormalities. Anorexia, vomiting, diarrhea, and/or abdominal pain are often demonstrated. Regurgitation occurs in patients that develop esophageal hypomotility and dilation secondary to lead toxicosis (a careful review of the history is necessary to determine that both regurgitation and vomiting, rather than vomiting alone, are occurring). Megaesophagus is not common in patients with lead toxicity. Neurologic abnormalities may range from sudden epileptic seizures to a variety of behavioral changes, including excitability, hysteria, continued barking or whining, dullness, and apparent blindness. A blood lead level of greater than 40 μg∕dl is suggestive of lead poisoning, and a level of greater than 60 μg∕dl is diagnostic. Abdominal radiographs may reveal radiopaque material in the GI tract, and there may be nucleated red blood cells and basophilic stippling on stained blood smears. In most cases administration of the antidote of choice (calcium ethylenediaminetetraacetic acid) is sufficient to correct the clinical manifestations of lead toxicity. If treated early enough, megaesophagus will resolve.
Antinuclear Antibody and Lupus Erythematosus Tests for Systemic Lupus Erythematosus. In my experience, systemic lupus erythematosus (SLE) is an uncommon cause of megaesophagus in patients. Antinuclear antibody (ANA) tests performed on patients with megaesophagus are rarely positive. Physical findings that should prompt the clinician to test for SLE as a cause of megaesophagus include gait abnormalities (e.g., stilted gait, shifting limb lameness), joint swelling or pain (polyarthritis), muscle pain (polymyositis), concurrent evidence of immune-mediated hemolytic anemia or immune- mediated thrombocytopenia, and skin lesions, which may include ulceration, erythema, crusting, and alopecia. Nonspecific signs of SLE may include weakness, lethargy, and anorexia.
Edrophonium Chloride (Tensilon) Challenge Test for Myasthenia Gravis. This test is used to detect generalized myasthenia gravis or, if a decreased or absent palpebral reflex is found on physical examination, focal myasthenia gravis. Most patients with generalized myasthenia gravis are thought to have at least some degree of esophageal dysfunction, ranging from mild hypomotility to megaesophagus. The most common clinical signs of generalized myasthenia gravis are episodic weakness and decreased exercise tolerance. Difficulty with barking and with swallowing and prehending food also may be present. Mild cases may be difficult to differentiate from polymyositis, in which decreased exercise tolerance, dysphagia, and regurgitation associated with megaesophagus also may occur. Edrophonium chloride, a short-acting anticholinesterase drug, given at a dose of 0.05 to 0.1 mg/lb intravenously usually produces dramatic improvement in patients with myasthenia gravis that have collapsed or that are exercise intolerant. The response occurs within 1 to 2 minutes but lasts only for several minutes.
All dogs with myasthenia gravis should be tested for hypothyroidism, since it is estimated that 20% of dogs with myasthenia gravis will concurrently have hypothyroidism.
Electromyography. This study may be useful in the diagnosis and the differentiation of polymyopathy, polymyositis, myasthenia gravis, and polyneuropathy. For example, in myasthenia gravis, electromyography (EMG) and nerve conduction velocity studies are usually normal. On repetitive nerve stimulation, a decremental response is seen that is most characteristic of myasthenia gravis. The decremental response disappears when edrophonium chloride is given. EMG in patients with polymyositis may demonstrate positive sharp waves, fibrillation potentials, and bizarre high- frequency discharges. There is no decremental response to repetitive nerve stimulation, which differentiates polymyositis from myasthenia gravis.
In most patients with megaesophagus, endoscopic examination is not necessary for diagnosis and is rarely beneficial in determining a cause for the disorder. Patients with mild esophageal motility disorders may have a completely normal endoscopic examination; alternatively, there may be various degrees of fluid pooling. In contrast, patients with megaesophagus almost always demonstrate fluid retention and often small to moderate amounts of food residue. Many patients with megaesophagus have grossly normal esophageal mucosa. However, in some patients there may be evidence of esophagitis (e.g., mucosal erosions, patchy erythema, or focal hemorrhage occurring secondary to mucosal contact with the endoscope tip), which is most likely related to putrefaction of retained contents or reflux of gastric acid and activated enzymes. The two primary rule-outs for patients with megaesophagus that become inappetent are pneumonia and esophagitis.
Treatment
The main objectives of treatment for regurgitation disorders are to remove the initiating cause as early as possible, to minimize chances of aspiration of esophageal content, and to maximize nutrient intake to the GI tract. In most cases, idiopathic megaesophagus is incurable, and treatment involves an individually tailored feeding regimen, with the animal eating in an elevated position. Specific medical management is concurrently administered to patients with an associated disorder, such as myasthenia gravis, hypoadrenocorticism, SLE, polymyositis, and lead poisoning. Pneumonia is watched for carefully and treated aggressively if it occurs.
Patients with megaesophagus are best fed with the upper body in an elevated position of at least 45 degrees and, if possible, at a greater angle of elevation (Figure 4-4). Elevated feeding allows gravity to assist entry of food into the stomach. It is important that proper positioning be clearly demonstrated to the owner so that there is no misunderstanding about what has to be done. Otherwise, some owners will mistakenly think that elevated feeding simply means making sure that the head, rather than the entire upper body, is raised during feeding.
Significant difficulty may be experienced when one attempts to hold medium to large dogs with
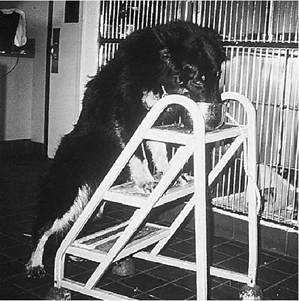
Figure 4-4 Ideal position for elevated feeding in a dog with megaesophagus. The dog was trained to remain on the ladder after it was finished eating until it was told to get down.
rear limb arthritis in a proper position. It is usually best to coax these dogs to sit down on their haunches while the owner stoops or kneels behind and helps hold the dog's body up by reaching around and supporting the sternum area. Food is placed on a table, a chair, or an elevated platform. The caregiver can reach around the dog to control the position of the food bowl if necessary. It is important to use a structure that is large enough for the patient to situate its front legs comfortably and strong enough to support its weight as it eats. Attention must also be directed toward controlling joint pain associated with arthritis as completely as possible. The more comfortable an arthritic patient is, the easier it will be for it to eat in the required position. Dedicated animal owners can almost always find a way to get the job done properly. Some owners build special platforms; others train their dogs to get into position with no assistance and stay until a command is given to get down. Giant-breed dogs such as Irish wolfhounds and Great Danes often do well when fed on indoor or outdoor house steps. Special “highchairs” have also been devised to aid in positioning and holding dogs upright (Figure 45). A shoulder harness can also be used for small dogs (Figure 4-6).
Cats rarely develop megaesophagus. Those that do often tolerate elevated feedings well. These feedings are accomplished either by holding the cat as demonstrated in Figure 4-7 or by supporting the animal from behind. I am also aware of cats that have been trained to eat in an elevated position (Figure 4-8).
The elevated position should be maintained for a full 10 minutes after food ingestion is completed. The importance of maintaining the elevated position for a sufficient time must be emphasized to the owner. Since the esophagus is virtually never completely empty in a patient with megaesophagus, it is often helpful to hold the patient in an elevated position for 5 to 10 minutes some time between meals and at bedtime. Nothing is fed at these times. I ask all my clients to do at least the bedtime elevation so that the esophagus will be as empty as possible before an expected period of prolonged recumbency. Some dogs regurgitate more during late evening and nighttime. This extra elevation maneuver often helps decrease the frequency of regurgitation significantly.
Patients with megaesophagus ideally are fed two to four times daily. This depends, of course, on the caregiver's time constraints. I have had the best success feeding soft-moist to solid (chopped) canned
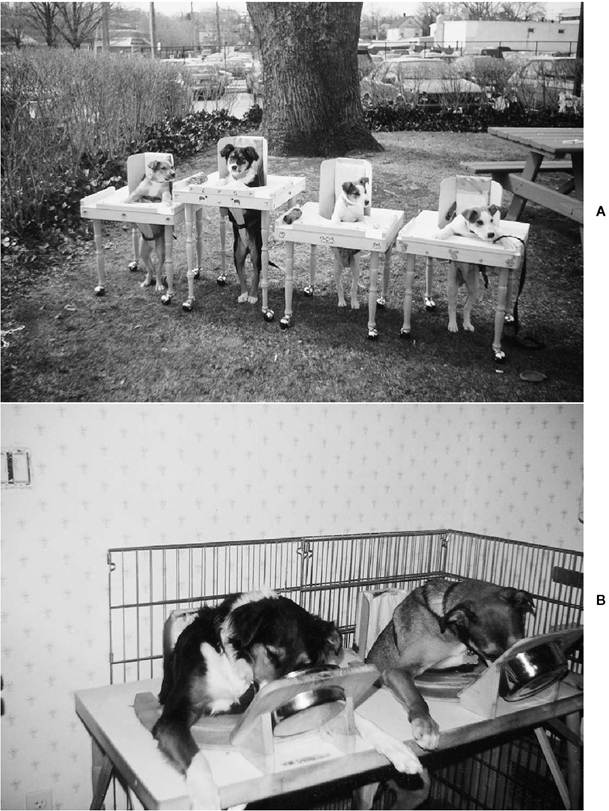
Figure 4-5 A, Specialized feeding chairs for dogs with megaesophagus. These chairs were designed by Donna Imhoff, a veterinary technician who has substantial experience in managing dogs with megaesophagus, and her husband. The chair provides full upright support for dogs to facilitate both feeding and holding them comfortably upright for the desired amount of time after they have eaten. The chair can be adjusted to accommodate patients of various sizes. Use of these chairs has the additional advantage of freeing the pet’s owner from having to physically hold the patient in an upright position, and thus it is also more likely that the patient will be kept upright for the full recommended period of time. B, A tilt feature can be added to the highchairs to make it easier for the patient to reach the food bowl. (Courtesy Donna Imhoff, North Shore Animal League, Port Washington, NY.)
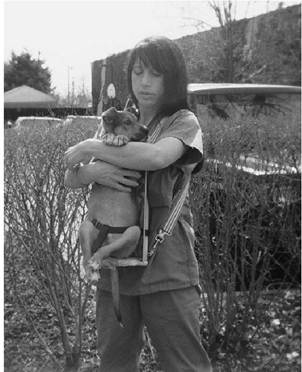
Figure 4-6 Use of a shoulder harness with a platform and restraint strap is another available means of feeding patients with megaesophagus. (Courtesy Donna Imhoff, North Shore Animal League, Port Washington, NY.)
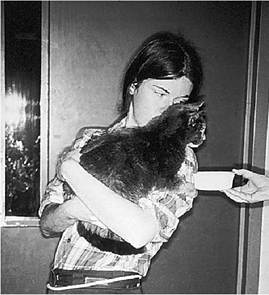
Figure 4-7 Elevated feeding position for a cat with megaesophagus. This 15-year-old cat had generalized gastrointestinal hypomotility. It had become hypothyroid after bilateral thyroidectomy for hyperthyroidism. The cat did not regurgitate as long as it ate in an elevated position. Thyroid supplementation did not improve gastrointestinal motility in this cat.
food. I recommend trying gruels only if the semimoist consistency is not well tolerated. Some dogs do not do well at all on liquid gruel diets, and this food consistency may be more easily aspirated. Some dogs do best when fed a series of “meatballs” fashioned from canned food. Others can tolerate dry food fairly well, either with or without water added to the food. The important point is that each patient can respond to various food consistencies in different ways. Owners should be instructed to conduct food trials in order to determine the best regimen for their own pet.
Specific pharmacologic agents have been used in efforts to improve esophageal emptying. The promotility drug metoclopramide has been ineffective in my experience. Metoclopramide can increase lower esophageal contractions slightly in normal patients but does not improve contractile activity in patients with megaesophagus. Nifedipine is a calcium channel antagonist that promotes relaxation of the LES. It was tried with the thought that decreasing LES tone might make it easier for the esophagus to pass food into the stomach. Calcium channel antagonists, however, can cause serious side effects, and there is no evidence that they are of any value in the treatment of megaesophagus. Their use is therefore not recommended.
The GI prokinetic drug cisapride is a benzamide derivative that promotes GI motility, increases antroduodenal coordination, and enhances LES tone. It has broader promotility effects than metoclopramide does. Cisapride has promotility effects in the esophagus of cats (distal esophagus where there is smooth muscle), the stomach, the small intestine, and the large intestine. It increases LES pressure, the amplitude of contractions in the distal esophagus, and the rate of gastric emptying. Cisapride, in theory, is likely to be of little benefit in dogs with megaesophagus because it stimulates smooth muscle motility and the canine esophagus is almost exclusively striated muscle. However, cisapride has been found to be helpful in decreasing significantly the frequency of regurgitation in several dogs with megaesophagus in our hospital series. These were cases that were being managed very diligently by their owners with elevated feeding programs but with poor responses (i.e., there was an ongoing high frequency of regurgitation). Concurrent with the institution of cisapride
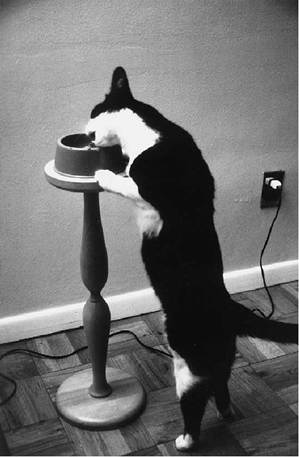
Figure 4-8 This cat had a regurgitation disorder and did quite well on an elevated feeding program. The cat learned to eat in a fully elevated position and regained lost weight rapidly once able to hold its food down. (Courtesy Dr. William Tepper.)
there was a dramatic decrease in the frequency of regurgitation. In one dog—a 14-year-old Labrador retriever cross with idiopathic megaesophagus, bilateral coxofemoral degenerative joint disease, and mild degenerative myelopathy—there was an ongoing high frequency of regurgitation (16 to 20 times per day despite a strict elevated feeding program). Once cisapride was instituted, the number of regurgitation episodes decreased to only one or two per day. This excellent response lasted 7 months, at which time the dog was euthanized because of its inability to walk due to severe degenerative myelopathy.
I am aware of anecdotal reports from academic institutions and private practices describing case histories in which cisapride has been effective in reducing the frequency of regurgitation in dogs with megaesophagus. In occasional cases the improvement has been dramatic. In other cases there has been minimal or no clinical improvement. In most cases it is not likely that the megaesophagus will be reduced with cisapride therapy. Presumably, the increase in motility in patients that have a positive response is, with elevated feedings, sufficient to improve esophageal emptying into the stomach.
The most common and severe complications of megaesophagus are aspiration pneumonia and significant weight loss. Most debilitated dogs with megaesophagus are quite hungry, but frequent regurgitation prevents them from being able to deliver enough food to their stomach. Another concern is that cachectic patients are immunocompromised and are unable to respond strongly to infection. It is often best to begin feeding debilitated megaesophagus patients through a gastrostomy tube, unless there is a very good initial response to elevated feedings at the time the diagnosis is established. Gastrostomy tube feeding bypasses the diseased esophagus and allows adequate caloric replacement. This is also an option in cases in which frequent regurgitation persists, with or without aspiration. Another advantage is that all required medications can be administered directly to the stomach through the tube. Gastrostomy tubes can be quickly placed under endoscopic guidance (e.g., percutaneous endoscopic gastrostomy, see Chapter 12). During tube placement, the esophageal mucosa can be concurrently evaluated for evidence of esophagitis. Surgical placement of a gastrostomy tube can also be done (see Chapter 12). The risks of general anesthesia must be considered. Precautions must always be taken in patients with megaesophagus to ensure that steps are taken to avoid aspiration during induction and recovery.
The length of time for which a feeding tube is left in place varies. Some dogs gain weight fairly quickly and respond well on an elevated feeding program with or without promotility therapy. In these cases the tube is often removed after 1 to 2 months. In other dogs tube feeding is the only possible way of successfully feeding on a long-term basis. Some large- breed dogs have been fed by gastrostomy tube for as long as 2 to 3 years. Periodic tube replacement is necessary in these dogs. The initial feeding tube is usually replaced with a “low profile” tube, which sits flush with the body wall (see Chapter 12). Complications related to gastrostomy tubes that could potentially cause significant problems in patients with megaesophagus include vomiting and gastroesophageal reflux. Many dogs with megaesophagus do well without ever having a gastrostomy tube placed. In summary, the two main indications for use of a gastrostomy tube are (1) significant weight loss with ongoing regurgitation despite elevated feedings and (2) aspiration pneumonia, in which it is best to avoid using the esophagus until the pneumonia is resolved and it is demonstrated that persistent regurgitation will not be a problem.
Treatment for aspiration pneumonia includes aggressive fluid therapy, antibiotics, coupage, nebu- lization, and nutritional support. Ideally, a tracheal wash should be done in patients with moderate to severe pneumonia as soon as the diagnosis is made. The initial choice of one or more antibiotics depends on cytologic studies and Gram stain results. The use of bactericidal antibiotics with a good gram-negative spectrum is recommended pending culture and sensitivity results. Trimethoprim-sulfonamide (Tribrissen) and enrofloxacin (Baytril) are good initial choices for mild pneumonia. Patients with mild pneumonia can often be treated with oral antibiotics on an outpatient basis.
If moderate to severe bacterial pneumonia is present and there is marked respiratory insufficiency, aggressive antimicrobial therapy should be instituted immediately. This usually involves combination therapy using cephalosporins (e.g., ce- fazolin [Kefzol], 10 to 15 mg/lb every 8 hours intravenously or intramuscularly, or cefoxitin [Mefoxin], 10 to 15 mg/lb every 6 to 8 hours intravenously) and aminoglycosides (gentamicin [Gentocin], 1 to 2 mg/lb intravenously or subcutaneously every 6 to 8 hours or 2.7 to 4.5 mg/lb intravenously or subcutaneously once every 24 hours, or amikacin [Amiglyde-V] 3 mg/lb every 8 hours or 9 mg/lb once every 24 hours intravenously, intramuscularly, or subcutaneously). Alternatively, imipenem (Primaxin) provides excellent four-quadrant coverage. Imipenem is administered as sole antimicrobial therapy at 2.5 to 5 mg/lb intravenously every 8 hours. Imipenem is a beta-lactam antibiotic. Beta-lactam agents have little if any dose-dependent toxicity. Imipenem has the same toxicity potential as that of other pen- cillins (e.g., ampicillin). The best use of this drug is in patients with renal compromise that cannot be given aminoglycosides safely. If the creatinine level is greater than 4 mg/dl, imipenem is administered at 12-hour, rather than 8-hour, intervals. Imipenem should be delivered over 30 minutes in the intravenous line.
Oral administration of antibiotics is contraindicated in seriously ill patients because of their low and erratic serum levels. There are also problems in ensuring that the medication is transported in a timely manner to the stomach in a patient with megaesophagus.
As previously mentioned, patients with megaesophagus occasionally develop esophagitis. The primary signs of esophagitis are decreased appetite and lethargy. Salivation also may be evident. Esophagitis should be suspected once pneumonia is ruled out. Treatment may include administration of a sucralfate (Carafate) suspension or H2-receptor antagonist therapy to lower gastric acid levels or both. A proton pump inhibitor (e.g., omeprazole, lansoprazole, esomeprazole) is used to completely block acid release in patients with moderate to severe esophagitis, instead of an H2-receptor antagonist. There is often rapid improvement once specific treatment is instituted. Duration of therapy depends on patient response. Management of esophagitis is discussed in more detail later in this chapter.
Dogs that seem to experience frequent bouts of mild pneumonia sometimes do best when maintained on long-term antibiotic therapy. In these cases, the antibiotics used are often rotated every 6 to 8 weeks. Likewise, an H2-receptor antagonist or proton pump inhibitor is sometimes used on a long-term basis in dogs with chronic esophagitis.
Too often patients with megaesophagus are quickly assigned a poor prognosis. Granted, some patients do poorly on any form of therapy and euthanasia may unfortunately be inevitable. However, many patients with megaesophagus can be successfully managed for months to years. Owners who are willing to invest time and effort in the care of their pet with megaesophagus are often rewarded. To highlight this point, three cases of note are presented in Figures 4-9 and 4-10.
Megaesophagus Secondary to Acquired Myasthenia Gravis Clinical Signs
Myasthenia gravis occurs both as an acquired autoimmune disorder and as a congenital, familial one. Acquired myasthenia gravis is an autoimmune disorder of neuromuscular transmission resulting from the actions of autoantibodies against nicotinic acetylcholine receptors at neuromuscular junctions. Conjointly there is complement medi-
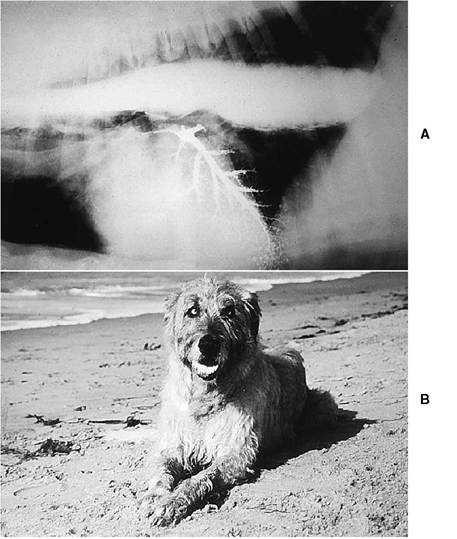
Figure 4-9 A, Contrast radiograph of an 8-year-old Irish wolfhound with adult-onset idiopathic megaesophagus. Note that there was aspiration of a small amount of barium into the airways. The dog was presented because of regurgitation. There was an excellent response to elevated feedings (the owner used a ladder and helped support the dog from the side). The diet consisted of kibble soaked in water. B, Photograph of the dog taken 5 months after the diagnosis was made. The dog regurgitated on average only two times per week.
ated destruction of the junction folds, altering the neuromuscular junction formation, or it may accelerate the internalization and the degradation of the acetylcholine receptor. Myasthenia gravis manifests itself in several clinical forms:
• Generalized myasthenia gravis: Manifests predominantly as tetraparesis, but there may be primarily pelvic limb paresis.
• Focal myasthenia gravis: Affects the cranial nerves mainly around the larynx and pharyngeal region.
• Acute fulminant myasthenia gravis: Flaccid tetraparesis, acute respiratory distress.
Megaesophagus associated with generalized myasthenia gravis has been well documented. Clinical signs include premature fatigue during exercise (manifested by a spastic pelvic limb gait followed by tetraparesis and then collapse), tachypnea and dyspnea, and sialosis. More recently, a focal form of myasthenia gravis, in which megaesophagus occurs in the absence of detectable generalized weakness, has been recognized. The primary clinical sign is regurgitation. Other clinical signs that may occasionally be observed in focal myasthenia gravis include pharyngeal and laryngeal muscle weakness (dysphagia and dyspnea), weakness of the facial muscles, and a decreased palpebral reflex. In some dogs there is a change in the quality of the bark or an inability to bark. A myopathy or a neuropathy should always be considered as a differential diagnosis in laryngeal or pharyngeal problems.
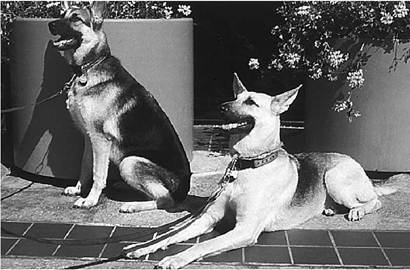
Figure 4-10 Two young German shepherd dogs with esophageal motility disorders. The dog on the left had congenital megaesophagus (also shown in Figure 4-1). Persistent right aortic arch was diagnosed in the dog on the right at 4 months of age. Surgery was successful in relieving the esophageal obstruction, but esophageal dilation persisted. The dogs are not related. Each of these dogs was adopted and cared for by a veterinarian on our staff. Note their excellent body condition. Long-term treatment for megaesophagus included twice daily elevated feedings. The diet consisted of a mixture of kibble, canned food, and water blenderized to an oatmeal consistency. Regurgitation rarely occurred, and both dogs remained highly energetic.
Diagnosis
Several large groups of affected dogs have been reported in the literature. In one group 40 of 152 dogs (26%) with megaesophagus were found to have elevated serum antibodies to acetylcholine receptors, diagnostic of acquired myasthenia gravis. Many breeds were affected, but Golden retrievers (7 of 20,35%) and German shepherds (8 of 25, 32%) were the breeds most commonly involved.
A diagnosis of acquired myasthenia gravis is established by demonstration of circulating antibodies against canine acetylcholine receptors by immunoprecipitation radioimmunoassay. An antibody titer greater than 0.6 nmol/L is diagnostic for acquired myasthenia gravis in dogs, whereas a value of greater than 0.3 nmol/L is diagnostic in cats. This test should be performed in all patients with acquired megaesophagus. This assay is particularly valuable in cases of focal myasthenia in which muscle weakness is localized to esophageal or pharyngeal musculature and generalized weakness is not present. Serial serum antibody titers are also important in following a patient's clinical response to treatment.
The acetylcholine receptor antibody titer assay is available at the Comparative Neuromuscular Laboratory.[‡‡] A blood sample is drawn into a red top tube and allowed to clot at room temperature. The sample is centrifuged as soon as possible after clotting has occurred. The serum is removed and refrigerated until the time of shipping. At least 1 ml (preferably 2 ml) of serum should be sent to the laboratory on a cold pack by an overnight mail service.
The edrophonium chloride challenge test may be useful in helping establish a presumptive diagnosis of focal myasthenia gravis in some dogs, especially those with a decreased or absent palpebral reflex. The administration of edrophonium chloride (0.05-0.1 mg/lb intravenously) may result in an improved blink reflex.
Treatment
Treatment includes drug therapy in conjunction with a standard elevated feeding program, as is done with any patient with megaesophagus. The cornerstone of treatment in generalized myasthenia gravis is anticholinesterase therapy. Pharmacologic management (anticholinesterase drugs or corticosteroids or both) may also be helpful in dogs with focal myasthenia gravis. Recent reports have highlighted azathioprine as an effective immunosuppressive drug for management of myasthenia gravis (see subsequent discussion).
In general, the following recommendations for pyridostigmine can be made. Careful monitoring is essential to the prevention of anticholinesterase overdose. Injectable neostigmine (Prostigmin) can be given at a dose of 0.2 mg/lb intramuscularly every 6 hours if administration by mouth or by gastrostomy tube is not possible or advisable (e.g., patients with frequent regurgitation should be treated initially with injectable medication because orally administered medication may not be transported to the stomach). Once oral medication can be tolerated, pyridostigmine bromide syrup or tablets (Mestinon) are administered at 0.25 to 1.5 mg/lb every 8 to 12 hours per os (start at the low end for focal myasthenia gravis patients because clinical response may be difficult to evaluate). Signs of overdose include muscle weakness, salivation, miosis, vomiting, and diarrhea. Administration of pyridostigmine may result in a decrease in clinical signs of regurgitation. Careful surveillance for the development of aspiration pneumonia is maintained at all times.
Corticosteroids may benefit some patients with myasthenia gravis. Corticosteroids alter macrophage function by inhibiting antigen processing and thus inhibiting interleukin-1 (IL-1) release. This alters B cell function. Corticosteroids also suppress interleukin-2 (IL-2) synthesis and thus alter T cell proliferation. Positive effects include enhanced presence of acetylcholine receptors, acetylcholine synthesis, and enhanced organization of the post- synaptic membrane.
Corticosteroids may cause some potentially negative effects in myasthenia patients, especially when used in high doses. Corticosteroids may actually antagonize acetylcholine and create a neuromuscular junction blockage effect of the acetylcholine receptor channel, which may then uncouple the excitatory processes. In some cases prednisone may actually create a fulminating myasthenic crisis.
Corticosteroids are instituted at immunosuppressive doses. It is recommended that steroids be started slowly, with an initial dose of 0.25 mg/lb of prednisone per day, divided BID. The dose is gradually increased over the next 5 days to 1 mg/lb per day. If aspiration pneumonia is present, administration of corticosteroids is avoided until the pneumonia has resolved. Caution must also be exercised when corticosteroids are used in conjunction with anticholinesterase drugs, since muscle weakness can be exacerbated by such treatment. It is difficult to assess the effectiveness of corticosteroids accurately because many dogs with focal myasthenia gravis reportedly go into spontaneous remission in the absence of any drug treatment. Some clinicians, including myself, have observed dogs with focal myasthenia gravis that have demonstrated dramatic positive responses to corticosteroids. In some patients long-term, low-dose therapy has been required for control of symptoms, whereas in others medication has been successfully discontinued.
Recently there have been favorable reports about azathioprine as an effective form of therapy for myasthenia gravis. Azathioprine is an immunosuppressive drug that binds to and interferes with synthesis of ribonucleic acid (RNA) and deoxyribonucleic acid (DNA) and therefore alters T cell proliferation after antigenic stimulation. Azathioprine affects both cell mediated and humoral responses. It is thought to have more of an affect on the cell mediated side.
The recommended regimen is 0.5 mg/lb orally once daily for 14 days, followed by an increase to 1 mg/lb per day. The idea is to slowly suppress the immune response. Azathioprine has a delayed onset of action of 3 to 4 weeks or so. Pyridostigmine may be needed for a while to be used in conjunction with azathioprine. The acetylcholine receptor antibody (AcRAb) titer should be checked monthly during therapy. When clinical signs have resolved and there has been normalization of acetylcholine receptor antibody levels azathioprine is reduced to an every other day schedule. The titer should still be monitored once monthly.
Side effects to azathioprine are uncommon when it is used at the recommended dose. The major effect to watch for is bone marrow suppression. A baseline complete blood count (CBC) and platelet count are followed by recheck tests at 3 and 6 weeks, then every 2 months. Azathioprine is discontinued if the neutrophil count drops below 1,000∕μl. Other uncommon but potential side effects include GI irritation, hepatotoxicity, drug induced pancreatitis, and slow hair growth.
Remission can be induced in most dogs, but relapses may occur. Three out of five patients in one report experienced complete remission of clinical signs within 3 months of therapy. Further studies to evaluate monotherapy with azathioprine and combination therapy with azathioprine and pyridostigmine or azathioprine, prednisone, and pyridostigmine are needed.
The course of focal myasthenia gravis is variable. Some affected dogs might progress to generalized myasthenia gravis, but if this is going to happen it generally occurs within the first few weeks after onset of clinical signs. Radiographs are also obtained periodically to monitor esophageal size. Esophageal function may return to normal, but remission may require days to months. Owners should also be warned that the disease may recur.
Several clinicians have reported seeing an occasional dog with both hypothyroidism (confirmed by a TSH response test) and focal myasthenia gravis. In some cases the myasthenic condition resolved after treatment for hypothyroidism was instituted.