vascular ring ANOMALIES
Vascular ring anomalies are congenital malformations of the great vessels and their branches that entrap the intrathoracic esophagus and cause obstruction. Although a number of different congenital vascular ring anomalies can occur in dogs and cats, persistent right aortic arch (PRAA) is by far the most common (95%).
Other anomalies that have been reported include persistent right ductus arteriosus, aberrant left or right subclavian arteries, double aortic arch, and esophageal compression by the left subclavian and brachiocephalic arteries (found in English bulldogs). Vascular rings are quite uncommon in cats.In PRAA the right rather than the left fourth aortic arch forms the functional adult aorta. The esophagus becomes entrapped by the aorta on the right, by the pulmonary trunk on the left, by the ligamentum arteriosum dorsolaterally on the left, and by the base of the heart ventrally (Figure 4-11).This anatomic “ring” results in obstruction and progressive dilation of the esophagus cranial to the base of the heart.
Vascular ring anomalies are inherited. There is a breed predilection for German shepherds and Irish setters. There is also a higher than expected incidence among Boston terriers and English bulldogs. There is no reported breed predilection for cats. Multiple puppies in a litter may be affected. Breeding affected patients is not recommended.
Clinical Signs
The most common clinical sign in puppies and kittens is an acute onset of regurgitation at or shortly after the time of weaning to solid foods. In patients that do not show significant signs around the time of weaning, the diagnosis will almost always be made by 6 months of age. Rarely, significant clinical signs may not be apparent until later in life. As the proximal esophagus becomes more dilated, food may be retained for longer periods before regurgitation occurs.
Affected patients become malnourished and weak and are smaller than their littermates. Coughing with respiratory distress is common and indicates a secondary aspiration pneumonia.Diagnosis
The primary differential diagnosis for vascular ring anomaly is congenital megaesophagus. Foreign body obstruction also should be considered. Diagnosis is based on survey and contrast radiography of the thorax. Survey radiographs of vascular ring anomaly show esophageal dilation with food and air. The dilation tapers to normal at the base of the heart. With PRAA the normal opacity caused by the bulge of the aortic arch is absent. Contrast studies of vascular ring anomaly reveal a characteristic constricted appearance over the base of the heart, with variable degrees of esophageal dilation proximal to the site of obstruction. Fluoroscopy demonstrates a loss of motility of the proximal esophagus. Esophageal motility distal to the stricture is usually normal. In the rare instance that the diagnosis cannot be confirmed by radiography, esophagoscopy can provide useful information in differentiating a mural lesion from extraluminal compression. With extraluminal compression of the esophagus, a full circumference indentation may be seen from the lumen side. Endoscopy is also useful for ruling out esophageal foreign body and in removal if one is found. Foreign bodies can become lodged secondary to the PRAA.
Treatment
Definitive management of vascular ring anomaly is limited to surgical correction of the constricting band forming the vascular ring. For PRAA this involves ligation and transection of the ligamen- tum arteriosum.
It is best to stabilize and strengthen the patient as much as possible before subjecting it to a thoracotomy. Elevated feedings having a gruel consistency are given frequently and in small enough amounts to minimize regurgitation. A gastrostomy tube can be used if oral feeding is poorly tolerated. If pneumonia is present, it should be treated aggressively and resolved before surgery.
Internal
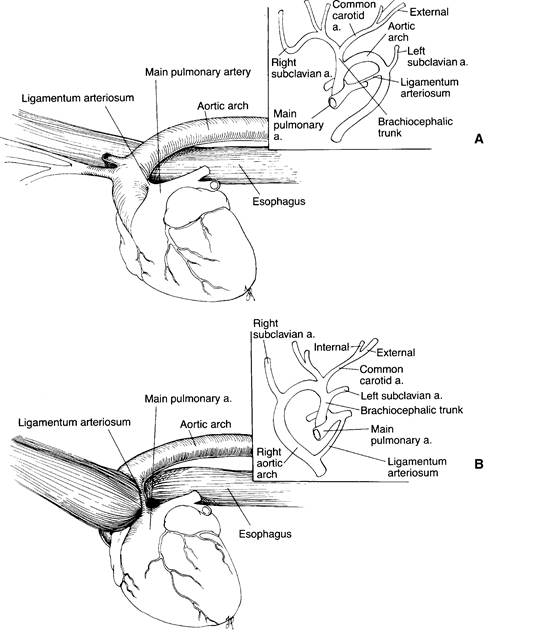
Figure 4-11 Persistent right aortic arch. A, Normal development of the aortic arch viewed from the patient’s left side. Inset shows normal embryonic development of the great vessels from a dorsoventral view. B, When the embryonic right fourth aortic arch becomes the adult aorta, esophageal constriction occurs. Inset shows dorsoventral view of the vascular malformation. (From Birchard SJ, Sherding RG, eds: Manual of small animal practice, ed 2, Philadelphia, 2000, WB Saunders.)
The prognosis for complete recovery after surgery is guarded to poor. Regurgitation of some degree persists in most dogs that undergo surgical correction. The esophageal dilation that exists early in the course of the disease persists to some degree indefinitely in most patients. In addition, esophageal dilation caudal to the vascular ring site can occur, possibly due to neuromuscular disease. Recovery of normal esophageal function is more likely when surgery is performed at an early age. Many patients significantly improve after surgery. If esophageal disease persists, an elevated feeding protocol should be followed. Surveillance for signs of aspiration pneumonia is always maintained.
A retrospective study examined whether the degree of esophageal dilation affects long-term outcome. Ten dogs and four cats with PRAA were studied through 6 months after surgery. Of all the animals, 35.7% (mean age 2.5 months) had a very good outcome, 42.9% (mean age 2.7 months) had a good outcome, and 21.4% (mean age 5.7 months, range 3 to 9 months) had a poor outcome. A measurement scheme was devised. After barium contrast esophagography the maximum diameter of the esophageal dilation cranial to the heart base (O ) was compared with the height of the body of the 5th thoracic vertebra at its narrowest point (T5). The degree of esophageal dilation was classified as mild, moderate, and severe on the basis of the ratio O : T. All measurements
e 5
were made to the nearest millimeter. The ratio of O :T5 for normal dogs and cats, based on esophageal contrast studies on 10 normal cats and 25 normal dogs, was considered to be less than or equal to 1. Mild dilation was considered to be less than or equal to 2.5, moderate less than or equal to 4, and severe greater than 4.
In this study a majority of the patients with a mild or moderate degree of dilation had a good to very good outcome after surgery. Of three patients that had a poor outcome (two cats and one dog), two had a severe degree of dilation (one cat and one dog), and one had a moderate degree of dilation. Although more animals must be evaluated using this scheme, it appears that the degree of preoperative esophageal dilation does affect the long-term outcome in patients with PRAA.