Molecular Testing for Infectious Diseases in Horses
Nicola Pusterla • Christian M. Leutenegger
The ready availability of a correct etiologic diagnosis, particularly in contagious infections, enables the veterinarian to make early decisions regarding the patient's care and management, address appropriate treatment, and allow timely notification and discussion of management issues pertaining to the prevention of disease spread.
The past 2 decades have seen a revolution in the understanding, management, diagnosis, control, and prevention of infectious diseases.1,2 This period has encompassed the discovery of emerging equine agents, antimicrobials, and vaccines, as well as a wealth of improved diagnostic tests for equine practitioners. Despite these advances, infectious diseases remain a leading cause of equine morbidity and mortality, with resurgence of certain infections (e.g., West Nile virus); an increasing population of elderly, more susceptible horses; and an increasing international equine commerce, expanding the geographic distribution of pathogens.3,4 The focus of rapid diagnosis of infectious diseases has also shifted during this time. The most obvious change has been the appearance and increasing importance of nucleic acid (NA) amplification-based techniques, primarily the polymerase chain reaction (PCR), at the expense of traditional methods of clinical microbiology.5 PCR has become an increasingly important tool in microbial diagnosis in recent years, mainly because of its rapidity, high sensitivity, and high specificity. These superior characteristics have propelled the field of PCR-based molecular diagnostics into the arena of applied diagnostics for infectious agents. Because the number of published and offered PCR assays is steadily rising, there is a need for critical evaluation, comparison of performance, and eventually standardization of methods to enable equine practitioners to select the optimal methodology.Sample Submission
NA techniques to detect the presence of infectious agents in biological specimens require stringent quality guidelines. These guidelines aim to ensure the stability of NAs (both genomic DNA and total RNA), which are the target for molecularbased diagnostic methods. Whole blood samples are collected aseptically into evacuated blood tubes containing ethylenediaminetetraacetic acid; body fluids (e.g., thoracic, abdominal, joint, cerebrospinal, tracheal wash, bronchoalveolar lavage, guttural pouch lavage fluid) and tissues should be collected into serum tubes without additives; nasal or nasopharyngeal secretions should be collected with rayon- or batting (Dacron, Invista, Wichita, Kan.)-tipped swabs and are best kept in a sterile serum or conical tube (virus transport medium is recommended for the detection of viruses); and fecal material should be collected into small fecal cups or serum tubes (Fig. 29.1; Table 29.1). All samples must be sent cooled on blue ice by express mail overnight to the laboratory. Freezing of samples should be avoided. Short-term storage for a period of 2 to 3 days before shipment (over a weekend) should be done in a refrigerated compartment. Each sample should be properly labeled and accompanied by a submission form containing information pertaining to the patient, owner, veterinarian, sample, and pathogen(s) to be tested (most submission forms can be downloaded from the respective laboratory website). The laboratory should be notified in advance, and inquiry should be made about the availability of the offered tests, as well as turnaround time and associated costs. Incoming samples normally are processed the same day, and PCR results usually are available within 24 to 48 hours if the NA passes quality control.
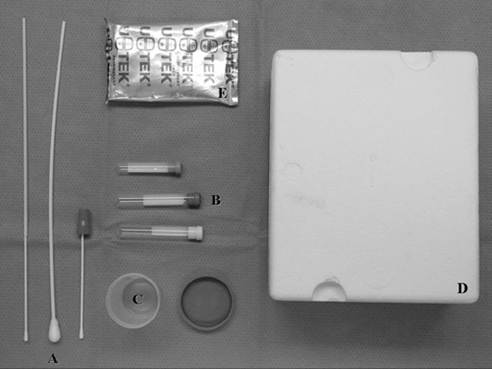
FIG. 29.1 Collection and shipping material routinely used to submit equine tissue samples for molecular detection. A, Three sterile swabs of different lengths.
B, Three sterile, evacuated tubes with and without additives. C, Sterile cup with lid. D, Styrofoam shipping container. E, Cooling element to keep the samples cooled.Clinical Applications
An array of NA amplification techniques may be offered by laboratories in order to establish an etiologic diagnosis of equine infectious diseases. Several published studies have shown the benefit of NA amplification techniques in comparison with conventional microbiological techniques. Current efforts are aimed at improvement of the diagnostic efficiency of molecular techniques, for both common and less common pathogens. To facilitate a decision on which pathogens should be evaluated for a specific case, some laboratories offer panels covering specific organ systems (e.g., respiratory, gastrointestinal, neurology, bloodborne). Such panels test several common pathogens for each organ system. Some of the diagnostic PCR applications most relevant for equine practice are presented as follows, along with their advantages and potential pitfalls.
RESPIRATORY PATHOGENS. Respiratory pathogens are often contagious, and infections must be diagnosed rapidly in order to prevent a disease outbreak and institute the appropriate management plan. The short turnaround time and reliability of PCR make this molecular technology an ideal tool for the diagnosis of respiratory pathogens.
Equine influenza is commonly diagnosed by virus isolation or detection from nasal or nasopharyngeal swabs collected from horses during the early febrile stage of the disease. Virus can be grown from nasal and nasopharyngeal swabs by inoculation and incubation of embryonated chicken eggs or passage through Madin-Darby canine kidney cells. Although isolation of the virus is essential to allow antigenic and genetic characterization of the strain, this technology is time consuming and successful isolation is, at best, to be expected in 50% of the cases. Further, since mutations have been reported to occur during the process of viral culture, recovered isolates must be viewed critically.
In recent years new methods for virus detection, such as antigen-detection enzyme-linked immunosorbent assays (ELISAs) and PCR, have been described. Collectively these detection methods have shown higher sensitivity than virus isolation and antigen-capture ELISAs.6-9 Amplification of the single-stranded RNA of equine influenza viruses is performed by reverse transcription-PCR (RT-PCR) technology, using a one-step, nested, or real-time approach. The hemagglutinin, nucleoprotein, and matrix gene are the commonly targeted genes for these molecular assays. Unfortunately,■ TABLE 29.1
Tissue Samples Commonly Used for Molecular Detection of Common Equine Pathogens
| Pathogen | Tissue Submission |
| Anaplasma | Whole blood |
| phagocytophilum | |
| Babesia caballi | Whole blood |
| Borrelia burgdorferi | CSF, CNS |
| Clostridium botulinum | Feces, gastrointestinal content, |
| Clostridium difficile | feed, wounds, and carrions Feces |
| (antigen and toxin A and B) | |
| Clostridium perfringens | Feces |
| Corynebacterium | Aspirate from abscess, body |
| pseudotuberculosis | fluid |
| Cryptosporidium spp. | Feces |
| Equine arteritis virus | NPS, uterine swab, placenta, |
| Equine coronavirus | aborted fetus, semen Feces |
| Equine herpesvirus 1 | NPS, whole blood, TW, BAL, |
| Equine herpesvirus 2 | CSF, CNS, uterine swab, placenta, aborted fetus NPS, whole blood, TW, BAL |
| Equine herpesvirus 4 | NPS, TW, BAL |
| Equine herpesvirus 5 | NPS, whole blood, TW, BAL |
| Equine influenza virus | NPS, TW, BAL |
| Equine rhinitis A virus | NPS, urine |
| Equine rhinitis B virus | NPS |
| Equine rotavirus | Feces |
| Lawsonia intracellularis | Feces, intestinal biopsy |
| Leptospira spp. | Urine, blood, uterine swab, |
| Neorickettsia risticii | placenta, aborted fetus Whole blood, feces |
| Neospora hughesi | CSF, CNS |
| Rhodococcus equi | TW, BAL, feces |
| Salmonella spp. | Feces |
| Sarcocystis neurona | CSF, CNS |
| Streptococcus equi subsp. | NPS, NPL, GPL, lymph node |
| equi | aspirate |
| Streptococcus equi subsp. | NPS, NPL, GPL, lymph node |
| zooepidemicus | aspirate |
| Theileria equi | Whole blood |
| West Nile virus | Whole blood, CSF, CNS |
BAL, Bronchoalveolar lavage fluid; CNS, central nervous system tissue; CSF, cerebrospinal fluid; GPL, guttural pouch lavage; NPL, nasopharyngeal lavage; NPS, nasal/nasopharyngeal swab; TW, tracheal wash fluid.
comparison of the different PCR assays is precluded by the use of different technologies, the lack of standardization among the assays, and variation in targeted genes. Nucleotide and deduced amino acid sequences of portions of the hemagglutinin gene are now routinely used for phylogenetic characterization of outbreak strains. Further, novel real-time PCR assays can be used as a viable replacement for the more traditional methods of quantifying equine influenza virus in vaccine efficacy studies. Another advantage of assays such as antigen-detection ELISAs and PCR is their ability to detect a nonviable virus, a situation that may occur when nasal or nasopharyngeal samples are frozen or not adequately stored and/or shipped to a diagnostic laboratory, allowing a rapid diagnosis in the acute phase of infection. Routine diagnostic testing for equine influenza virus does yet not allow differentiation between clade I and clade II viruses of the Florida sublineage.
EHV-1 and EHV-4 are important and widespread equine viral pathogens that cause important economic losses in the equine industry. Both are double-stranded DNA alphaherpesviruses that affect the equine respiratory tract and can establish lifelong latent infection after primary exposure. Traditionally, virus isolation has been the gold standard for diagnosing EHV-1 and EHV-4 infections. The sample of choice is a nasal or nasopharyngeal swab, which should be taken early in the febrile phase of the disease. The swabs should be kept in viral transport medium and shipped on ice to a veterinary diagnostic laboratory. Because of the lymphotropism of EHV-1, virus isolation can also be attempted from citrated or heparinized whole blood. Virus isolation requires the maintenance of specific cell culture lines, making this process relatively expensive and time consuming. EHV-1 can be propagated in a broad range of cell lines; however, EHV-4 grows only in cell lines of equine origin. Virus isolation is often hampered by the fragility of the virus, intermittent viral shedding, and interference with local antibodies.
PCR offers an alternative to virus isolation and has proven to be a sensitive method of detecting EHV-1 and EHV-4 in respiratory secretions, peripheral blood lymphocytes, and other tissues.10-12 Many PCR assays have been established to study the pathophysiology and improve the diagnosis of these viruses. Conventional one-step or nested PCR assays do have inherent risks of carry-over contamination as a result of postamplification steps required to detect the PCR products. Novel molecular platforms such as real-time qPCR have strongly reduced the risk of contamination. PCR assays used in routine diagnostics are based on the detection of viral genomic DNA and are therefore unable to distinguish among lytic, nonreplicating, or latent viruses. Alternative molecular approaches have recently been established using real-time PCR to allow discrimination among the different viral states in horses naturally infected with EHVs.13,14 Discrimination among the different viral states is now possible by 1) targeting several genes (e.g., glycoprotein, latency-associated transcripts), 2) detecting viral genomic DNA and transcriptional activity of the target genes at the messenger RNA (mRNA) level, and 3) using absolute quantification. Viral threshold loads are used in selected human infectious diseases (i.e., HIV, HCV) to determine disease stage and response to antiviral therapy. A similar concept is used diagnostically for EHV-1- or EHV-4-infected horses in order to discriminate between lytic and nonreplicating virus, to determine their infectious risk based on viral load in respiratory secretions, 1314and to monitor their response to treatment.13,14
Streptococcus equi subsp. equi infection is rarely associated with detection difficulties when using conventional cultures in clinically affected horses. Culture, however, may be unsuccessful during the incubation, and early clinical phases of infection and the presence of other β-hemolytic streptococci, especially S. equi subsp. zooepidemicus, may complicate interpretation of cultures. Available PCR assays are designed to detect the DNA sequence of various virulence genes of S. equi. PCR assays can be completed in a few hours, and results may be available on the same day that samples have been submitted to the laboratory. One of the pitfalls of PCR has been its inability to distinguish between live and nonviable organisms; therefore positive results have in the past been considered presumptive until confirmed by culture. Nowadays, the viability issue can be addressed by quantitation of S. equi virulence genes or the detection of transcriptional activity for virulence genes at the RNA level.15 In several studies, PCR proved to be up to three times more sensitive than culture.16-17 PCR accompanying culture on a nasal swab or guttural pouch lavage may be used in a control program to select possible carrier animals, because PCR is capable of detecting S. equi DNA in guttural pouch lavages for weeks after disappearance of live organisms. Such is not the case for the nasopharynx, in which the efficient mucociliary apparatus removes organisms and DNA at the same time. PCR should be considered in order to detect asymptomatic carriers, establish the S. equi infection status of asymptomatic horses, and determine the success of elimination of S. equi from the guttural pouch. A particular problem in the management of strangles outbreaks is the lack of a suitable assay to differentiate between wild-type and vaccine S. equi strains. However, recent studies have shown gene variations in the N-terminal region of the SeM gene of various field isolates, allowing epidemiologic analysis of disease transmission.18 Further, a deletion in the aroA gene of a live-attenuated strangles vaccine marketed in Europe (Equilis StrepE, Merck Animal Health, Walton Manor, Walton, Milton Keynes, UK) has allowed the development of a PCR assay able to differentiate between wild-type and vaccine strains.18 Such assay has, however, not yet been developed to differentiate between the intranasally applied attenuated live vaccine marketed in North America (Pinnacle I.N., Zoetis, Overland Park, Kan.) and field isolates. However, when needed for forensic reasons, differentiation can be done via the morphology of colonies, biochemical analysis, genotyping, and restriction digest.19 Together, these assays allow differentiating between wild-type and vaccine/ ancestor strains.
Streptococcus equi subsp. zooepidemicus (S. zooepidemicus) is a commensal, opportunistic equine pathogen that is generally present in the upper respiratory tract and responsible for secondary bacterial bronchopneumonia in young and adult horses. The literature reports on a few outbreaks of upper respiratory disease associated with S. zooepidemicus.20,21 The clinical signs are indistinguishable from S. equi infection and include lethargy, anorexia, elevated rectal temperature, serous to purulent nasal discharge, coughing, and lymphadenopathy with abscessation. Single clones of S. zooepidemicus, as determined by sequencing of the szP gene and multilocus sequence typing, have been associated with increased pathogenicity.20 From a diagnostic standpoint, one should not test for S. zooepidemicus in nasal secretions from horses with upper airway disease due to the ubiquitous nature of this bacterial organism. However, S. zooepidemicus should be considered as the etiologic agent in respiratory cases when detected by culture or qPCR from a draining lymph node or guttural pouch empyema and other respiratory pathogens have been ruled out.
Rhodococcus equi is an important cause of chronic suppurative bronchopneumonia with extensive abscessation in foals 3 weeks to 6 months of age. Culture of the organism from tracheal wash (TW) fluid currently is considered the gold standard for diagnosis.22 However, it can be difficult to reliably grow R. equi from a single TW sample, possibly because of prior antimicrobial administration or overgrowth by multiple pathogenic bacterial species.23,24 Hillidge25 reported that only 62% of foals with positive R. equi cultures at necropsy and 64% of those with radiographic evidence of lung abscessation yielded R equi on culture of TW fluid. PCR has been evaluated in order to increase the diagnostic sensitivity of TW fluid samples. Strains of R. equi isolated from sick foals uniformly contain an 85- to 90-kb plasmid that carries the gene responsible for expression of a 15- to 17-kDa antigen (vapA) of undetermined function.26,27 Environmental strains of R. equi not associated with disease do not contain this plasmid. Therefore detection of the vapA gene of R. equi in a TW fluid sample from a foal with pneumonia can be considered diagnostic. Both culture and PCR, however, may detect environmental contaminants of R. equi in TW fluid, but PCR has the ability to distinguish between virulent and avirulent strains. Foals, however, may have virulent or avirulent strains of R equi present as contaminants in their airways that are not responsible for clinical signs of pneumonia. This situation may be more likely on farms in which R. equi problems are endemic. In a study evaluating the sensitivity of conventional culture, PCR, and serology from 53 foals with pneumonia, PCR of TW fluid was found more sensitive and specific for the diagnosis of R. equi pneumonia than the other two available diagnostic tests.28 PCR should be used in conjunction with standard culture because of the probability of the presence of multiple bacterial pathogens and the inability of PCR to determine antimicrobial sensitivity of R. equi. PCR with its higher sensitivity and specificity may be useful to rule out R. equi pneumonia in culture-negative foals that have failed to improve with standard antimicrobial therapy and have clinical signs consistent with
R. equi pneumonia. It may also be useful in monitoring response to therapy and deciding when to discontinue therapy in foals that are confirmed to have R. equi pneumonia. In clinical situations in which the severity of the respiratory signs of the patient prevents the collection of TW fluid, feces have been shown to be a sensitive surrogate specimen for the molecular detection of R. equi.29,30 However, serial R. equi qPCR testing on feces should not be used as a screening test for clinical R. equi foal pneumonia.31
Equine rhinitis A and B virus and equine arteritis virus, although less commonly associated with infectious upper respiratory disease, should also be considered as target pathogens during respiratory outbreaks.32-34
EHV-2 and EHV-5 are widespread in horse populations; therefore the detection of any of these viruses can occur in healthy but also sick animals. These two viruses are optimally adapted to their host, which means that significant clinical expression of infection is rarely encountered. Recent work has shown that different genetic variants of these viruses circulate among healthy horses, hypothesizing that viral reinfections or reactivations may be the origin of clinical disease and also explaining the sporadic occurrence of such cases.35 Another characteristic of the gammaherpesviruses is their ability to immunomodulate the immune system, potentially increasing the susceptibility of horses to various infectious pathogens.36 A recently described atypical interstitial pneumonia named equine multinodular pulmonary fibrosis (EMPF) has been linked to the presence of EHV-5 in affected pulmonary tissue.37 The diagnosis of this disorder is based on clinical signs, radiographic abnormalities of the lungs, lower airway fluid cytology, histopathology of pulmonary tissue, and EHV-5 detection by qPCR in bronchoalveolar fluid and/or pulmonary tissue.37,38 Due to their high prevalence in the horse population, and in order to avoid dilemmas with the interpretation of PCR results, testing of EHV-2 and EHV-5 in horses with upper respiratory tract disease is not recommended at this time.
NEUROLOGIC PATHOGENS. Although highly sensitive and specific PCR assays have been developed for detection of viral and protozoal genomes in the cerebrospinal fluid (CSF) of neurologic patients, these methods are often of limited value in the routine diagnosis of these diseases because viremia is often short-lived or the pathogen has no affinity to the cells of the CSF. Consequently, pathogens are usually no longer detectable at the onset of systemic or central nervous system signs.
Equine protozoal myeloencephalitis (EPM), caused by the protozoal Apicomplexa parasites Sarcocystis neurona and Neospora hughesi, represents one of the greatest diagnostic challenges for equine practitioners. Detection of the parasite at necropsy is considered the gold standard. Therefore clinical diagnosis is based on clinical findings, exclusion of other neurologic diseases, and the use of serologic assays (e.g., Western immunoblot, indirect immunofluorescent assay, ELISA) on serum and CSF.39-41 Molecular diagnostics have also been investigated, but their sensitivity was found to be low.42
Apparently, intact merozoites rarely enter CSF, and free parasite DNA is destroyed rapidly by enzymatic action.43 On the basis of low sensitivity, PCR testing of CSF should not be recommended for routine diagnosis of EPM. In contrast, PCR testing of neural tissue has been shown to be useful as a postmortem test.44 Sequence analysis is routinely used to identify
S. neurona and N. hughesi isolates and to determine the heterogeneity and evolutionary relatedness within these and related species.45,46 Detection and isolation of S. neurona from peripheral blood have been reported only in experimental studies.47,48 Therefore molecular detection of S. neurona in blood is insensitive and should not be used in order to document or rule out EPM in a neurologic horse.
Diagnosis of WNV encephalitis in horses currently is based on observation of compatible clinical signs (e.g., ataxia, paresis, paralysis, hyperesthesia, muscle fasciculation, seizures, fever) and one or more of the following: isolation of WNV from blood, CSF, or tissue; a fourfold increase in plaque reduction neutralization test antibody titers on paired serum samples taken 2 weeks apart; or the detection of IgM antibody to WNV by IgM-capture ELISA.49,50 Given the nonspecificity of the IgM ELISA (i.e., does not differentiate between disease and exposure) and the time required to serologically confirm WnV infection, alternative tests able to rapidly detect WNV in clinical specimens are important. RT-PCR using a one-step, nested, or real-time approach has been evaluated to investigate antemortem cases of suspected WNV encephalitis in horses and humans using blood. The diagnostic sensitivity of WNV RT-PCR using either serum or whole blood was low.51-53 However, 57% to 70% of CSF samples from human beings with serologically confirmed WNV infection tested positive by real-time RT-PCR.51,52 The reduced ability to detect WNV in CSF or serum from patients with serologically confirmed WNV infection is likely due to the short-lived viremia in dead-end hosts, and it emphasizes the fact that, in order to detect WNV in blood or CSF, the sample should be collected early during the disease process. Investigation of the sensitivity of RT-PCR on CSF from horses with WNV encephalitis has not yet been reported. RT-PCR has also been shown to accurately identify WNV in field-collected mosquito pools, avian tissues, and human and equine brain tissue samples with a degree of sensitivity approaching that of virus isolation in Vero cells.52-54
Myeloencephalopathy is an uncommon presentation of EHV-1 infection and should always be considered as a differential diagnosis when a horse develops sudden neurologic signs (e.g., ataxia, paresis, urinary incontinence), especially if multiple horses on the premises are involved or when a recent history of fever, abortion, or viral respiratory disease in the affected horse or herdmates is reported.55 Diagnosis is often based on history, clinical signs, and xanthochromia and elevated total protein concentration in CSF resulting from vasculopathy. Attempts to isolate virus from the blood or CSF of patients are often unsuccessful because the peak of viral shedding has usually passed by the time neurologic signs appear.56 However, affected horses can shed the virus in nasal secretions and thus represent a risk of infection for unaffected in-contact horses. This outcome has been reported in a hospital setting in which horses developed neurologic disease after having been exposed to horses with EHV-1 myeloencephalopathy.57 Therefore it is imperative to determine the risk of shedding in a suspected horse in order to initiate appropriate infectious disease control protocols. PCR, as previously shown for viral respiratory diseases, is a fast and sensitive molecular diagnostic tool and should be performed on blood and nasal or nasopharyngeal swabs to document viremia and nasal shedding, respectively.58,59 The dilemma as to whether the virus is in a lytic, nonreplicating, or latent state can be addressed by using absolute quantitation or transcriptional activity of the target gene similar to the approach used for EHV-4.13 A recently identified single nucleotide polymorphism (SNP) at position 2254 in the DNA polymerase gene (ORF 30) correlates with neurologic disease.60 This SNP is responsible for a single amino acid residue at position 752 of the DNA polymerase with EHV-1 strains associated with neurologic outbreaks involving a D752 genotype (also referred to as G2254), whereas most nonneurologic outbreaks involve a N752 genotype (also referred to as A2254). Rapid qPCR assays have been established to allow differentiation between neuropathogenic and nonneuropathogenic strains.61-63 However, the genotyping of field isolates needs to be interpreted carefully as 14% to 24% of EHV-1 isolates from horses with EHM do not have this neuropathogenic marker.64 Strain characterization may be important given that the potential of EHM development is greater in horses infected with a neuropathogenic genotype (D752). Furthermore, detection of a neurotropic EHV-1 strain may influence therapy, especially in the use of antiviral drugs such as valacyclovir, used to decrease viremia and prevent the development of neurologic sequelae.
Borrelia burgdorferi, the causative agent of Lyme disease, is a helical-shaped, gram-negative, unicellular spirochete transmitted by infected Ixodes ticks. In general, the diagnosis of Lyme disease in horses is made on the basis of the geographic origin of the horse, ruling out other causes of clinical signs and a high antibody titer to B. burgdorferi.65 qPCR for B. burgdorferi in CSF has been shown to be specific, but the results are often negative due to the rare occurrence of the spirochetes in the CSF.66 However, PCR can be used to help document the presence of B. burgdorferi at postmortem on neurologic tissue or infected ticks.67
GASTROINTESTINAL PATHOGENS. The detection of equine gastrointestinal pathogens using conventional or molecular tests is often challenging because these pathogens are difficult to grow in cell culture systems or can be present in pathogenic or nonpathogenic forms, making interpretation of positive results difficult. Furthermore, the use of fecal material for molecular diagnostics has been associated with false-negative results because of the presence of inhibitory substances in the feces that can interfere with NA extraction or amplification.68 However, development and use of specific extraction kits (DNA Stool Mini Kit, QIAGEN, Valencia, CA) have improved the yield of NA from feces.69
Neorickettsia risticii is the rickettsial agent responsible for equine neorickettsiosis (EN) (formerly Potomac horse fever), a serious enterocolitis of horses. Because of the nonspecific nature of the clinical signs, a provisional diagnosis of EN is often based on the presence of typical clinical signs and the seasonal and geographic occurrence of the disease. A definitive diagnosis of EN, however, should be based on isolation or detection of N. risticii from blood or feces of infected horses.70 Isolation of the agent in cell culture, although possible, is time consuming and not routinely available in many diagnostic laboratories. The recent development of N. risticii-specific PCR assays has greatly facilitated the diagnosis of PHF.71-72 These molecular assays have contributed to the investigation of the epidemiology of PHF, allowing the discovery of helminthic vectors and intermediate and definitive helminthic hosts, as well as determining the natural route of infection.73-75 Nucleic acid of N. risticii can be detected in the blood and feces of naturally or experimentally infected horses, but the detection period does not necessarily coincide between the two sample types (Fig. 29.2). On the basis of these results, we recommend analyzing both blood and feces from suspected horses in order to enhance the chance of molecular detection of N. risticii.
Lawsonia intracellularis, an obligate intracellular bacterium, is the causative agent of proliferative enteropathy in a variety of domestic and wild animal species.76 In horses, Equine proliferative enteropathy (EPE) often affects young horses. Antemortem diagnosis can be challenging and is based on interpreting clinical signs (e.g., lethargy, anorexia, fever, weight loss, subcutaneous edema, diarrhea, colic), clinicopathologic results (e.g., hypoproteinemia resulting from hypoalbuminemia), and ultrasonographic findings (e.g., thickened small intestinal walls) and excluding other causes of similar gastrointestinal findings.77 Currently, culture of the organism is difficult and is not routinely offered by laboratories. Antemortem diagnosis relies on serology and PCR.78 The combination of both tests and repeated fecal sampling for PCR from target animals will increase the chance of diagnosing the disease. PCR has the advantage of being fast and can yield positive results in the early stage of disease, when antibodies are not yet measurable. Prior use of antimicrobials can negatively affect the molecular detection of L. intracellularis in feces. Therefore in a suspected case, fecal collection for PCR testing should be performed before the institution of any antimicrobial treatment.
In recent years, PCR assays for the detection of Salmonella spp. in fecal samples from horses admitted to veterinary hospitals have been evaluated.79-82 Collectively, these studies have shown an unquestioned higher analytic sensitivity for the detection of Salmonella spp. PCR assays when compared with conventional microbiological culture. The higher detection rate of Salmonella by PCR has been attributed to the detection of nonviable organisms and of previously undescribed Salmonella-like bacterial organisms. The use of novel virulence target genes for the molecular detection of Salmonella spp. has considerably improved the performance and accuracy of such assays. More and more veterinary hospitals across North America are switching from conventional microbiological culture to qPCR for the testing of Salmonella as part of their infectious disease control program. In such instances, qPCR is performed on fecal and environmental samples following a 24-hour selective enrichment step. The use of qPCR is cost effective and has the potential to reduce contamination risks and turnaround time, with results being available within 22 to 28 hours from sample collection (18 to 24 hours enrichment time, 4 hours for DNA purification and amplification). Further, the use of absolute quantitation allows assessment of the infectious nature of hospitalized animals and may be an excellent alternative to conventional culture methods for surveillance and research studies.83 Although qPCR for Salmonella spp. is an accurate and fast screening test, one must still consider microbiological culture to confirm positive molecular results and to determine the serovar and antibiogram of the isolated Salmonella spp.
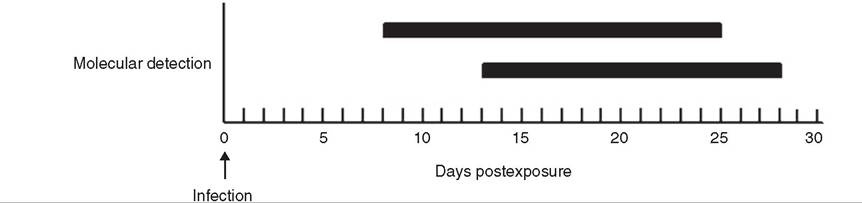
FIG. 29.2 Molecular detection period of Neorickettsia risticii in blood and feces of experimentally infected horses. (From Pusterla N, Madigan JE, Leutenegger CM: Real-time polymerase chain reaction: a novel molecular diagnostic tool for equine infectious diseases. J Vet Intern Med 20:3, 2006. Reprinted with permission of the American College of Vterinary Internal Medicine.)
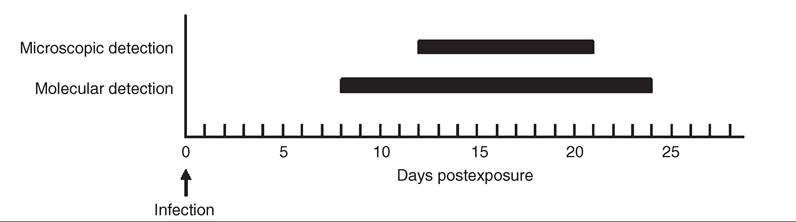
FIG. 29.3 Microscopic and molecular detection period of Anaplasma phagocytophilum in the blood of horses experimentally infected with Ixodes scapularis. (From Pusterla N, Madigan JE, Leutenegger CM: Real-time polymerase chain reaction: a novel molecular diagnostic tool for equine infectious diseases. J Vet Intern Med 20:3, 2006. Reprinted with permission of the American College of Veterinary Internal Medicine.)
The detection of equine coronavirus (ECoV) by qPCR in the feces of foals with fever and diarrhea is difficult to interpret because ECoV has also been detected in the feces of healthy foals.84 Healthy foals have been found to be infected mostly by ECoV in a single infection without any other co-infecting agents, whereas ECoV was found exclusively in association with other co-infecting agents in sick foals. This is in agreement with coronaviruses in other species, where the virus may not have enough pathogenic potential to cause disease but causes local immune suppression, allowing secondary infections to take place more efficiently. In adult horses, ECoV causes a self-limiting disease characterized by lethargy, anorexia, fever, and less frequently changes in fecal character and colic.85,86 The diagnosis of ECoV infection in adult horses should be supported by the qPCR detection of ECoV in the feces.
Equine rotavirus poses a challenge each foaling season to farm managers and veterinarians in intensive horse-breeding areas throughout the world. A quick and reliable diagnosis is essential in order to separate affected foal with diarrhea and reduce the spread of this virus. The diagnosis of rotavirus infection has in the past relied on direct virus detection using a rapid antigen-capture ELISA. Commercially available qPCR assays have shown high analytical sensitivity, specificity, and accuracy in the diagnosis of equine rotavirus infection and will likely replace the less sensitive ELISA test in the near future.87
Clostridium difficile is a fastidious anaerobe considered an important cause of colitis, although it can also be found in the intestinal tract of healthy horses.88 Although the dynamics of colonization are unknown, it is likely that horses can carry C. difficile for long periods without ever developing disease. Carrier status is generally higher in foals and adult horses treated with antimicrobials. The diagnosis of C. difficile infection is generally based on the detection of toxin A or B or both in feces, gastric reflux, or colonic content, ideally using a test that has been validated in horses.88 A variety of immunoassays are available, but only one assay has been validated in horses (Clostridium difficile TOX A/B II ELISA, Techlab, Blacksburg, Va.).89 This test, which detects toxin A and B, has a reported sensitivity of 84% and specificity of 96% compared with the gold standard (cell cytotoxicity assay). qPCR targeting the toxin A and B genes of C. difficile has been shown to be highly sensitive with the advantage of a short turnaround time.90 However, the clinical specificity will depend on the overall background prevalence of C. difficile colonization in the population of horses tested. qPCR is considered an acceptable screening tool to rule in or rule out C. difficile infection, allowing proper management and isolation of qPCR-positive patients.
Clostridium perfringens type A and C are important causes of enteric disease in young foals. Disease induced by C. per- fringens, especially type C, is associated with hemorrhagic diarrhea, abdominal distention, and circulatory shock.91 The diagnosis of C. perfringens infection is challenging because the microbe can be cultured from the feces of healthy foals. Therefore identification of toxins and ruling out other etiologies of diarrhea are key.91 For toxin assays, fresh feces should be submitted to a laboratory with immunoassays for C. perfringens toxins including alpha, beta, and epsilon toxins. Fecal assays for C. perfringens enterotoxin (CPE) are readily available but lack sensitivity because only minorities of equine isolates produce CPE.92 The alternative diagnostic avenue is to submit isolates cultured from feces for qPCR analysis. The novel pore-forming necrotizing toxin (netF) of C. perfringens type A is an important advance in understanding the virulence of this pathogen and potentially improves the diagnostic field.93
MISCELLANEOUS PATHOGENS. Equine granulocytic ana- plasmosis (EGA) is caused by Anaplasma phagocytophilum, a rickettsial pathogen transmitted by Ixodes spp. ticks. Diagnosis is often based on awareness of the geographic area for infection, typical clinical signs, abnormal laboratory findings, and identification of characteristic pathogen inclusions in the cytoplasm of neutrophils and eosinophils in a peripheral blood smear.94 qPCR has been used for many years to study several aspects of the epidemiology and pathophysiology of EGA.95 For clinical purposes, the material of choice is whole blood. PCR has been shown to be a sensitive and specific tool, supporting the diagnosis especially during the early and late stages of the disease, at times when the number of organisms is too small to be detected via microscopy (Fig. 29.3).
Corynebacterium pseudotuberculosis is a common cause of external and internal abscesses in horses from arid regions of North America.96 The epidemiology has been investigated with the help of qPCR, and flies have been identified as potential vectors.97 C. pseudotuberculosis is easy to grow on culture, and use of qPCR on clinical samples is restricted to specific situations (e.g., culture-negative aspirates or body fluids).
Additional PCR assays for Leptospira spp., Clostridium botulinum neurotoxins, Mycobacterium spp., Mycoplasma spp., Babesia caballi, Theileria equi, Cryptosporidium spp., and methicillin- resistant Staphylococcus aureus have been developed and are being used in the research setting.98-102 These assays will likely be offered in the near future for diagnostic purposes when additional epidemiologic information has been evaluated and accuracy of the tests has been validated using clinical samples from infected horses.