A nationwide seroprevalence screening for West Nile virus in the population of Bulgaria
To assess local circulation and risk for human infections with WNV, a nationwide seroprevalence study was conducted.
Serum samples were collected prospectively from persons visiting laboratories for routine prophylactic checkup in all districts of Bulgaria: Blagoevgrad (n = 64), Gabrovo (n = 63), Vidin (n = 40), Dobrich (n = 52), Plovdiv (n = 62), Targovishte (n = 42), Montana (n = 78), and 50 samples from each of the rest 21 districts.
Information on age, sex, and area of residence for each sampled person was recorded by the staff in the laboratories.Using ELISA kits (Euroimmun, Lubeck, Germany), serum samples were tested for WNV IgG antibodies. IgG-positive samples were further tested for specific IgM antibodies and for IgG avidity using the tests from the same manufacturer. Microneutralization assay (MNTA) was used to test all IgG-positive samples to exclude infection with closely related Usutu virus (USUV).
Serum samples from 1451 residents of all districts in Bulgaria, 622 male and 829 female, mean age ± standard deviation 53.2 ± 18.8 years, were tested for WNV- specific IgG antibodies.
Specific WNV IgG antibodies were detected in 22 participants tested by ELISA giving mean seroprevalence rate of 1.5%. Neutralizing antibodies were found in 6 (27.3%) of the IgG-positive samples; titer of these antibodies ranged between 1:10 and 1:100. The MNTA-positive samples originated from four districts (Figure 4). IgM antibodies were detected in two of the IgG-positive samples, and one of them was also MNTA- positive (titer 1:100) with IgG avidity index 48%. IgG avidity index for the rest of the MNTA-positive samples was between 70 and 97%. IgG avidity index of all samples ranged between 14 and 97%, mean 59%. USUV was not found in any serum samples.
The highest seroprevalence rates of WNV IgG antibodies were detected in districts of Sofia Province and Vidin—10 and 7.5%, respectively, followed by districts of Ruse and Silistra—6% each (Figure 4).
There was no significant association of WNV seroprevalence neither with gender or age [27].The first and nationwide seroprevalence survey on WNV circulation in Bulgaria found overall seroprevalence of 1.5% for WNV However, district analysis showed WNV seroprevalence up to 7.5-10%. Recent and past infections could be suspected in accordance with variability of the IgG avidity indices.
Analysis of the WNV seroprevalence rates in Bulgaria showed that they are lower than the rates in the endemic European countries (Greece, Northern Italy, and Southern France) [37, 39, 40]. Nevertheless, they showed that WNV is widespread in the country. The highest WNV seroprevalence rate was detected in Sofia Province, where the first confirmed neuroinvasive case was described in 2015 [36] and an additional case was confirmed in 2016. WNV IgM antibodies were detected in people only from this district, giving a certainty that it is a “hot spot,” and more cases from this area could be expected in the future. WNV antibodies were detected in almost all districts near the river Danube, the border of Bulgaria with Romania. WNV outbreaks in Romania in 1996-1997 and 2010 appeared in areas close to the Bulgarian border [41]. This area represents excellent conditions for mosquito reproduction. At high risk for attracting WNV infection, according to the seroprevalence data, are also people in some central districts along the big rivers Maritsa and Tundzha as well as in a southern district, close to the border with Greece. The
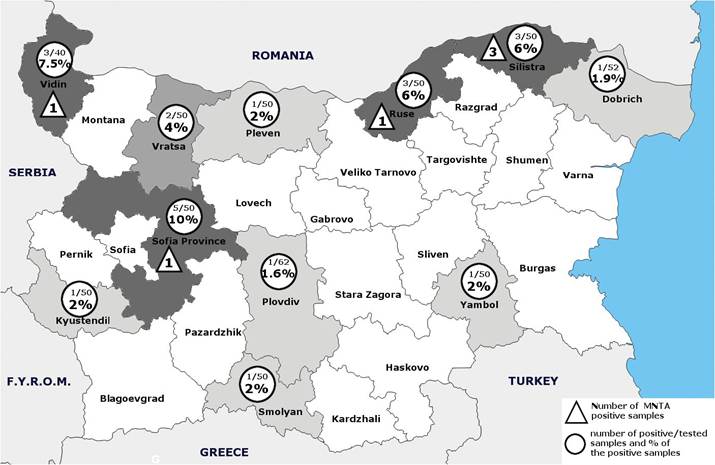
Figure 4.
WNV seroprevalence in Bulgaria, 2015.
big WNV outbreak in Greece, 2010-2012, affected northern parts of the country, not far from Bulgarian territory. The causative WNV was a recent introduction of WNV lineage 2 strain [42]. In the last years, WNV expanded and was reported also in other Balkan states.
WNF infection seems to be more widespread in the country as has been described so far. The level of WNV seroprevalence found in Bulgaria is evidence that some viral encephalitis or meningoencephalitis cases in the country are underdiagnosed and underreported.
Acknowledgements
This work has received funding from the European Unions Horizon 2020 research and innovation program under grant agreement No 732732.