Neoplastic conditions of the esophagus
Ann E. Hohenhaus
Introduction
Esophageal tumors represent less than 0.5% of all canine tumors.1 Both dogs and cats can develop esophageal tumors, which are typically malignant in both species.
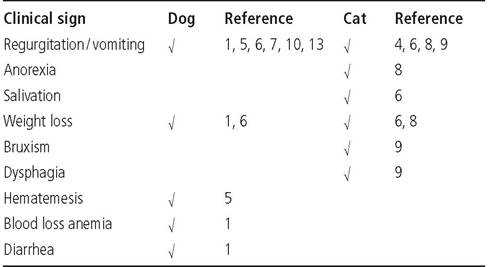
A strong causal relationship has been reported between infection by the nematode Spirocerca lupi and canine esophageal sarcoma in geographical regions where the parasite is enzootic.2,3 Other than spirocercosis, the etiology of esophageal neoplasms in dogs and cats is unknown.Table 3.1: Clinical signs attributed to esophageal neoplasia in the dog
Histopathology
Many histological types of primary esophageal tumors have been described, including squamous cell carcinoma, adenosquamous carcinoma, adenocarcinoma of the esophageal glands, neuroendocrine carcinoma, plasma cell tumor, and osteosarcoma.1-11 Benign esophageal tumors such as leiomyoma have been reported in the dog.12-13 Secondary esophageal tumors originate from locally invasive tumors such as thyroid carcinoma or gastric carcinoma, or via distant metas- tasis.1,14 In one study, tumors metastatic to the esophagus were three times more common than primary esophageal tumors (Figure 3.16).1
Clinical signs
The clinical signs of esophageal tumors in the dog and cat have been summarized in Table 3.1. Most of the clinical signs associated with esophageal neoplasia can be explained by obstruction of the esophageal lumen by tumor or because of pain during swallowing. An association has been made between chronic upper respiratory signs and papillomatous esophagitis in a cat.15 This cat was believed to have had chronic reflux into the pharynx and nasal passages resulting in the chronic upper respiratory signs.
Esophageal tumors should be suspected in cases of unexplained chronic upper respiratory signs.Diagnosis
Physical examination findings and routine blood tests are not typically contributory to the diagnosis of esophageal neoplasia unless a cervical mass is present. Diagnostic imaging is required to localize the esophageal tumor and determine the best approach for biopsy and treatment.14
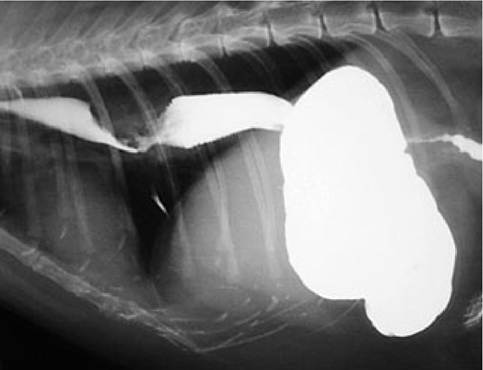
Figure 3.15:
Esophageal tumor in a cat. This contrast esophagram demonstrates a filling defect secondary to an esophageal tumor in a cat.
Plain radiographs are of limited utility in the diagnosis of esophageal neoplasia unless a soft tissue mass associated with the esophagus is seen. Thus, the value of plain radiographs is in eliminating other esophageal disorders, such as foreign bodies and megaesophagus. As a sequela of vomiting and regurgitation, air may be present in the esophagus. Also, pulmonary infiltrates consistent with aspiration pneumonia may be seen. A contrast esophagram will frequently show esophageal dilation proximal to a tumor, a filling defect in the area of the tumor, or leakage of contrast material from an esophageal defect caused by the tumor (Figure 3.15). When interpreting contrast esophagrams, it is important to remember that the
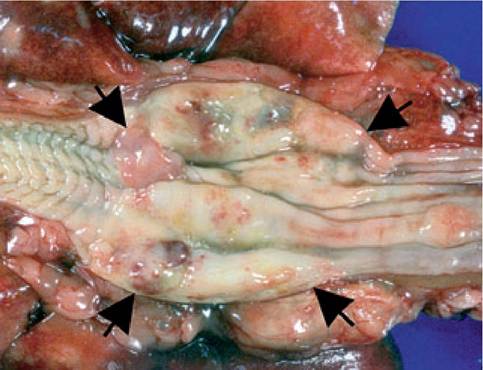
Figure 3.16:
Appearance of striated muscle in a cat esophagus. This Figure shows a metastatic renal sarcoma in the esophagus (arrows) of a cat. Note the normal striated muscle of the distal feline esophagus on the right.

Figure 3.17:
Esophageal squamous cell carcinoma in a dog. This Figure shows an endoscopic view of a squamous cell carcinoma in the esophagus of a dog.
distal portion of the feline esophagus consists of striated muscle and will normally have a regular herringbone appearance (Figure 3.16). Fluoroscopic evaluation of the esophagus is not always necessary for a diagnosis of an esophageal tumor unless an evaluation of esophageal motility is required.
Esophageal tumors are typically intraluminal. Esophagoscopy allows a biopsy to be taken from the luminal surface and is a less invasive procedure than thoracotomy (Figure 3.17). Consequently, esophagoscopy is typically the procedure of choice to obtain a sample for histopathological evaluation of an esophageal tumor. Multiple tissue samples should be obtained with the biopsy forceps to ensure adequate tissue for histological evaluation.
Treatment
Although surgical resection of esophageal tumors has been the treatment modality of choice, rarely is an esophageal tumor amenable to complete resection because the esophagus is incapable of longitudinal stretching and heals poorly under tension. Reconstruction of the esophagus has been attempted by microvascular colon transfer and also by use of a vascular skeletal muscle graft.16-17 Currently, neither procedure is being widely used.
Only single case reports of other treatment modalities, such as chemotherapy, radiation therapy, and photodynamic therapy for esophageal tumors have been reported. Except for lymphoma, chemotherapy is unlikely to be of benefit in the treatment of esophageal neoplasia. The utility of radiation therapy for the treatment of esophageal tumors is limited by the poor tolerance of normal structures in the thoracic cavity for radiation-induced side effects. Photodynamic therapy, utilizing a photosensitizing dye activated by a laser light source, was administered to a dog with esophageal squamous cell carci- noma.18 The tumor underwent a partial remission and the dog survived for 9 months before recurrent regurgitation and aspiration pneumonia resulted in euthanasia.
Supportive care
Oral alimentation is compromised by esophageal tumors and a gastrotomy tube should be placed to provide adequate nutrition and decrease the risk of aspiration pneumonia from regurgitation. Naso-esophageal or esophagotomy tubes are not appropriate in patients with esophageal tumors.
Systemic complications of esophageal neoplasia
Paraneoplastic syndromes are sequela of cancer occurring remote from the site of the primary tumor.
Hypertrophic osteopathy is a paraneoplastic syndrome of unknown cause associated with esophageal osteosarcoma and also Spirocerca lupi infection.7,19Passive congestion of the liver causing ascites and hindlimb edema has been attributed to caudal vena cava compression by an esophageal leiomyoma ofthe caudal esophagus.20Two other complications of esophageal tumors reported include tracheal invasion and aspiration pneumonia. 1,6
Survival
Typically, esophageal tumors are too advanced at the time of diagnosis to allow successful treatment. Most cases have a reported survival of less than 1 month. An exception is a single reported case of esophageal plasma cell tumor treated with surgery with a survival in excess of 18 months.5
O Key Facts
■ Esophageal tumors are rare in both dogs and cats.
■ Tumors metastatic to the esophagus are more common than primary esophageal tumors.
■ Spirocerca lupi is a known cause of esophageal tumors in dogs.
■ Clinical signs are most frequently related to esophageal obstruction.
■ Resection of the esophageal tumor is rarely possible because the tumor is advanced at the time of diagnosis, leading to short survival times.