Neoplastic conditions of the liver
7.4.4.1 Hepatocellular carcinoma and adenoma
Pathogenesis
Epithelial hepatic tumors occur usually only in old dogs (> 10 years of age), and less frequently in cats.102,103 Both adenomas and adenocarcinomas are usually solitary and can become very large.
They grow slowly and have little tendency to metastasize. These tumors are usually asymptomatic until the stomach is so severely displaced by the local mass that the dog or cat starts to vomit. Hypoglycemia occurs in about half of the cases due to the production of insulin-like growth factor by the tumor cells. This may cause episodic weakness, especially during exercise. Histologically, these tumors are well- differentiated, so it is not possible to diagnose them by cytological examination of a fine-needle aspirate as it may be difficult to distinguish them from normal liver. In some cases, however, a central necrosis of the mass occurs, which may in turn become infected and may lead to signs of sepsis.Symptoms
Patients with hepatic epithelial tumors often present with chronic vomiting and sometimes weakness or exercise intolerance. Depending on the size of the tumor, the patient may also present with abdominal distension.
A combined surgical and medical therapeutic approach is usually needed for the treatment of dogs and cats with EBDO.101 After the animal is stabilized (i.e., normalized fluid and electrolyte status, vitamin K supplementation), surgery is required to relieve the obstruction. It is usually impossible to identify the precise cause of EBDO with ultrasonography and an ex-
Diagnosis
Abdominal palpation may reveal a cranial abdominal mass. Ultrasonography will confirm the hepatic origin of the mass. The mass may have an echodensity similar or slightly less than that of normal liver. The histology of a liver biopsy is diagnostic.
Hepatic enzymes or bile acids may not be elevated. In the case of a single abscess being identified in the liver, it is important to not only puncture the center of the process for cytology and culture, but also to take histological biopsies from the periphery of the abscess, in order not to miss a potential neoplastic lesion that may have led to the abscess.Management
Surgical removal of the affected liver lobe (lobectomy) is the only definite treatment. This may be successful if the tumor is not localized near the hilus, any large vessels, or the major bile ducts. Peripherally localized carcinomas are usually well resectable. Because many hepatocellular carcinomas secrete insulin-like growth factor, it is important to monitor the blood glucose concentration before and during surgery.
Therapy
Mesenchymal tumors are usually inoperable and rapidly progressive. Survival times are usually not more than a few weeks.
7.5.5.3 Malignant lymphoma
Pathogenesis
The liver is often affected by various types of lymphoma. Infiltration of tumor cells causes hepatomegaly and, in some cases, intrahepatic cholestasis can also occur. Because hepatic damage is diffuse and widespread, hepatic lymphoma is often associated with severe liver dysfunction. Usually, the tumor cell infiltration is most severe in the portal areas and around the central veins. In very rare cases, this may cause portal hypertension, leading to the formation of ascites and portosystemic collaterals. While the liver is only one of multiple sites affected by lymphoma, it is often one of the easiest sites to sample tissue for diagnosis. Cytology is adequate for diagnosis in most cases.
7.4.4.2 Hemangiosarcoma
Hemangiosarcomas are the only common mesenchymal liver tumor. Hemangiosarcomas can originate in the liver or metastasize from the spleen to the liver. In both instances, the tumor is usually spread throughout the liver. This often causes highly elevated serum or plasma liver enzyme activities and serum bile acids concentrations.
The cholestasis may also cause jaundice. Hemangiosarcomas usually occur in middle-aged and older patients, and are much more frequent in dogs than in cats.103,104Symptoms
Mesenchymal tumors usually have a severe and rapid course, with anorexia, vomiting, weight loss, and sometimes icterus. Some patients may present for acute onset of hemorrhagic ascites due to rupture of the tumor.
Diagnosis
Patients with hemangiosarcoma may a have palpable liver mass and icterus. Serum chemistry often reveals elevated liver enzyme activities and bile acids concentrations, but this is not specific. The mass can usually be visualized by abdominal ultrasonography and a fine-needle aspirate or biopsy can be collected under ultrasound-guidance. Histology is preferable to cytology for the definitive diagnosis of this tumor.
Symptoms
The clinical signs of lymphoma are highly variable and are dependant on the other organ systems that are involved. Hepatic involvement may cause icterus, malaise, anorexia, and vomiting. Hepatomegaly and splenomegaly may cause abdominal distension.
Diagnosis
A diagnosis of hepatic lymphoma is made by cytology or histology of the liver. Blood coagulation is often abnormal. However, this does not preclude the clinician from taking a fine- needle aspirate, but an abnormal coagulation profile is a contraindication for the collection of biopsies.
Therapy
Chemotherapy may be considered, but when the liver is involved the results are less favorable than with other forms of lymphoma.
7.5.5.4 Bile duct carcinoma
Pathogenesis
A bile duct carcinoma is a tumor of the biliary epithelium and occurs infrequently.104-105 Bile duct carcinomas usually metastasize quickly throughout the liver via the lymphatics and the biliary tree. This can cause severe cholestasis and icterus.
Symptoms
Many patients with bile duct carcinoma have severe icterus, general malaise, and often vomiting. The liver is often enlarged and palpable.
Diagnosis
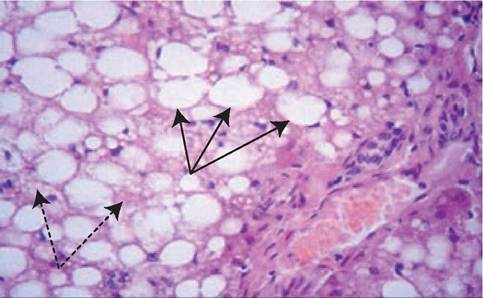
Figure 7.17:
Hepatic lipidosis - histopathology. This figure shows a histopathological image of a liver biopsy from a cat with hepatic lipidosis. The image shows both macro- (solid arrows) and microvesicular (dotted arrows) steatosis. (H&E stain, 40?).
Physical examination and laboratory evaluation indicate cholestasis. The tumor is usually detectable by ultrasonography and the diagnosis is made by ultrasound-guided biopsy. Both fine-needle aspiration and histological biopsies are diagnostic.
Management
As bile duct carcinomas spread quickly, there is no treatment and the disease is fatal.
7.5