Parenchymal liver diseases in cats
7.5.1.1 Hepatic lipidosis
Pathogenesis
Diabetes mellitus can lead to fat accumulation in the liver in all species. However, in cats, the most common form of hepatic lipidosis is idiopathic hepatic lipidosis (steatosis).
Idiopathic hepatic lipidosis used to be the most common hepatic disease of cats in North America and Europe. In the recent past, there has been a dramatic decrease in the incidence of this disease. Adipose cats seem to be predisposed, but the trigger of the disease is catabolism and cats can develop hepatic lipidosis when they consume insufficient amounts of calories or do not eat at all due to any cause. In cats with experimentally induced hepatic lipidosis, deficiency of certain essential amino acids, such as arginine and methionine, may play a role in hepatic lipid accumulation. Also, an amount of carbohydrates less than what is needed for maintenance stimulates the mobilization of fatty acids from the body fat. The fatty acids released into the blood in the periphery are then cleared by the liver and fat accumulates in the liver, causing lipidosis. The utilization of triglycerides as an energy source in different tissues depends on the presentation of fats as lipoproteins, such as VLDLs. There is some suggestion that the lipoprotein metabolism is not normal in cats that develop lipidosis.106,107 Fasting cats may not be able to supply the essential amino acids, which are required for the production of the apoprotein moiety of lipoproteins. Arginine is an essential intermediate in the urea cycle and a lack of arginine causes reduced function of the hepatic urea cycle. It is very common to find high plasma ammonia concentrations in cats with severe lipidosis of the liver. These cats often develop signs of HE and, as a result, eat even less and enter a vicious cycle, which is fatal without intervention.Many cats with hepatic lipidosis show mild to moderate hyperglycemia. This is not believed to be due to stress secondary to chronic disease, since these cats also have an impaired glucose tolerance. The exact underlying mechanism for this insulin resistance is not known. Whatever the cause, hyperglycemia is another possible factor that can further contribute to the accumulation of triglycerides in the liver. Hepatic lipidosis causes cell swelling, hepatomegaly, and intrahepatic cholestasis. Most cats with hepatic lipidosis are icteric.
Symptoms
Cats with hepatic lipidosis are usually presented with a history of anorexia, malaise, and icterus. HE may occur, with apathy, ptyalism, and ataxia.
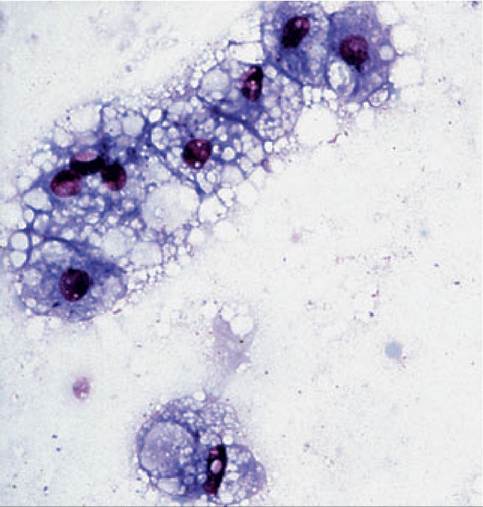
Figure 7.18:
Hepatic lipidosis - cytology. This cytological picture shows a smear from a fine- needle aspirate of the liver. There are only a few hepatocytes, most of which show a grossly distended cytoplasm with many clear vacuoles. This finding of fatty infiltration of hepatocytes in a cat is consistent with a diagnosis of hepatic lipidosis. (Diff Quick stain, magnification 150?; image courtesy of Dr. A. Rick Alleman, University of Florida, Gainesville, FL.)
Management
The most important goal of the management of feline patients with hepatic lipidosis is to get them out of their catabolic state and to supply the amino acids essential to prevent further fat accumulation and development of HE. Complete nutritional support along with treatment of known concurrent and possibly precipitating conditions are the corner stones to allow recovery.108,109 Feeding via a nasoesophageal or gastric tube is necessary if the cat is unable to be fed orally. It is essential to choose a high protein diet as cats with hepatic lipidosis cannot metabolize fat or carbohydrates efficiently. Severely affected cats are first stabilized by attending to their fluid and electrolyte needs (i.e., potassium is usually low, and hypokalemia is a risk factor for HE).
During this time, nutritional support can be provided via a nasoesophageal or nasogastric tube with a liquid enteral diet, such as CliniCare Feline Liquid Diet (Abbott Laboratories, North Chicago, IL). The use of a large bore Pezzer mushroom-tip tube (Bard urological catheter, Bard Urological Division, Covington, GA; 16 or 18 Fr; a Foley catheter should not be used) allows the use of blenderized diets (Feline p/d or k/d, Hill’s Pet Products, Topeka, KS; a mixture of one can with 11/2 cups water yields a slurry with 0.9 kcal/ml) for administration at home. Feline k/d or Veterinary Diet NF (Nestle Purina Company, St. Louis, MO) is preferred for the initial treatment of cats with HE. These diets are then gradually switched to a higher protein diet when the signs of encephalopathy have subsided. Several other diets are made to be used undiluted (i.e., feline a/d, Hill’s Pet Products, Topeka, KS [1.3 kcal/ml] and Maximum-Calorie, Eukanuba Veterinary Diets, The Iams Company, Dayton, Ohio [2.1 kcal/ ml]), making home feeding for the first 1-2 weeks even easier. It is not known whether supplementation with taurine, carnitine, or arginine hastens recovery.Diagnosis
A physical examination of cats with hepatic lipidosis usually reveals icterus and hepatomegaly. The clinicopathological findings are usually consistent with cholestasis with total bilirubin concentrations ranging up to 20 mg/dl and /or mild to moderate non-regenerative anemia. Normal to high (i.e. 3- to 5-fold increase) ALT activities and high (i.e. 10- to 15-fold increase) AP activities are usually present. There is often mild to moderate hyperglycemia and, in severe cases, hyperammonemia. Hepatomegaly can be confirmed by abdominal ultrasonography, which also often shows generalized hyperechogenicity. However, cats with hepatic lipidosis do not have any evidence of localized structural disease, such as mass lesions, or a dilated gallbladder and /or bile ducts. A diagnosis of hepatic lipidosis can only be made by the evaluation of hepatic cells (Figure 7.17).
A cytological smear of a fine-needle aspirate is diagnostic in most cases. Sudan III can be applied to unstained smears to confirm lipid vacuolation of the hepatocytes (Figure 7.18).Cats that cannot tolerate full feeding because of gastroparesis, as indicated by vomiting during feeding or repeated retrieval of a residual gastric fluid volume of more than 10 ml of food or fluid before the next feeding, may benefit from potassium supplementation if they are hypokalemic, or from the administration of a prokinetic agent such as metoclopramide (0.2 to 0.5 mg/kg SC q 6-8 h, or via feeding tube 15-20 minutes before feeding). Cisapride (0.5 mg/kg PO q 8-12 h) is a potent prokinetic agent, but can only be obtained from veterinary compounding pharmacies. Hypophosphatemia may develop during re-feeding and, if severe, can lead to hemolytic anemia. For cats with a coagulopathy, vitamin K1 (0.5 mg/kg SC q 12 h) is recommended.
Results of recent studies of experimentally induced hepatic lipidosis in cats indicate that a high-protein diet may hasten recovery. This is the only condition in which HE should be treated with a high protein diet. Also, it is not recommended to administer insulin, because this may induce severe hypoglycemia.
The dietary measures often have to be continued for a long period, which the owner can do at home. Cats that are susceptible to developing hepatic lipidosis will often develop another episode later in their life. An average of 60-70% of cats hospitalized for the treatment of hepatic lipidosis do recover. However, it is important to make the owner aware of any susceptibility so that future episodes of hepatic lipidosis can be prevented.
7.6.1.2 Acute toxic hepatopathy
Pathogenesis
Diazepam and stanozolol have been reported to be hepato- toxic in some cats.52-54 Potentially, tetracycline can also be hepatotoxic in cats, but this relationship needs to be further evaluated. While toxic effects of these drugs do occur, all three drugs have been used extensively and toxic reactions are considered to be rare.
Adverse reactions of the liver to tetracycline have been found not to be lethal, and the liver lesions observed were relatively mild.55 Diazepam toxicity is usually fatal and the liver of cats with diazepam toxicity shows massive centrilobular necrosis and exudative cholangitis. Although this seems to be a rare complication, the hepatic necrosis is so severe that one should consider alternative treatments to diazepam. Cats with stanozolol toxicity show severe centrilobular lipidosis and pronounced intrahepatic cholestasis. Stanozolol toxicity is fatal in the majority of affected cats, but most of these patients do have a pre-existent kidney dysfunction. Like dogs, cats may also have a severe dose-dependent hepatic necrosis after high doses of acetaminophen (see acute hepatitis in dogs, 7.5.1.1.1).10,48,49 All these toxic reactions are characterized by severe hepatocellular damage and these patients usually have very high serum activities of liver enzymes and are often icteric.Treatment
In cats with suspected acute hepatotoxicity, general supportive care is given. Prevention of further exposure, management of fluid and electrolyte disturbances, anti-emetic therapy, and other symptomatic and supportive measures as indicated in the individual case are required. There is no specific therapy for most hepatotoxicities. For acetaminophen intoxication: see acute hepatitis in dogs (7.5.1.1.1)
7.6.1.3 Hepatopathy due to infectious peritonitis (FIP)
Pathogenesis
Manifestations of FIP are chronic and may vary depending on the organs involved. Ascites or pleural effusion may or may not be present. The liver is often affected in patients with FIP, exhibiting a granulomatous inflammatory reaction.10,110
Diagnosis
Cats with FIP commonly have a hypergammaglobulinemia, however, so do cats with lymphocytic cholangitis.10 Hepatic granulomas due to FIP are too small to be detected by ultrasonography, but they are microscopically visible upon the evaluation of a liver biopsy.
Although these granulomas are not entirely specific for FIP, they allow a very strong suspicion of a diagnosis of FIPManagement
There is no known therapy for FIP that is efficacious.
Diagnosis
It is important to ask the owner of feline patients with acute hepatopathies for any possible exposure to known hepa- totoxins in the recent history. The liver of cats with a hepatotoxicity is usually enlarged, but this is true for most liver diseases ofcats. Serum ALT and AST activities and serum bilirubin concentration are often highly elevated. Histological examination of liver biopsies shows nonspecific changes. Therefore, the diagnosis is often based on a combination of history, disease course (acute), very high serum ALT and/or AST activities, and histopathological findings.
7.6.1.4 Hepatic changes due to hyperthyroidism
Hyperthyroidism causes fatty infiltration of hepatocytes. This fatty infiltration of the liver does not cause clinical signs of hepatic dysfunction, but in many cases the serum activities of the liver enzymes and serum concentrations of bile acids are abnormally high.5,111 The fatty changes of the liver are not severe and there is usually no hepatic enlargement. A number of symptoms associated with hyperthyroidism mimic those of primary hepatic disease: polyuria, vomiting, diarrhea, and weight loss. Hence, these clinical findings may prompt the clinician to measure serum activities of liver enzymes and serum bile acids concentrations. A subsequent liver biopsy may reveal histological changes suggestive of hyperthyroidism. In most patients, treatment of hyperthyroidism will lead to a resolution of hepatic changes.
7.6.1.5 Nonspecific reactive hepatitis and amyloidosis
See 7.5.1.6 and 7.5.2.4 for a discussion of these diseases in the dog.
7.6.2