NucleosideAnalogs
Flucytosine (5-fluorocytosine or 5-FC) is the only systemic antifungal agent belonging to the class of nucleoside analogs. It was the first agent used for the treatment of invasive mycoses in humans in 1968 (Tassel and Madoff 1968).
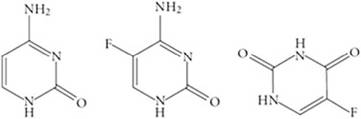
Flucytosine is the fluorinated analog of cytosine and was discovered in 1957 as an analog of the cytostatic chemotherapeutic agent 5-fluorouracil (5-FU) used for antitumor therapy (Heidelberger et al. 1957). After it penetrates the cell wall, which is controlled by the enzyme cytosine permease, 5-FC is converted to 5-FU by the cytosine deaminase and then further to 5-fluorouridine (Polak and Scholer 1975).After three phosphorylation steps, it is incorporated into RNA instead of uracil, which results in the blockade of protein synthesis. This inhibition leads to reduced DNA synthesis because of a reduction in the available nucleotide pool (Cutler et al. 1978). Therefore, fungi lacking cytosine deaminase are not susceptible to 5-FC (Polak 1977), and it is noteworthy that this enzyme is absent in mammalian cells. Figure 16.6 shows the chemical structures of cytosine and two fluorinated pyrimidines (5-fluorocytosine and 5-fluorouracil).
Flucytosine can be administered both orally and intravenously and is well distributed in almost all body fluids including the lacrimal fluid, urine, and cerebrospinal fluid (CSF) (Cutler et al. 1978). Flucytosine is well-tolerated, but at concentrations above 100 mg/L, it may induce liver and bone marrow toxicity including bone marrow suppression, myocardial toxicity, and renal failure (Benson and Nahata 1988).
5-FC is active against most clinically important yeast such as those of the Candida (Pfaller et al. 2002) and Cryptococcus genera (Pfaller et al. 2005), shows limited activity against melanized fungi and Aspergillus spp. (Verweij et al. 2008), and is ineffective against dimorphic fungi (Shadomy 1969).
The in vitro activity of 5-FC is affected by a variety of test conditions such as incubation time, test medium, medium pH, and endpoint determination criteria (34).Fig. 16.6 Chemical structures of cytosine (left), 5-fluorocytosine (middle), and 5-fluorouracil (right)
In humans, flucytosine combined with amphotericin B is primarily recommended for the treatment of cryptococcal infections of the central nervous system (Perfect et al. 2010). In addition, flucytosine in combination with an azole (fluconazole) may have a role in the treatment of disseminated Candida infections that are refractory to first-line antifungal agents (triazoles and lipid formulations of amphotericin B) (Pappas et al. 2004). Rapid resistance occurs if flucytosine is used as monotherapy (Hospenthal and Bennett 1998), and, therefore, it should never be used alone.
In cats, flucytosine in combination with amphotericin B has been used for treatment of systemic cryptococcosis, whereas this combination therapy is not recommended in dogs due to potential severe toxic reactions (Malik et al. 1996).
16.2.5