Nutritional and Metabolic Diseases
Obstructive Urolithiasis
In goats, clinical obstructive urolithiasis is most frequently seen in young, castrated males and the calculi are usually composed of phosphate salts, especially calcium phosphate (apatite) and magnesium ammonium phosphate (struvite).
Goats kept as pets are at high risk for developing the condition, due primarily to the feeding of excessive grain in the diet. The case management and treatment options of goats kept as pets may differ considerably from those for goats kept as livestock.Etiology and Pathogenesis
Obstructive urolithiasis is the inability to normally void urine because of obstruction of the urinary outflow tract by calculi. The formation of urinary calculi results from the interaction of numerous physiologic, nutritional, and management-related factors. The tendency for urinary calculi to become lodged in the urethra derives from anatomic factors and castration practices in male ruminants. Factors predisposing to urinary calculi formation in livestock have been well reviewed (Constable et al. 2017).
The urine is a highly saturated solution of mineral solutes. Under normal circumstances, these solutes usually remain in solution. However, numerous factors can predispose to precipitation of minerals from urine leading to calculi formation. These include increased urine concentration from decreased water intake or increased insensible water loss, urine stasis, increases in urine pH that favor precipitation of phosphate calculi, increased mineral concentration in the urine related to diet composition, and decreases in the concentration of protective colloids in the urine that ordinarily inhibit precipitation by transforming the urine into a stable gel.
Calculus composition frequently reflects diet. Silicate calculi are common where grass and cereal hays are the main dietary constituents, particularly in arid regions.
Forages high in oxalates promote oxalate calculi, with certain plants such as Halogeton contributing significantly to the problem. Legumes like subterranean clover and alfalfa are high in calcium and extensive grazing or hay feeding of legumes may lead to calcium carbonate stones. Grain rations, or concentrates, are commonly high in phosphorus and relatively low in calcium. This imbalance promotes the formation of phosphate calculi, as frequently seen in feedlot steers and wethers on finishing diets. The calculogenic potential of such diets is increased when the concentrate is also high in magnesium.In goats, several relationships of diet to calculus formation have been observed in the field or confirmed experimentally. Obstructive urolithiasis caused by magnesium ammonium phosphate (struvite) calculi was observed in Brazilian goats fed a concentrate ration of three parts corn to one part cottonseed meal (Unanian et al. 1982) and in Australian Angora goats fed a pelleted feedlot finishing ration with a calcium-to-phosphorus ratio of 1 : 15 (Bellenger et al. 1981). Goats fed rations containing magnesium in excess of 0.6% developed struvite crystals or calculi even when the calcium-to-phosphorus ratio was properly balanced (James and Chandran 1975; James and Mukundan 1978). Experimentally, phosphate calculi were consistently produced in goats fed a ground corn and soybean meal ration supplemented with 3.5% K2HPO4 (Sato and Omori 1977). Calcium carbonate uroliths developed in the urinary bladders of goats fed a diet of alfalfa hay and pellets with calcium-to-phosphorus ratios over 3 : 1 under experimental conditions (Jones et al. 2018).
There are additional factors in the actual formation of calculi. A nidus may be necessary for calculus formation to occur. Desquamated epithelial cells in the urinary bladder are commonly considered to function as a nidus. Factors that may contribute to increased desquamation of epithelial cells include vitamin A deficiency and infections of the urinary tract.
A role for vitamin A deficiency in obstructive urolithiasis has been specifically confirmed in goats (Schmidt 1941). Desquamated epithelium in sufficient quantity may obstruct the urethra, even without the formation of mineral calculi. Infections can alter urine pH, which may promote precipitation of mineral salts.Once calculus formation is initiated, growth occurs by the process of concretion. Increased mucoproteins in the urine serve as a matrix and favor concretion. The feeding of high-concentrate rations, particularly in pelleted form, promotes an increase in urine mucoproteins.
Obstruction is not a necessary result of calculus formation, but is predisposed by anatomic factors. Obstructive urolithiasis is rarely seen in female ruminants despite the fact that calculi can and do form. The short, straight urethra allows calculi to pass easily with the urine. In contrast, the long, convoluted course of the urethra through the sigmoid flexure of the penis, ending in the small urethral process, provides ample opportunity for even small calculi to become lodged in the male urethra. This tendency is aggravated by early castration of male ruminants that results in penile hypoplasia with attendant reduction in urethral bore size, and failure of the maturing urethral process to separate completely from its distal attachment to the preputial mucosa. The effect of castration on reduced urethral diameter has been documented in goats (Kumar et al. 1982). Exogenous estrogens either in the diet or from growth-promoting implants can also lead to reduced urethral diameter by promoting swelling of the surrounding accessory sex glands in the pelvic region.
When complete obstruction of the urethra occurs, forceful attempts to urinate produce little or no voided urine. Animals so affected soon become azotemic because of decreased renal function, secondary hydroureter, and hydronephrosis.
Unless the obstruction is relieved spontaneously or by intervention, the urinary bladder or the urethra will eventually rupture.
In the former case, abdominal distension may result as urine fills the peritoneal cavity. In the latter case, urine fills the subcutaneous space in the perineal or preputial region, depending on the site of urethral rupture. At this point, the uremic process accelerates and, without veterinary intervention, the animal ultimately dies.Epidemiology
Obstructive urolithiasis is a well-recognized, highly prevalent, and costly disease of finishing steers and sheep wethers maintained in feedlot conditions and fed high- concentrate rations. Goats are rarely managed in similar intensified finishing situations, and therefore the disease is far less prevalent in the caprine species, though growing interest in commercial goat meat production could alter this situation.
In the United States and Europe, most affected goats are young males, often castrated, and frequently maintained as pets (Craig et al. 1987; van Weeren et al. 1987a). A retrospective study of 38 cases of caprine obstructive urolithiasis seen at Tufts University in Massachusetts showed 24 affected goats to be castrated males and 14 to be intact males, with no female cases seen. The average age of affected goats was 27 months, with a range of 2 months to 12 years. Many of these goats were obese, and virtually all were on high-grain diets providing energy in excess of their metabolic needs as inactive pets. There was an increased prevalence in summer and winter, times when dehydration is more likely to occur. Phosphatic calculi (struvite and apatite) were most common and occurred in the form of either sand or sediment. Calcium carbonate calculi were less frequently identified, larger, and more likely to occur as stones. More recent case reviews from other veterinary teaching hospitals or referral centers report similar findings, with young, castrated male goats representing the most common signalment for obstructive urolithiasis, and virtually no cases involving females (Ewoldt et al. 2006; George et al.
2007). Pet goats are increasingly represented in these case populations, at least in the United States.In Texas, obstructive urolithiasis is recognized as a potential problem in young Angora males being raised for sale as replacement breeding stock. To promote growth and condition in time for sale before the breeding season, these animals are fed a pelleted ration comprising sorghum or corn, cottonseed hulls, and alfalfa. The diet is recognized as highly calculogenic and obstructive urolithiasis is avoided by appropriate adjustment of the calcium-to-phosphorus ratio and addition of salt and urinary acidifiers.
In Brazil, urolithiasis occurs sporadically in the Northeast region when goats are managed intensively and fed corn and cottonseed concentrates (Unanian and Silva 1987). In Queensland, Australia, Angora goats were reported to experience obstructive urolithiasis because of greater access to grain and formulated feedstuffs (Manning and Blaney 1986). Urolithiasis in goats occurs elsewhere in the world, but contributing factors are not always evident or reported.
Clinical Findings
In the first phase of obstruction, male goats show restlessness and anxiety. Tail twitching is an early sign. There may be excessive vocalizing and teeth grinding. Affected animals strain frequently and forcefully to urinate, often stretching their bodies out to full length with a dip to the back, followed by arching. Marked abdominal press may produce some degree of rectal prolapse. Inexperienced owners may assume that the animals are constipated and medicate goats inappropriately rather than seeking veterinary attention. Palpation of the urethra on the median raphe in the perineal region reveals distension and pulsation during straining. Drops of bloody urine and/or crystals may be seen attached to preputial hairs. Animals with partial obstruction may be able to void small intermittent streams of urine but show discomfort.
Careful examination of the urethra should be conducted to locate the site of obstruction.
Visualization of the urethral process may reveal calculi at this common site of blockage (Figure 12.7). Deep palpation of the urethra along the prepuce and perineum may indicate pain or swelling at more proximal sites of obstruction such as the sigmoid flexure.When complete obstruction goes uncorrected, rupture of the bladder or urethra usually results within 24-48 hours. Rupture relieves pressure and may produce alleviation of discomfort and anxiety, so that the animal resumes a more normal attitude, at least until the signs of uremia supervene. Inexperienced owners may interpret this as a resolution of the problem rather than a progression of the problem, and thereby delay seeking veterinary attention. If it is the urethra that ruptures, then subcutaneous filling of the preputial or perineal region becomes noticeable. In rupture of the urinary bladder, bilateral, ventral abdominal distension develops, but progresses more slowly and may
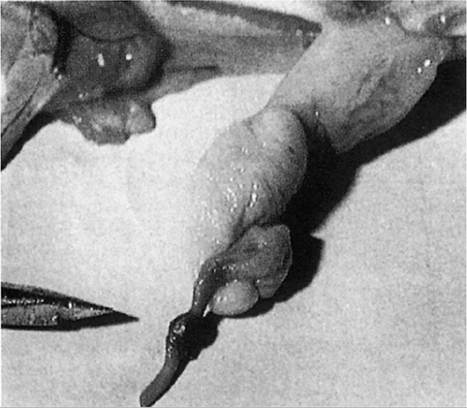
Figure 12.7 A common site of urethral obstruction with calculi is at the urethral process. The lesion pictured is highly unusual, in that the obstruction at the urethral process is a lead shotgun pellet rather than mineral calculi as is usually the case. Source: Blackwell and Dale 1983 / Veterinary Medicine and Small Animal Clinician.
be more difficult to detect, especially in obese goats or Pygmy goats that already have a distended appearance of the abdomen. Ultrasound examination will reveal an enlarged bladder or free fluid in the abdomen from a ruptured bladder, which may have sealed and be full again.
Ensuing uremia causes affected goats to become anorexic, weak, and depressed. Advanced cases often present in a moribund state and the condition is fatal if left untreated. The entire clinical course is usually two to five days.
Clinical Pathology, Radiology, and Necropsy
The most consistently reported abnormality of clinical chemistry in goats with obstructive urolithiasis is azotemia. This is reflected in the chemistry profile as high levels of BUN and serum creatinine. These levels may climb even higher if rupture of the bladder or urethra occurs. Levels of BUN in affected goats have been reported in the range of 11.7-47.5 mmol/L (70-285 mg/dL) (van Weeren et al. 1987b). A summary of biochemical abnormalities in 107 goats with uroliths has been reported (George et al. 2007). Compared to control goats, goats with urolithiasis had higher mean BUN, creatinine, total CO2, glucose, and potassium concentrations, and lower phosphorus concentrations. Hypochloremic metabolic alkalosis was the most common acid-base disorder. Rupture of the bladder or urethra was associated with an increased prevalence of hyperkalemia and hyponatremia. Hypophosphatemia was an unexpected finding in this series of cases, because among the domestic species, except horses, hyperphosphatemia is usually associated with postrenal obstruction or ruptured bladder.
Urine sediment should be examined whenever a urine sample can be obtained. Marked crystalluria supports the diagnosis of obstructive urolithiasis. Aspiration of subcutaneous or peritoneal fluid can be helpful, though confirming that the fluid is urine can be problematic. It has been reported that urine can accumulate in the abdomen, even in the absence of bladder rupture, presumably due to passage of urine through an intact but compromised bladder wall under intense pressure (Ewoldt et al. 2006). Some obstructed goats develop hydronephrosis or leak urine around the kidney. A urea nitrogen or creatinine level equal to or greater than that of blood suggests that the abdominal fluid is urine. An odor of urine may be helpful in field diagnosis.
Plain radiographs only rarely reveal cystic or urethral calculi and their use in cases of obstructive urolithiasis is not considered to be cost-effective, whereas contrast studies can be very effective both as diagnostic aids and in case management. In one retrospective study involving 21 goats with urolithiasis, the most useful imaging technique was

Figure 12.8 Necrosis, inflammation, and hemorrhage of the penile urethra at the site of an obstructive calculi in a young wether viewed at necropsy. Source: Courtesy of the Cummings School of Veterinary Medicine at Tufts University.
normograde contrast cystourethrography, performed through a tube cystostomy catheter placed as part of the surgical treatment for the cases involved (Palmer et al. 1998). Plain radiographs and excretory urethrography offered little diagnostic assistance in those cases. Ultrasonography can provide a rapid, non-invasive, and safe means of assessing the extent and location of calculi.
At necropsy, careful dissection of the urinary tract reveals the presence of calculi, urethral trauma (Figure 12.8), and bladder or urethral rupture. Calculi may be present in the bladder or renal pelvis as an incidental finding in goats dying of causes other than obstructive urolithiasis, and their presence suggests the need for reviewing nutritional management in the source herd. Calculi obtained during case management or at necropsy should be submitted for chemical analysis. In the United States, this can be done free of charge through the Minnesota Urolith Center (https://urolithcenter.org). Note that calcium carbonate stones, which are smooth, gold- to copper-colored spheres of various sizes, can be confidently identified by appearance alone (Figure 12.9).
Diagnosis
Diagnosis is based on the characteristic signalment, history, and clinical signs of obstructive urolithiasis. During the early stages, when straining is present, gastrointestinal obstructions should be considered. When stranguria is recognized, cystitis and ulcerative posthitis must be ruled out. When the bladder or urethra has ruptured and signs of uremia predominate, other causes of profound depression and weakness must be considered, especially hepatoencepha- lopathy and enterotoxemia. Confirmation of the presence of urine in the abdomen or subcutaneously quickly narrows the diagnosis.

Figure 12.9 Characteristic calcium carbonate calculi obtained from a Boer goat with urolithiasis. Source: Courtesy of Dr.M.C. Smith.
Treatment
The approach to treatment depends on the stage of the disease, the nature and extent of calculi present, the intended long-term use of the animal, and frequently financial constraints. When conservative treatment does not alleviate the condition and surgical intervention becomes necessary, a guarded prognosis should be given for successful longterm outcome. This is particularly true for intact breeding bucks and goats maintained as pets.
Medical Management
If cases are seen before rupture of the bladder or urethra occurs, conservative management can be attempted. If calculi are lodged in the urethral process, the process can be amputated to reestablish patency. When sandy material or sludge is present in the urethral process, it sometimes can be successfully milked out without removing the process itself. Such efforts require exteriorization of the penis from the sheath. This can be facilitated by the cooperation of a capable assistant, as described earlier in the chapter for examination of the penis, and by tranquilization of the animal, using diazepam, at a dose range of 0.1-0.5 mg/kg intravenously, or acepromazine at 0.05-0.1 mg/kg intravenously. Alternatively, for better analgesia and relaxation of the retractor penis muscle, lumbosacral epidural anesthesia can be employed, using 2% lidocaine at a dose of 0.1-0.2 mL/kg bw administered into the epidural space at the lumbosacral junction. The maximum dose of lidocaine should not exceed 15 mL (Van Metre et al. 1996a).
Amputation of the urethral process should be viewed as a short-term, temporary solution or as a salvage operation, because the likelihood of recurrence of obstructive urolithiasis is high after removal of the urethral process. This is exemplified in one retrospective study from North Carolina, where, in 14 of 16 cases (87.5%), urethral process amputation with medical therapy either did not relieve the obstruction or provided relief of less than 36 hours (Haven et al. 1993).
If calculi are lodged proximal to the urethral process, attempts can be made to pass a catheter far enough into the urethra to permit infusions of sterile saline in attempts to distend the urethra and dislodge the offending calculi (urohydropulsion). This procedure is frequently unsuccessful and often traumatic, and may result in urethral rupture or stricture, especially if attempts to force the catheter past the urethral diverticulum are made. The use of urethroscopy in association with laser lithotripsy has been reported to fracture and clear calculi from the distal urethra in three goats for which urohydropulsion was not successful (Halland et al. 2002).
Tranquilizers and anti-spasmodics may help to promote urethral relaxation and facilitate natural expulsion of the calculus by the pressure of attempted urination. Diazepam (0.1-0.5 mg/kg intravenously), acepromazine (0.1 mg/kg intravenously), or aminopromazine (2 mg/kg intramuscularly) have all been used for this purpose, with variable results. Xylazine hydrochloride should not be used in these cases because its hyperglycemic effect promotes diuresis, and increases in urine production are problematic in a goat with urinary tract obstruction.
Surgical Management
When conservative treatment fails, then some sort of surgical intervention, or euthanasia, becomes necessary. Detailed descriptions of the surgical procedures discussed here are beyond the scope of this book and are available in current veterinary surgery texts (Hendrickson and Baird 2013; Tibary et al. 2017). The surgical procedures include perineal urethrostomy, modified proximal perineal urethrostomy, penile amputation, ischial urethrostomy, ischial urethrotomy, surgical tube cystostomy, and marsupialization of the bladder. Prepubic urethrostomy, used in feline practice as a salvage technique for obstructive disease of the pelvic urethra, is also sometimes used in goats with favorable results, but is not discussed further here (Stone et al. 1997). A novel technique, vesiculopreputial anastomosis, was applied to four male castrated goats that already had previous surgical interventions for obstructive urolithiasis that recurred. Three of the four goats were alive 12 months post surgery (Cypher et al. 2017).
Before any surgery is attempted, particularly if general anesthesia will be involved, the patient should be evaluated for hydration status, uremia, and electrolyte imbalances, and these should be addressed through appropriate fluid therapy. Because goats with obstructive urolithiasis tend to be hyperkalemic, hypochloremic, and hyponatremic, sterile physiologic saline solution is a good empirical choice of intravenous fluid if laboratory assessment is not available (Van Metre et al. 1996a). With regard to evaluating the suitability of cases for surgery and the associated prognosis, it has been reported that an intact urethral process, the absence of fluid in the abdomen, and serum potassium concentrations less than 5.2 mEq/L at admission were all associated with greater survival following surgical tube cystostomy (Ewoldt et al. 2006).
Bladder rupture in and of itself does not necessarily require surgery. If urine outflow can be established by conservative means, the bladder defect, which often seals with fibrin or by adhesions, may heal spontaneously. This is more true of rents in the dorsal bladder wall than in the ventral wall.
If the bladder has ruptured, urine should be drained from the abdomen via abdominocentesis to slow the uremic process if surgery is delayed. This should not be accomplished too abruptly, because it could predispose to hypovolemic shock when blood that was displaced by the fluid pressure of uroperitoneum returns to the visceral vasculature from the general circulation. If the urethra has ruptured, multiple, small stab incisions can be made in the skin over the areas of urine accumulation to allow drainage.
When the decision is made that surgery is required for satisfactory case management, then the surgical approach selected depends to a great extent on the intended use of the animal and the estimated overall cost of the surgery, hospitalization, and aftercare. Clear and careful client communication is critical in these cases, because uncomplicated, fully satisfactory recoveries cannot be guaranteed and misunderstandings or false expectations about the ultimate outcome can lead to poor veterinarian-client relations, especially when pet goats or breeding bucks are involved.
For commercial wethers or intact males destined for slaughter, two relatively simple and low-cost salvage procedures are commonly in use: perineal urethrostomy and penile amputation. When performing perineal urethrostomy, a site as low on the perineum as possible should be selected for the incision for two reasons. First, it reduces the extent of subsequent urine scald. Second, the procedure is prone to failure due to stricture of the surgically created urethral opening. If that occurs, the surgery can be repeated at a site higher on the perineum to extend the salvage period for the animal. Additional salvage procedures that have been used in goats or sheep include ischial urethrostomy and ischial urethrotomy. Ischial urethrostomy offers an advantage over perineal urethrostomy in that the pelvic urethra is exteriorized instead of the penile urethra. The wider bore of the pelvic urethra reduces the likelihood of stricture at the stoma site.
For breeding bucks, surgical tube cystostomy has emerged as the preferred surgical approach for retaining breeding capacity (Van Metre and Fubini 2006). In this procedure, a paramedian abdominal approach is made and the bladder exteriorized so that a cystostomy can be performed to remove calculi from the bladder, and to place an indwelling balloon type (Foley) catheter that is exteriorized through a second stab incision and sutured in place (Figure 12.10). Ruptures of the bladder can also be repaired during this procedure if required. Antibiotic treatment should be initiated prior to surgery and continued for one week after the cystostomy catheter is finally removed, because cystitis is a potential complication of this procedure.
In a report on the outcomes of 50 goats and 13 sheep treated for obstructive urolithiasis with surgical tube cystostomy, 48 of 63 cases (76%) were discharged from the hospital with normal urethral urination. At six-month follow-up, 34 cases could be located and 21 (65%) of these had no recurrence of urethral obstruction. While some animals were lost to long-term follow-up, at 12 months up to 72 months after discharge, 18 of 20 animals (90%) identified as still alive had no recurrence of urethral obstruction (Ewoldt et al. 2006).
Early reports of surgical tube cystostomy often included antegrade flushing of the urethra as part of the surgical procedure, but flushing has come to be seen as potentially traumatic, contributing to prolonged surgical time and unnecessary. In the report of Ewoldt et al. (2006), calculi present in the bladder were removed, but no urethral flushing was done. Reestablishment of urethral patency was allowed to occur spontaneously after surgery.

Figure 12.10 View of the abdomen of a goat following surgical tube cystostomy for treatment of obstructive urolithiasis. Note the Foley catheter secured to the skin distal to its emergence from the urinary bladder through a paramedian stab incision. The primary cystostomy incision is lateral to the prepuce. Source: Courtesy of Dr. Peter Rakestraw.
In such cases, the indwelling catheter is left open after surgery to allow urine outflow. Then, beginning on the fourth day after surgery, the catheter is periodically occluded to determine if the animal is able to pass urine through the urethra. If the animal continues to display stranguria or failure to urinate, then the catheter is reopened to allow urine outflow and occluded again periodically until the patient can urinate freely. Once that occurs, the catheter is left in place for an additional three days and then removed, allowing the cystostomy site to heal on its own. Rakestraw et al. (1995) reported that the mean time until animals could urinate freely following surgery was 11.5 days, with a mean time of 14.5 days until the cystostomy tube was removed. The principle behind this approach is that diversion of urine outflow through the catheter avoids repeated trauma to the urethra caused by straining, and thereby allows the urethra to relax and heal, with a strong likelihood that calculi present in the distal urethra will ultimately dissolve or dislodge spontaneously. Calcium carbonate stones will not dissolve and need to be surgically removed from the urethra. Even in cases where the urethra has ruptured, tube cystostomy with proper postsurgical management can allow for restoration of a patent urethra and normal urine flow (Pearce et al. 2003).
A successful outcome is not guaranteed in all cases managed with tube cystostomy. Obstruction of the catheter itself with clotted blood, calculi, or sludge can occur. Therefore, it is suggested that larger-bore catheters, 18-24 or larger French, be used (Van Metre and Fubini 2006). In addition, catheters have been reported to malfunction, with the balloon not retaining its inflation. This has been associated with catheters that have been reused after autoclaving and it is therefore recommended that for tube cystostomy, only new catheters be used. Animals may also chew on catheters and dislodge or damage them, so application of Elizabethan restraint collars is indicated postsurgically.
Even when the animal recovers successfully from the procedure, maintenance of reproduction in breeding bucks is not assured, as evidenced by the reported case of erection failure associated with vascular occlusion of the corpus cavernosum penis in a goat three months after surgical tube cystostomy. The vascular lesion was believed to be associated with trauma from the inciting urethral obstruction and not the surgical procedure (Todhunter et al. 1996). Nevertheless, the ultimate goal of retaining breeding function was not realized.
Anti-inflammatory drugs post surgically should be used to facilitate urethral healing. Flunixin meglumine at a dose of 1.1 mg/kg bw twice a day (BID) intravenously for three to five days and then 0.5 mg/kg once a day (SID) intramuscularly for an additional three to five days has been reported. Acepromazine can be given to promote relaxation of the urethra postsurgically. A low dose of 0.02 mg/kg bw given subcutaneously two or three times a day has been used (Ewoldt et al. 2006).
Efforts to dissolve existing calculi have also been employed to improve outcomes, with or without surgery. In one case, irrigation of the bladder through the cystostomy catheter with the chemolytic solution hemiacidrin was reported for dissolution of calculi (Streeter et al. 2002). Hemiacidrin is an acidic solution of citric acid, magnesium carbonate, and glucono-delta-lactone, used effectively for dissolution of calcium phosphate and magnesium ammonium phosphate uroliths in human medicine (Gonzalez et al. 2012), and is marketed in the United States under the name Renacidin (Guardian Laboratories, Hauppauge, NY, USA). In the case of the goat, 30 mL of hemiacidrin was infused into the bladder via the cystostomy catheter and then the catheter was occluded for 30 minutes, after which the infusion was allowed to drain out. This was repeated four times a day for three days and appeared to be effective in dissolving existing calculi based on ultrasound evaluation. The use of Renacidin is now recommended in goats postoperatively to help acidify the urine and dissolve stones, particularly struvite stones (Tibary et al. 2017).
In another study, percutaneous infusion of Walpole's solution into the urinary bladder via ultrasound-guided cystocentesis was conducted in a series of 25 goats with obstructive urolithiasis in order to acidify the bladder environment and dissolve the calculi present. Walpole's solution is composed of sodium acetate (1.16%), glacial acetic acid (1.09%), and distilled water (97.75%), and has a pH of 4.5. It is marketed as a treatment for cats with struvite urethral obstruction and labeled for urethral catheter infusion. The amount of Walpole's solution required to achieve the target urine pH of 4-5 ranged from 50 to 250 mL. In 20 (80%) goats, the urethral obstruction resolved and the goat was discharged, though obstruction recurred in 6 of those goats. Thus, the technique offers a possible successful alternative to more costly surgical interventions (Janke et al. 2009).
One drop of glacial acetic acid in 500 mL of non-buffered sterile saline produces a solution in the desired pH range of 4.5-5.5, 60-150 mL of which can be infused and left for one to two hours before draining (Van Metre et al. 1996b). The pH should be checked before use.
Cystostomy combined with antegrade and retrograde flushing of the urethra but without tube placement was also reported to offer good results (Haven et al. 1993), although the procedure has some disadvantages, including the risk of urethral rupture during flushing, the need for an assistant to accomplish retrograde urethral flushing, and a potentially prolonged surgical time, since it can sometimes take two to three hours of repetitive flushing to fully clear the urethra of obstruction (Van Metre et al. 1996b). The technique has largely been displaced by surgical tube cystostomy. Tube cystostomy performed concurrently with urethrostomy for removal of obstructing calculi has also been reported in intact and castrated male goats, with favorable outcomes. It was noted that that calculus removal by urethrostomy may be particularly useful when calcium carbonate calculi are involved, as these calculi are not subject to dissolution by acidification techniques (Applegate et al. 2020).
Ultrasound-guided percutaneous tube cystostomy has been assessed as a surgical treatment option and found to be unsatisfactory. In a series of ten cases, all required a second surgery, five because of tube displacement from the bladder, four because of persistent or recurrent obstructive urolithiasis, and one because of subsequent urethral rupture (Fortier et al. 2004). While surgical tube cystostomy takes longer and is more costly than percutaneous tube cystostomy, the long-term outcome is much better.
Another alternative surgical procedure for breeding animals is urethrotomy in those cases in which a discrete single stone can be located by palpation or imaging studies and can be accessed and removed via an incision through the urethra. Success depends in large part on the accuracy of determining that only a single calculus is involved. Urethral stricture at the surgery site is a serious potential complication.
For pet goats, surgical tube cystostomy and marsupialization of the bladder are considered satisfactory surgical approaches. The former is likely to produce a more desirable outcome, but the latter is cheaper, a consideration for many owners. In one study of surgically managed obstructive urolithiasis cases, goats with bladder marsupialization had a median duration of hospitalization less than one- fourth the duration of goats with surgical tube cystostomy and at two-thirds the cost (Fortier et al. 2004). The main objection to marsupialization is that the permanent stoma on the ventral abdomen is associated with chronic urine scald, which requires regular attention by the owner, including clipping the hair around the site, washing, and applying petroleum jelly or other salves. Surgical placement of the stoma as far forward on the ventral abdomen as is possible without causing undue tension or strain on the bladder itself helps to obviate this problem.
Other complications of marsupialization may include prolapse of the urinary bladder mucosa, stricture of the stoma, and possibly cystitis. In one report of 19 cases of obstructive urolithiasis corrected by bladder marsupialization, 18 of 19 goats survived the procedure. At follow-up between 1 and 59 months after surgery, one animal had developed cystitis and one had a closure of the stoma due to fibrosis. While all the surviving goats had urine scald associated with the stoma site, 15 of 17 owners were satisfied with the procedure and its outcome. The two dissatisfied owners cited odor and urine scald as their objections (May et al. 1998). In that study, the median hospitalization time associated with the procedure was 4 days (range 1-10 days), compared to a mean hospitalization time of 14 ± 10 days in a report on a case series of 63 small ruminants treated by tube cystostomy (Ewoldt et al. 2006).
Before the techniques of surgical tube cystostomy and bladder marsupialization were refined and successfully applied in goats, perineal urethrostomy was often the intervention used for managing obstructive urolithiasis in pet goats. However, with the advent of these improved procedures, perineal urethrostomy should not be recommended for goats kept as pets due to the likelihood of recurrence, associated expense of additional corrective procedures, and owner dissatisfaction.
If owners insist on this salvage procedure for financial reasons, it should be made clear that long-term prospects for return to normalcy are poor, because strictures of the urethra at the urethrostomy site are common. In a study from the Netherlands on perineal urethrostomy in 28 goats and sheep, 10 died or were euthanized in the immediate postsurgical period. Of the 18 that left the hospital, only 8 had no additional problems on extended follow-up. Most of the others reobstructed and were destroyed or required second or even third operations (van Weeren et al. 1987a). Even when patency is maintained after urethrostomy, persistent problems with urine scalding on the perineum and hindlimbs often make the outcome undesirable to owners.
A modified proximal perineal urethrostomy technique has been described for non-breeding goats that is less likely than the standard perineal urethrostomy technique to result in urethral stricture postoperatively (Tobias and van Amstell 2013). The technique includes transection of the retractor penis muscles and other penile attachments to the ischium of the pelvis, to improve mobilization of the penile body and reduce tension on the perineal urethrostomy site.
Regardless of the type of surgical management selected, certain considerations of postsurgical management apply. Animals need to be monitored for abnormalities associated with uremia and treated with appropriate fluid and electrolytes as needed. Antibiotic therapy is indicated to prevent cystitis or ascending infection. Procaine penicillin G at 22 000 IU/kg intramuscularly BID, or ampicillin at 15 mg/ kg subcutaneously three times a day (TID), has been used effectively. In the case of surgical tube cystostomy, continuation of antibiotic therapy for one week after removal of the tube is recommended.
In bladder marsupialization, antibiotics should be given for a week post surgery. While there may be an inclination to keep the animals on antibiotics for prolonged periods because the bladder is open to contamination through the stoma, this is not recommended. One reason is that the occurrence of cystitis is facilitated by urine stasis and there is no stasis when the urine can passage continuously from the bladder stoma. Second, prolonged antibiotic use may promote selection of highly resistant bacteria, so that if cystitis does occur, treatment options will be limited. As such, infections that occur in marsupialized animals should be treated as they occur, preferably with antibiotic selection guided by culture and sensitivity. Marsupialized animals should be housed in clean, dry quarters when returned home.
Whenever possible, calculi removed at time of surgery or by conservative treatment should be submitted to a suitable laboratory for structural analysis, if not readily recognizable as calcium carbonate calculi based on their appearance (Figure 12.9). This permits appropriate dietary and management recommendations to be made for preventing new calculi on the basis of their composition. If the underlying management and nutritional factors leading to calculus formation are not addressed, obstructions may recur and longterm survival after surgery will be diminished.
Control
Prevention of obstructive urolithiasis depends primarily on inhibiting the formation of calculi through ion aggregation in the urine. There are three main points of control to achieve this goal: increasing urine output, acidifying the urine, and reducing the presence of calculogenic solutes in the urine. Each will be discussed separately, but in practice they are combined to successfully control the disease.
Increasing Urine Output
The solutes in concentrated urine are more likely to precipitate and form uroliths than are the solutes in dilute urine, so efforts to increase water intake and promote diuresis are critically important. Access to a clean, reliable, and adequate water supply must be assured. Goats can be particularly finicky about drinking water that is contaminated with feces, feed, or other foreign materials, so care in placement and cleanliness of waterers is important. Goats are also very hierarchical and dominant animals may keep others away from waterers, so adequate space at the water source is also a consideration. Heating water supplies in the winter and shading them in the summer may also promote consumption. For pet goats, owners may try adding flavored, sugared drink powders to encourage water consumption.
A key intervention to stimulate water consumption and to dilute the urine is the feeding of increased salt in the ration. Sodium chloride should be fed at a rate of 3-5% of the total dry matter intake, which can be estimated at about 2% of bodyweight, so that a 40-kg wether would eat about 0.8 kg dry matter and require between 24 and 40 g of sodium chloride per day. Goats may be unwilling to consume this level of salt reliably if offered free choice or in a lick, so if necessary it should be incorporated directly into the ration. One approach is to put the salt into solution and spray it onto the hay.
Acidify Urine
Ruminant urine is normally alkaline and the alkaline pH favors the formation of calculi. Acidification of urine can increase the solubility of uroliths composed of magnesium ammonium phosphate (struvite) or calcium phosphate (apatite), and thereby inhibit their precipitation from the urine. There is also evidence in sheep that silicate urolith formation can be suppressed by urinary acidification (Stewart et al. 1991). Addition of anionic salts such as ammonium chloride to the ration can be helpful in this regard (Stratton-Phelps and House 2004). The daily dose can be calculated as either 0.5-1% of the total dry matter intake, 2% of the concentrate ration, or 200-300 mg/kg/ bw/day. Ammonium sulfate has been used in place of ammonium chloride at a rate of 0.6-0.7% of the total ration. However, feeding of ammonium sulfate has been associated with cases of polioencephalomalacia in lambs (Jeffrey et al. 1994). Ammonium chloride is not very palatable to goats, so free-choice feeding is not likely to be successful. It may be necessary to add the ammonium chloride to some concentrate feed to encourage consumption, remembering that concentrate feed itself is calculogenic and should be limited in the diet. Alternately, for individual animals it can be mixed with a sugar solution, honey, or syrup, and administered as a drench.
Urinary acidifiers are not a panacea. Under e:ratio of only 1 : 1 that may require supplementation of calcium to kids. In addition, increased magnesium content of 0.6% in milk replacer was identified as contributory to the formation of calcium apatite calculi in calves, while a magnesium content of 0.1% produced no abnormalities (Petersson et al. 1988). The calculogenic effect of high magnesium content in the ration is exacerbated by high phosphorus content, but countered by high calcium content (Kallfelz et al. 1987).
The occurrence of calcium carbonate uroliths is associated with the feeding of alfalfa or other legume hays, which are high in calcium content, or the grazing of clover pastures. Mature breeding bucks, wethers, and pet goats - the main candidates for urolithiasis - are unlikely to require calcium in their diets at the level provided by legume hays. Instead, they should be fed a high-quality grass hay.
Silica calculi are seen most often in extensively grazed ruminants where the range grasses contain high silicate content. Therefore, dietary management options are limited. Ensuring adequate access to water and supplemental feeding of salt may be helpful.
Some other control interventions merit consideration. Feeding animals frequently or on an ad libitum basis rather than only once or twice per day may be helpful. Large meals can draw extracellular fluid into the rumen, resulting in transient increases in urine concentration that can promote calculus formation. This effect is less pronounced with smaller, more frequent feedings. Ensuring adequate vitamin A in the diet is also advised.
Delaying castration may be another management tool for reducing the prevalence of obstructive urolithiasis. However, the early precocity of goats requires that castration be performed by 3 months of age to avoid unwanted sexual activity, unless assured separation of males from females can be achieved past that age.
Oxalate Toxicosis
Like other ruminants, goats are susceptible to oxalate toxicosis from consumption of oxalate-containing plants or chemical compounds such as ethylene glycol that produce oxalates as metabolites. However, reports of naturally occurring disease in goats are uncommon compared with sheep (Kimberling 1988).
Etiology and Epidemiology
Oxalate toxicosis results from consuming large quantities of plants containing increased levels of sodium or potassium oxalate. Plants in the genus Rumex, such as sorrel and dock, and the family Chenopodiaceae are well known as oxalate accumulators. The most commonly involved species are Halogeton glomeratus (halogeton) and Sarcobatus vermiculatus (greasewood), found in the semiarid grazing areas of the western United States, and Oxalis spp. (sour- sob) in Australia. Numerous other plants are also recognized as containing soluble oxalates, but are less frequently involved in poisoning of livestock (Osweiler et al. 1985).
In goats, clinical oxalate toxicosis has been diagnosed after consumption of Amaranthus spp. (pigweed) in Mexico (Gonzalez 1983). In Australia, goats died after grazing almost exclusively P. clandestinum, or Kikuyu grass. Though it was not the primary lesion, the affected goats had nephrosis with tubular casts containing calcium oxalate crystals (Peet et al. 1990). Goats maintained as pets or on hobby farms may be at increased risk if they are fed certain garden cuttings. Rhubarb and spinach ingestion have been associated with oxalate toxicosis of goats in Australia (Baxendell 1988).
In addition, oxalates may be found in some manmade chemical products or be derived from other products by metabolism in the body. Ethylene glycol poisoning, likely resulting from automotive antifreeze ingestion, has been reported in goats (Boermans et al. 1988). Excessive administration of ascorbic acid, a metabolic precursor of oxalate, was believed to be responsible for a case of oxalate nephro- toxicosis in a 10-year-old Toggenburg doe (Adair and Adams 1990). The goat received 108 g of ascorbic acid over a six-day period before the onset of azotemia.
Pathogenesis
When small quantities of oxalates are consumed by ruminants, most of the oxalates are either destroyed in the rumen or combined with free calcium and excreted in the feces. A small quantity may be directly absorbed into the blood. When large quantities are consumed, the amount of oxalate absorbed increases. When in the blood, oxalates combine with calcium ions to form calcium oxalate. This causes a decrease of serum calcium levels, sometimes as much as 50%, and leads to a clinical syndrome of neuromuscular dysfunction similar to that seen in milk fever in cattle. Because calcium oxalate is insoluble, crystal formation ensues, with crystals accumulating both in the systemic vasculature and in the renal tubules. Renal tubular damage can cause severe renal insufficiency.
Ethylene glycol, the active ingredient in engine antifreeze products, is less toxic to ruminants than monogas- trics or preruminants, because much of it is degraded by rumen microflora after ingestion. However, when sufficient quantities are consumed, absorption and subsequent metabolism to toxic intermediates such as oxalic acid can occur. Unmetabolized ethylene glycol can act directly on the central nervous system as a depressant. Pathophysiologic changes induced by ethylene glycol toxicosis include hypocalcemia, increased serum osmolarity, acidosis, renal tubular dysfunction, and uremia, though death is not necessarily related to the degree of uremia.
Clinical Findings
Oxalate toxicosis is an acute poisoning with clinical signs developing within several hours of ingestion of offending plants. Affected goats exhibit incoordination, muscular trembling, hyperexcitability, and restlessness, followed by weakness, recumbency, and torticollis. Coma ensues and death often occurs within hours of the onset of clinical signs.
In the one reported case of ethylene glycol toxicosis in a goat (Boermans et al. 1988), the affected goat initially showed polydipsia, constipation, corneal opacity, and a progressive incoordination, especially in the hindlimbs. This was followed by depression and increasing salivation. On the fifth day, before death, clonic-tonic convulsions were observed accompanied by blindness, vertical nystagmus, decreased rumen motility, diarrhea, and a subnormal temperature.
Clinical Pathology and Necropsy
Hypocalcemia may be detectable in affected goats, but the degree and occurrence are variable. Hyperphosphatemia and hypermagnesemia also may occur. A moderate to severe azotemia is usually present. Urine samples may demonstrate proteinuria and crystalluria. A characteristic rectangular parallelepiped shape for calcium oxalate dihydrate crystals found in the urine of a goat has been reported (Clark et al. 1999). When oxalate toxicosis is suspect, oxalate levels should be measured in suspected plants, if available.
Oxalate toxicosis is most accurately diagnosed at necropsy. The rumen content should be carefully inspected for evidence of oxalate-containing plants, and oxalate concentration of the rumen content can be measured. In affected goats, the rumen oxalate content ranged from 0.5 to 1.8% (Gonzalez 1983). Inflammation and hemorrhage of the gastric and intestinal mucosa and serosa, hydrothorax, and ascites are common but non-specific findings. The kidneys are edematous and swollen.
A characteristic but inconsistent finding is a clearly demarcated yellow to yellow-green, streaked appearance of the renal cortex on visual inspection, with the medulla remaining reddish brown. Kidney oxalate content in affected goats ranged from 2.9 to 7.1%. Histologically, the renal tubules are dilated and filled with birefringent oxalate crystals. These crystals may also be found in vessel walls, especially in the rumen vasculature. Similar histologic renal lesions are observed in ethylene glycol toxicosis. Glycolic acid, a stable metabolite of ethylene glycol, can be measured in serum, urine, and ocular fluid post mortem to support the diagnosis of ethylene glycol toxicosis.
Diagnosis
Diagnosis is based on a history of exposure, clinical signs, and often oxalate crystals in the renal tubules at necropsy. In the live animal, other causes of hypocalcemia, both metabolic and nutritional, must be ruled out. When signs of excitation or convulsions occur, primary neurologic diseases must be considered. The differential diagnosis for convulsions is given in Chapter 5.
Treatment
The prognosis for recovery is guarded once clinical signs appear. Animals at risk should be removed from the offending source of oxalates and alternate food sources provided. Subcutaneous administration of 50-100 mL of calcium borogluconate helps to counter the potential hypocalcemia of animals at risk. Severely affected individuals may require intravenously administered calcium salts and intravenously administered fluid therapy to counter the accumulation of oxalate crystals in renal tubules and the development of severe nephrosis. Oral administration of large quantities of water may be beneficial when there are economic constraints to therapy.
In ethylene glycol toxicosis, the prognosis is poor once signs appear. If the ingestion is recognized before signs begin, oral administration of activated charcoal (0.75-2.0 g/ kg bw in water) may be beneficial in detoxification. When signs are present, intravenous fluid therapy should include sodium bicarbonate to counter the severe acidosis. Calcium borogluconate is also indicated to counter hypocalcemia. Neurologic signs may be controlled with diazepam. The administration of ethanol intravenously to serve as a competitive inhibitor of ethylene glycol metabolism in the liver has been used as an effective therapy in dogs and cats, but has not been reported in ruminants. The dose in dogs is 5.5 mL of 20% ethanol per kg given intravenously every four hours. It should be used cautiously, as ethanol itself can be toxic.
A more recent treatment option used in dogs and cats is 4-Methylpyrazole (4-MP, fomepizole), which inactivates alcohol dehydrogenase without the adverse effects of ethanol. The dose of 4-MP (5% solution [50 mg/mL]) in dogs is 20 mg/kg bw initially, followed by 15 mg/kg at 12 and 24 hours, and 5 mg/kg at 36 hours, all intravenously (Grauer 2016). To date, there are no reports of the use of fomepizole in goats or other ruminants.
Control
Controlling oxalate toxicosis involves minimizing the grazing of animals on range with heavy cover of oxalate-containing plants. When such grazing is necessary, supplementary feed should be provided for at least the first few days to allow time for the rumen flora to adapt to more efficient degradation of oxalates. A good calcium source such as dicalcium phosphate helps to form calcium oxalate in the alimentary tract, thereby limiting absorption of oxalate.
Oak Poisoning
Oak poisoning (Quercus spp.), which is caused by ingesting large quantities of young leaves, blossoms, buds, stems, or acorns, produces considerable morbidity and mortality in cattle and sheep. The toxic principle is believed to be a gallotannin and it produces a severe intestinal irritation and a characteristic nephrosis. Animals show depression, abdominal cramping, and constipation, followed by bloody, mucoid feces, and they often succumb to uremia.
Goats appear highly resistant to oak poisoning, possibly because of comparatively increased levels of tannase enzymes in the rumen mucosa. It has been demonstrated in vitro that infusion of tannin into goat rumen fluid increases fermentation activity, while it depresses activity in sheep rumen fluid (Narjisse and El Hansali 1985). Goats are routinely used to clear scrub oak from pastures to make them safe for sheep and cattle. While goats do not have high levels of proline-rich proteins capable of binding tannins, as are found in some other herbivore species, there is evidence that there are other, as yet unspecified proteins in their saliva that do have a high tannin-binding affinity (Schmitt et al. 2020).
The only report of spontaneous oak poisoning in goats involved consumption of Quercus floribunda in Sikkim. Affected animals showed signs of abdominal pain and constipation, followed by hemorrhagic diarrhea and death (Katiyar 1981). In experiments, clinical signs of oak poisoning typically seen in cattle were produced in goats when they were fed a diet consisting almost exclusively of fresh shin oak (Quercus havardi) for an extended period (Dollahite 1961). In an unrelated study, goats fed 1 kg of dry oak leaves daily for three days showed no ill effects, and it was concluded that goats can browse oak with impunity. In this same study, however, oral administration of tannic acid (1 L of a 7% solution) resulted in an acute hemolytic crisis with hemoglobinuria. A regenerative response developed 7-14 days later, with macrocytes and reticulocytes observed. A transient thrombocytopenia also occurred 72 hours after administering tannic acid (Begovic et al. 1978).
If oak poisoning is suspected in goats, the animals should be removed from the source of oak and treated with oral purgatives, including mineral oil and/or magnesium sulfate. Intravenous fluid therapy may be required to correct dehydration and acidosis.