Nutritional Myodegeneration
John Maas • Stephanie J. Valberg
■ Definition and Etiology Nutritional myodegeneration (NMD; also known as white muscle disease, stiff lamb disease, and nutritional muscular dystrophy) is an acute myodegenerative disease of cardiac and skeletal muscle caused by a dietary deficiency of selenium or vitamin E.115-118 This syndrome occurs in most farm animal species but is most commonly found in young, rapidly growing calves, lambs, kids, and foals, particularly those born to dams that consumed selenium-deficient diets during gestation.
An in utero form of NMD may occur with affected animals showing clinical signs soon after birth. The disease has also been reported in yearling and adult cattle and occasionally adult horses. Selenium and vitamin E appear to be synergistic in preventing NMD. However, on the basis of prophylaxis and response to treatment, selenium deficiency appears to be more important.■ Clinical Signs There are two distinct syndromes of NMD: a cardiac form and a skeletal form. The cardiac form is associated with acute signs of myocardial decompensation, whereas the skeletal form results in stiffness, weakness, and difficulty in ambulation.
The cardiac form of NMD usually has a sudden onset of depression, weakness, respiratory distress, rapid irregular heartbeat, severe debilitation, and often death within 24 hours. Occasionally an animal responds to therapy, but it often fails to thrive because of residual myocardial damage. Animals with predominantly cardiac signs can also manifest mild skeletal muscle problems associated with NMD. Lesions are present in the heart, diaphragm, and intercostal muscles.
The skeletal form of NMD frequently has a slower onset characterized by muscular weakness, stiffness, trembling, and recumbency with notably hard and painful muscles on palpation. Commonly affected muscle groups may include the gastrocnemius, semitendinosus, semimembranosus, and biceps femoris and muscles of the lumbar, gluteal, and neck regions.
If the diaphragm and intercostal muscles are affected, the animal may show respiratory distress and evidence of increased abdominal effort when breathing. The muscles of the tongue may be involved, resulting in dysphagia. Dysphagia, especially in foals and lambs, may be the only sign. Some animals exhibit what appears to be abdominal pain with violent thrashing. Animals with skeletal NMD often respond favorably to treatment and rest. Improvement is evident after a few days, and within 3 to 5 days animals can often stand and walk.Differentiation of NMD from other diseases causing sudden death or recumbency is important. Infectious diseases resulting in septicemia, pneumonia, and toxemia may have similar presenting signs. Acute heart failure resulting from cardiac anomalies; cardiotoxic agents such as those found in plants (oleander, cassia, yew, white snakeroot, and gossypol toxicity from cottonseed); and the ionophore antibiotics should also be considered. Other diseases causing stiffness of gait, weakness, and recumbency with no change in mental status must be differentiated from NMD. Spinal cord compression, cerebellar disease, suppurative and nonsuppurative meningitis or myelitis, polyarthritis, neurotoxins such as organophosphates, tetanus, pelvic fractures, and parasitic myositis all can cause recumbency. Clostridial myositis and traumatic injuries to muscles, long bones, and joints should be considered. Diseases characterized by abdominal pain may resemble NMD because they may also cause stiffness of gait, weakness, and recumbency.
■ Clinical Pathology Significantly elevated CK, AST, and LDH activities and myoglobinuria occur during the acute phase of myodegeneration. Progressively decreasing activities of CK can be used as a prognostic indicator of a reduction in the myodegenerative process. In foals, other reported abnormal laboratory findings include variable hyperkalemia, hyperphosphatemia, hyponatremia, and hypochloremia.118 Evidence of dehydration, reflected by elevated serum protein concentrations and hemoconcentration, is common in nonambulatory animals unable to nurse or drink water.
The selenium status of an animal or members of a group can be determined by laboratory analysis of tissue biopsies and whole blood (Table 42.2). Vitamin E status in serum or plasma is satisfactory for assessing intermediate to long-term nutritional status; however, short-term supplementation or injections can confuse interpretation of circulating levels of selenium or vitamin E. Tissue biopsies and tissue specimens obtained at slaughter and necropsy provide an indication of storage and can also be used to assess herd status and success of supplementation. Whole blood selenium analysis is preferred over plasma and serum.119 Whole blood selenium concentrations ranging from 0.07 to greater than 0.1 ppm (μg/ mL) are considered normal in large animals. Normal liver concentrations of selenium are 0.9 to 1.75 μg∕g of dry weight (DW), 0.9 to 3.5 μg∕g DW, and 1.05 to 3.5 μg∕g DW for cattle, sheep, and horses, respectively.120 Selenium-dependent glutathione peroxidase (GSH-Px) formed in the RBCs during erythropoiesis also provides an index of body selenium status.
■ TABLE 42.2
Deficient, Marginal, and Normal Concentrations of Whole Blood Selenium and GSH-Px Activities in Sheep and Cattle67,71
| Whole Blood Selenium (ppm) | GSH-Px (U/mg Hb/min) | Category | Interpretation |
| 0.01-0.04 | 0-15 | Deficient | Selenium supplementation is always beneficial |
| 0.05-0.06 | 15-25 | Marginal | Selenium supplementation is often beneficial |
| ≥0.07 | 25-500 | Normal | Selenium supplementation is never beneficial |
GSH-Px assays are performed by different procedures in individual laboratories, and quantitative relationships between blood selenium concentrations and blood GSH-Px activities can vary.
These numeric relationships are site specific, and interpretation must account for these differences.GSH-Px, Glutathione peroxidase; Hb, hemoglobin; ppm, parts per million.
Cross-reacting enzymes, such as glutathione reductase, are not found in erythrocytes. Adequate GSH-Px activities are greater than 30 U/mg of hemoglobin per minute in cattle, 60 to 180 U/ mg of hemoglobin per minute in sheep, and 20 to 50 U/mg of hemoglobin per minute in horses. However, GSH-Px reference values are only specific to the laboratory where the analysis is performed and must be validated by comparison with blood selenium concentration. The activity of GSH-Px in RBCs of domestic species remains constant for 4 to 6 days when maintained at 39° F (4° C); after this time, significant decreases occur. The critical concentration of vitamin E (α-tocopherol) in plasma is 1.1 to 2 ppm (pg/mL) in large animals. Vitamin E deteriorates rapidly in plasma samples. Therefore plasma or serum samples for α-tocopherol analysis need to be put on ice immediately, protected from light by wrapping in tin foil, and stored (-21° F/-70° C) if analysis is to be delayed.
■ Pathophysiology The effects of selenium and vitamin E deficiency have been postulated to result, at least in part, from the destruction of cell membranes and proteins leading to a loss of cellular integrity.115,121 Selenium, which has been shown to be an essential component of at least five selenopro- teins122 (three GSH-Px enzymes; a deiodinase in liver and kidney that converts T4 to T3; and selenoprotein P, a plasma protein of unknown function), and vitamin E (α-tocopherol) serve as biologic antioxidants. During normal cellular metabolism, highly reactive forms of oxygen (free radicals) are produced. These include hydrogen peroxide, hydroperoxides, lipoper- oxides, superoxide, various hydroxy radicals, and singlet oxygen. Vitamin E is active within the cell membrane as a lipid-soluble antioxidant that scavenges free radicals that otherwise might react with unsaturated fatty acids to form lipid hydroperoxides.
In contrast, GSH-Px destroys hydrogen peroxide and lipo- peroxides that have already been formed and converts them to water or relatively harmless alcohols. Other enzymes such as catalase and superoxide dismutase are also involved in this protective process.Apparently important interrelationships exist among the selenium and vitamin E status of the animal, the level of polyunsaturated fatty acids (PUFAs) in the diet,115,121 and NMD, particularly in ruminants.115 PUFAs of dietary origin can undergo peroxidation to hydroperoxides forming toxic free radicals. During active growing periods, pasture grasses and plants contain high concentrations of linolenic acid, a PUFA. Under normal conditions the rumen is thought to be important in saturating dietary unsaturated fatty acids. However, concentrations of PUFAs in the plasma often increase in calves recently turned out to pasture, possibly enhancing the chance of free radical formation and tissue damage. This indicates that the capacity of the various protective mechanisms can be overwhelmed by dietary factors such as high levels of PUFA. Not surprisingly, selenium- or vitamin E-deficient animals may be at a greatly increased risk of tissue oxidative damage when exposed to such diets. However, the potential for induction of NMD by this process should not be overemphasized because calves on a milk diet may be severely affected.
The precise interrelationships among selenium, vitamin E, other metabolic factors, and triggering mechanisms in NMD are not fully understood because many animals deficient in selenium or vitamin E have no evidence of muscle disease. In certain situations, deficiencies of both selenium and vitamin E are necessary for disease to occur. In other animals NMD can occur when a deficiency of only one of the agents is present and the other is normal in blood and tissues.
■ Epidemiology NMD occurs in all farm animals and is seen most commonly in young, rapidly growing calves, lambs, kids, and foals.
The occurrence of NMD in very young animals usually reflects a deficiency in their dams during a substantial portion, if not all, of the gestation period. The selenium and GSH-Px values of neonatal calves tend to be similar to those of their dams.123,124Marginally to severely selenium-deficient areas occur throughout a large portion of the United States and other countries of the world. Forages and grains produced in the northeastern and eastern seaboards and northwestern regions of the United States are particularly deficient because of low soil levels of selenium. Acid soils and those originating from igneous (volcanic) rock are often selenium deficient, as are those having high sulfur content or soils treated with sulfur- containing fertilizers. Sulfur inhibits selenium uptake by plants and absorption by animals. Different forages in a specific area will also vary in their selenium content. Legumes take up less selenium than do grasses. Also, forage selenium concentrations are lowest during periods of rapid growth such as in the spring and during times of highest rainfall.
Vitamin E deficiency occurs most commonly when animals are fed poor-quality hay, straw, or root crops. Grain treated with propionic acid and having high moisture content is commonly vitamin E deficient. Storage of grain crops for extended periods results in marked decreases in their vitamin E content. Calves fed milk replacers containing fish oil, linseed oil, or soybean or corn oil, all of which increase the dietary levels of unsaturated fatty acids, require increased dietary supplementation of vitamin E to avoid deficiency. In contrast, cereal grains, green growing pastures, and properly prepared hay usually have adequate vitamin E.
In young ruminants the majority of NMD cases occur in calves, 2 to 4 months of age, during the spring and summer months in association with exercise when at pasture, although congenital and perinatal cases do occur. Histologic lesions consistent with NMD have also been seen in late-term aborted fetuses.120 These findings are suggestive of an in utero form of NMD in large animals. Yearling cattle housed during the winter, fed diets high in grain with high moisture content, and then turned out in the spring may also be affected. Lambs born in confinement and turned out to pasture at 1 to 3 weeks of age frequently develop signs of NMD. Stresses such as
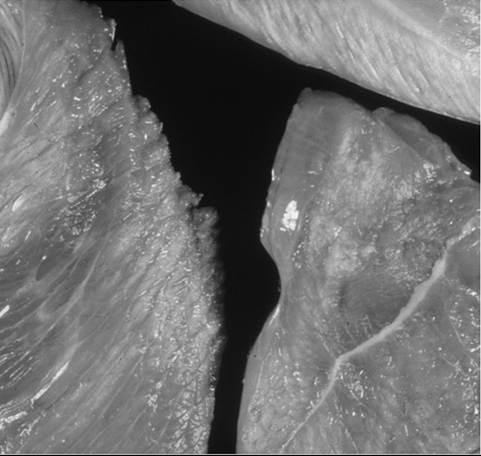
FIG. 42.12 White streaks within diffusely pale skeletal muscle due to nutritional myodegeneration.
transport, herding, and driving can also precipitate signs of NMD. In horses, NMD generally occurs during the first year of life with most cases observed from birth to weaning.116,125
■ Necropsy Findings Bilaterally symmetric myodegeneration is a consistent finding in NMD. Skeletal muscle degeneration is characterized by pale discoloration and a dry appearance of affected muscle, white streaks in muscle bundles, calcification, and intramuscular edema (Fig. 42.12). The white streaks seen in muscle bundles represent bands of coagulation necrosis or, in chronic cases in which insults may have occurred weeks before, may represent fibrosis and calcification. Affected muscle bundles are often adjacent to apparently normal or minimally affected muscle. The color of normal muscle in young calves is pale because of reduced myoglobin concentrations; therefore close inspection and histologic examination are necessary in cases of suspected NMD. Cardiac muscle undergoes changes similar to those of skeletal muscle. In calves the left ventricle and septum are most frequently involved (Fig. 42.13), but in lambs both ventricles are usually involved. Myocardial degeneration usually extends through the full thickness of the ventricular wall.
Histologically, affected muscle fibers may be hypercontracted and fragmented with some mineralization of muscle fibers and others undergoing macrophage infiltration. In yearling cattle, type I muscle cells are more frequently affected.
■ Treatment and Prognosis In the cardiac form of NMD, myocardial damage is often extensive and incompatible with life. In contrast, the skeletal form of NMD is more generally amenable to treatment, although the prognosis for clinical recovery from the skeletal form of NMD is guarded and depends often on whether secondary complications such as respiratory disease develop. In all cases of NMD, therapy should involve specific supplementation with selenium and vitamin E and general supportive care.
Alleviation of selenium-responsive NMD requires the use of injectable selenium products. These are available with selenium concentrations varying from 1 to 5 mg/mL, with all products containing 50 mg/mL (68 IU) of vitamin E as DL-α-tocopheryl acetate. The label dose for selenium is 0.055 to 0.067 mg/kg (2.5 to 3 mg/45 kg) body weight given intramuscularly or subcutaneously.

FIG. 42.13 Pale areas of muscle necrosis in the myocardium of a calf with nutritional myodegeneration.
Dosage of these injectable products should not be greatly increased above the label dose to prevent an inadvertent selenium toxicosis. However, when using the vitamin E/selenium combinations, the amount of vitamin E in these combination products is present as a preservative for the solution and is therefore insufficient for vitamin E supplementation. Oral supplementation is the general approach to provide additional dietary levels of vitamin E. Vitamin E can be obtained from natural or synthetic sources, which differ in bioavailability. In order for α-tocopherol acetate to be used in the body, the ester has to be removed and the α-tocopherol made water dispersible by the action of bile salts (micellization), which can limit α-tocopherol acetate absorption in the horse. To further enhance the bioavailability of α-tocopherol, water-dispersible formulations of vitamin E have been developed. The biopotency of these compounds in horses is much greater than synthetic vitamin E. When tested, two of the commercially available water- dispersible natural vitamin E products had a bioavailability 5.59 (Elevate WS [Kentucky Performance Products, Versailles, Ky.]) and 6.13 (Nano-E [Kentucky Equine Research, Versailles, Ky.]) times higher than synthetic vitamin E acetate (D-α-tocopheryl acetate). Recommended levels of supplementation for calves range from 15 to 60 mg of DL-α-tocopheryl acetate per kg of dry feed. For horses, a daily supplement of 600 to 1800 mg per os of DL-α-tocopheryl acetate has been recommended.125
Studies with injectable selenium show that absorption and distribution occur rapidly.126 It is thought that incorporation of selenium into heart, skeletal muscle, and other tissues may be rapid and could account for the rapid improvement in clinical signs seen in reversible cases. The discovery of four new selenoproteins may help explain these clinical observations.122 This improvement can occur even though blood GSH-Px activity rises slowly because of the delay caused by erythropoiesis and release of RBCs from the bone marrow.126 However, platelet GSH-Px activity rises within hours and may be a more accurate reflection of changes in muscle and other tissues.
Supportive therapy may include administration of antibiotics to help combat secondary pneumonia and infected decubital lesions that are common in recumbent patients. Provision of adequate energy intake and attention to the fluid and electrolyte balance are of critical importance if recovery is to be successful.
■ Prevention and Control The prevention and control of NMD are achieved through supplementation of both selenium and vitamin E. The use in ruminants of rumenoreticular boluses, which release a precise amount of selenium daily, has been commonplace in many countries of the world; however, current guidelines should be checked to ensure they are not permitted. These slow-release boluses can replace supplementation by salt mixtures or by injections and are extremely valuable in extensive grazing systems. Alternatively, individual animals can be supplemented by periodic (30- to 60-day intervals) injections of selenium/vitamin E preparations to help maintain body concentrations and assist in transplacental transfer of selenium to the fetus.
Oral supplementation for horses at 1 mg of selenium per day increases blood selenium concentrations above levels known to be associated with NMD.127 Supplementation of pregnant mares is advised in areas known to be selenium deficient; however, only limited selenium may cross the placenta.117 Supplementation during lactation increases the levels of selenium in milk and thus provides a potential means of selenium supplementation in foals; however, evidence in cattle indicates that this increased level of selenium in milk may not meet nutrient requirements.
Regardless of the method of supplementation, periodic blood (or tissue) sampling of animals at risk is recommended to ensure desired levels of selenium. In high-risk areas, samples should be taken every 60 to 90 days to determine selenium status in susceptible animals and every 6 to 12 months to monitor supplementation. On the basis of these assessments, adjustments to the rate or extent of selenium supplementation may be made.
Feeding animals properly prepared and stored hay and grain or allowing them access to high-quality green forage should ensure adequate vitamin E intake.
Masseter Muscle Myodegeneration
Adult horses with selenium deficiency may be clinically normal or can present with acute clinical signs of bilateral swelling of the masseter muscles, trismus, dysphagia, and salivation.128-131 Although postural and locomotor muscles may appear normal on clinical examination, postmortem of horses with masseter muscle myonecrosis has shown histopathologic evidence of bilateral symmetric lesions in muscles of the hind and thoracic limbs. Tachycardia and dysrhythmias may indicate the presence of myocardial damage. Accompanying clinical pathologic findings include pigmenturia, elevated serum AST and CK activity, and elevated cardiac troponin concentrations. Ultrasonography can be used to determine the extent of masseter muscle swelling or atrophy, as well as the presence of myocardial dysfunction. Prognosis is guarded, but there are individual reports of successful treatment. Important aspects of treatment include nutritional support via stomach tube, IV fluids, analgesics, IM selenium (0.055 to 0.067 mg/kg), and oral vitamin E (1000 to 5000 IU∕day). Progression to bilateral muscle atrophy is common and may resolve after a period of months. Without early treatment, permanent trismus can occur due to muscular atrophy and fibrosis. Ruleouts for masseter swelling include parasites—most commonly Trichinella spiralis, Halicephalobus species, or Haycocknema perplexumv32—trauma, and fibrosis due to trauma or chronic abscessation.
Vitamin E-Deficient Myopathy
Some horses with clinical signs of EMND and a deficiency in vitamin E are not diagnosed antemortem with EMND because they lack evidence of neurogenic atrophy in the sacrocaudalis dorsalis (SC) muscle. A recent study suggests that many such undiagnosed cases are the result of a specific myogenic presentation of vitamin E deficiency.133 With vitamin E-deficient myopathy, the clinical presentation resembles EMND; however, sacrocaudalis muscle lacks evidence of neurogenic atrophy but contains an abnormal moth-eaten staining pattern of mitochondria. Muscle α-tocopherol concentrations from affected horses are low, but serum α-tocopherol concentrations are inconsistently low. This vitamin E-deficient myopathy has likely been missed previously because formalin-fixed biopsy specimens are most often evaluated for a diagnosis of EMND and mitochondrial staining is not possible with this fixative. The observed generalized weakness in the horses with abnormal mitochondrial stains could be due to a reversible manifestation of skeletal muscle mitochondrial oxidative stress associated with vitamin E deficiency. Horses can recover completely after vitamin E therapy (5000 IU/day per os for >3 weeks) (Fig. 42.14). Vitamin E-deficient myopathy could be an entity unto itself or a predecessor to development of EMND, but this distinction was not evaluated in the study because all horses successfully responded to vitamin E therapy, precluding a postmortem examination.
Toxic Causes of Rhabdomyolysis
Stephanie J. Valberg
Ingestion of toxic substances in feed or forage is a common cause of toxic rhabdomyolysis.
IONOPHORES. Ionophores are commonly added to feeds for their growth promotion and coccidiostat properties. Species differences in sensitivity to ionophores and the variety of ionophores on the market have led to several cases of ionophore- induced toxicosis. Rhabdomyolysis and cardiomyopathies are common sequelae to ionophore toxicosis. Experimental studies have indicated that LD50 values for monensin are 2 to 3, 12, 17, 26, and 21 to 36, for horses, sheep, pigs, goats, and cattle, respectively. Feed concentrations of 100 g/ton and 400 g/ton have been fatal to sheep and cattle, respectively.134,135 Newborn calves dosed with 100 mg lasalocid twice daily, for cryptosporidiosis, experience muscle necrosis.136 Other ionophores include naracin, salinomycin, and laidlomycin. Ionophores are quickly eliminated from the body after exposure.
CHEMICAL TOXINS. Several chemical agents have been associated with muscle necrosis on rare occasions. Parenteral products, insecticides, and feed contaminants have been implicated. Muscle necrosis has been reported in cattle and pigs after receiving injections of lidocaine, diazepam, digoxin, levamisole, nitroclofene, pentazocine, thiazinamium, chloramphenicol, and oxytetracycline and in horses after injectable ivermectin administration. One of 70 horses poisoned with blister beetles developed muscle necrosis.137 Animals with organophosphate toxicosis, particularly parathione, may develop muscle necrosis.138-140 Several miniature horses being fed a complete feed containing tetrachlorovinphos, a feed-through fly control agent, were reported to develop chronic myonecrosis involving masseter, tongue, neck, respiratory and postural

FIG. 42.14 A horse with vitamin E-deficient myopathy before (A) and after (B) 6 months of vitamin E treatment. Before vitamin E treatment, notice the marked generalized muscle atrophy; following treatment, notice the normal muscle mass.
muscles, and occasionally cardiac muscle.141 Affected horses showed signs of lethargy, dysphagia, fasciculations, tachypnea, and tachycardia. Muscle tissue showed evidence of chronic myonecrosis and lipid accumulation. Myonecrosis was attributed to acetylcholine accumulation at muscarinic and nicotinic sites producing oxidant stress. Low selenium concentrations may contribute to the toxicosis.
TOXIC PLANTS. Gossypol is of greatest significance in swine. Monogastrics, including young calves, should not ingest feed containing more than 200 ppm gossypol. Mature ruminants may tolerate 20 g of gossypol/head/day. This normally amounts to 5 to 6 lb of whole cottonseed per head per day.142 Two common forage toxins that cause myonecrosis are Cassia spp. and tremetone-containing plants. Cassia obtusifolia (sicklepod) is prevalent in the southeastern United States, and ingestion of seeds by swine, ruminants, or horses may cause a degenerative myopathy and cardiomyopathy with evidence of myofiber atrophy, segmental necrosis, and mitochondrial disruption.142 White snakeroot (Eupatorium rugosum) grows in shaded areas of the eastern and central United States, and rayless goldenrod (Isocoma wrightii) is common in the Southwest on open pastures. These tremetone-containing plants can cause a fatal cardiomyopathy and severe skeletal muscle degeneration in horses when ingested at 0.5% to 2% of body weight.143,144 Other grazing livestock are likely to be affected by ingestion of these plants at 2% of body weight. Tremetone remains active in hay and in the stalks of the dead plants on pasture, so both the fresh and the dried form of the plants should be kept from livestock.145 Microsomal activation of the toxin in the liver may be necessary for toxic effects.143
Marshmallow Toxicity
Marshmallow (Malva parviflora), also known as small-flowered mallow, cheeseweed mallow, and little mallow, is a common weed found in pastures of grazing animals with extensive distribution, including in regions of Europe, Asia, North and South America, Australia, and New Zealand. The two cyclopropene fatty acids, malvalic acid and sterculic acid, are thought to be the main toxic components of plants.146 Horses consuming marshmallow with little else to eat developed signs of sweating and muscle fasciculations progressing to recumbency and had elevated serum CK, AST, and lactate.146 Increases in serum cyclopropene fatty acids, large increases in C14 to C18 acylcarnitine concentrations, and smaller increases (up to eightfold) in other acylcarnitines such as C2 to C5 suggest that the toxin disrupts long-chain fatty acid metabolism.146
Seasonal Pasture Myopathy and
Atypical Myopathy
EPIDEMIOLOGY. A highly fatal acquired lipid storage myopathy of pastured horses occurs in the fall and less often in the spring in Europe and central and northeastern parts of North America.147-151 Affected horses are usually young or new to affected pastures and kept on wooded pastures for more than 12 hours a day without additional feed provided. Windy weather often precedes outbreaks.152,153
■ Clinical Signs Clinical signs develop acutely and include muscular weakness, sweating, fasciculations, stiffness, tachycardia, tachypnea, recumbency, and when urine is observed, myoglobinuria. A rapid rise in respiratory rate is usually followed by collapse and death from respiratory or cardiac failure.
■ Diagnosis The most notable change in serum biochemistry is a marked increase in serum CK and AST activity, which is often accompanied by hyperglycemia, lactic acidemia, and in some cases elevated serum troponin I concentrations.154 A definitive diagnosis can be made by a pattern of accumulation of serum acylcarnitines and urine organic acids and glycine conjugates typical of a deficiency in multiple acyl-CoA dehydrogenases, as well as isolation of the conjugated toxic metabolite methylene cyclopropyl acetic acid (MCPA) and hypoglycin A in blood or urine.155-158 Serum vitamin and selenium, as well as urine tremetone, concentrations are normal. Postmortem findings include extensive necrosis in deep postural and respiratory muscles and, in 50% or more of cases, in myocardium. Frozen sections of myocardium, intercostal, diaphragm, or deep postural muscles show marked intracellular lipid accumulation in oxidative fibers (oil red O stain).147,150
■ Pathophysiology Seeds of Acer species trees such as the box elder (Acer negundo) and the European sycamore maple (Acerpseudoplatanus) (Fig. 42.15) contain the toxic nonproteo- genic amino acid hypoglycin A.157-159 Hypoglycin A is metabolized in the liver to MCPA, and MCPA CoA irreversibly binds to multiple acyl-CoA dehydrogenases, enzymes that are essential for metabolism of short- and medium-chain fatty acids and

FIG. 42.15 Box elder seeds that contain the toxin hypoglycin A, which causes seasonal pasture myopathy.
branched chain amino acids. Accumulation of fat esters can damage muscle cell membranes, and an energy deficiency also arises from an inability to metabolize fat.
■ Treatment and Prognosis Less than 75% of horses survive.153 Early aggressive fluid therapy and antioxidant and anti-inflammatory treatment, including dimethyl sulfoxide, vitamin E, vitamin C, riboflavin, and NSAIDs, are indicated.147 Although many older horses are asymptomatic on pastures with Acer species trees, young horses or new horses should not be pastured with box elder or European sycamore maple trees in the fall. Provision of additional feed or reducing grazing time during the fall may also decrease the incidence of pasture- associated myopathies.