Obstructive Intestinal Diseases
David Francoz • Charles L. Guard
Definition and Etiology
Several conditions may lead to obstruction of the flow of ingesta through the intestinal tract. These conditions can be divided into functional or mechanical obstructions.
Functional obstructions (pseudoobstruction or ileus) are the consequence of neuromuscular perturbations of the gastrointestinal tract. Mechanical obstructions are the consequence of a physical obstruction of the intestinal tract secondary to digestive tract lesions (intussusception, volvulus, or congenital lesions) or extradigestive lesions (mesenteric fat necrosis, fibrous adhesions, or hernia). Each of the specific diseases is discussed in the following paragraphs and summarized in Table 32.21.Clinical Signs and Differential Diagnosis
Acute manifestations of obstructive diseases include a reduced amount of feces or failure to pass feces, progressive abdominal enlargement with areas of tympanic resonance on the right side of the abdomen, and sometimes colic. If pain is severe, forestomach atony may occur. Mechanical obstructions may lead to circulatory shock and collapse. Electrolyte abnormalities depend on the site of the obstruction; obstructions in the jejunum or near the duodenum or pylorus lead to sequestration of abomasal secretions and result in hypochloremic, hypokalemic metabolic alkalosis, whereas those in the cecum, colon, or rectum may lead to dehydration without alkalosis. If bowel necrosis or rupture occurs, acidosis may result from the circulatory collapse that accompanies peritonitis and the absorption of toxins.
Volvulus of the Duodenal Sigmoid Flexure
A syndrome affecting the duodenal sigmoid flexure was reported in Holstein cattle by Vogel and colleagues.1 The etiologic and pathophysiologic features of this condition are not known, but the authors advanced a potential role of duodenal ulcers or previous omentopexy (years to months before development of volvulus of the duodenal flexure).
Clinical presentation resembles abomasal volvulus with anorexia, decreased milk production, scant feces, tachycardia, moderate dehydration, tympanic resonance in the tenth to twelfth right intercostal spaces, and succussion of fluid in this area.1 Serum biochemistry panels revealed a severe hypokalemic and hypochloremic metabolic alkalosis, as well as hyperbilirubinemia and increased liver enzyme levels. Interestingly, those modifications were more pronounced than those observed in cases of abomasal volvulus. Confirmation of the diagnosis is made by palpation of a counterclockwise duodenal sigmoid flexure volvulus during right flank exploratory laparotomy. Treatment consists of manual reduction of the volvulus, massage of the duodenum, and fluid therapy to correct electrolytic disorders. Prognosis of the condition is reported to be fair; 22 of 29 animals were treated successfully.■ TABLE 32.21
Causes of Intestinal Obstruction in Ruminants
| Disease | Animals Most Commonly Affected | Signs |
| Intestinal atresia or stenosis | Neonates | No feces; abdominal distention |
| Intestinal volvulus around mesenteric root | All ruminants; more common in neonates | Colic; rapid abdominal distention; collapse; shock |
| Intussusception | All ruminants; large or small intestine of neonates; small intestine of adults | Colic early, then chronic low-grade pain; dehydration; mucus plus blood in dark red feces; slow abdominal distention; decreased fecal output; mass palpated rectally; distended loops of intestine palpated rectally |
| Cecal dilation and volvulus | Adult dairy cattle in early lactation | Mild to severe colic; distended abdomen, especially upper right; ping in right paralumbar fossa; distended cecum palpated rectally |
| Intestinal tumors | Sheep, rare in cattle | Progressive weight loss; in cattle, mass may be palpable rectally; in sheep, mass identified by celiotomy or necropsy |
| Mesenteric fat necrosis | Cattle, especially Channel Island breeds | Masses possibly discovered on routine examination; progressive weight loss; scant or no feces; dilated loops of bowel palpated rectally |
| Intestinal incarceration | All ruminants | Same as for intussusception |
| Ileus | All ruminants | Scant or no feces; right-sided ping; succussable fluid on right; often associated with peritonitis |
Intestinal Atresia or Stenosis
Intestinal atresia or stenosis is a congenital anomaly reported in calves and lambs.
Clinical signs usually become evident within a few days after birth. Animals with anal or distal rectal atresia usually have the slowest onset of signs, whereas proximal obstructions lead to more rapid onset of signs. Malformations of the anus and rectum are believed to be hereditary,2 and breeding of surgically corrected survivors should be discouraged. Jejunal atresia in Jersey cows is reportedly inherited as an autosomal recessive trait. The etiopathogenesis of atresia coli in calves is not well understood, but autosomal recessive inheritance has been reported,3 and Holstein calves seem to be predisposed to its development.4 Rectal palpation of the amniotic vesicle for diagnosis in early pregnancy (collapse after the intestine proximal to the obstruction becomes distended with fluid and gas. Tympany may be easily detected by percussion. If the anus and rectum are normal, a digital examination usually reveals only mucus or blood (or both). Because the rectal and descending colon walls are thin in cases of atresia coli, retrograde tubes or catheters should be used with extreme caution to prevent rupture of the bowel or should be avoided completely.6 Complete intestinal volvulus must be considered in the differential diagnosis, but the histories in the two conditions are often different.Surgical repair is indicated if the animal is of high value. However, the prognosis for normal and productive life is guarded. Many affected neonates develop severe complications in the immediate postoperative period. Pneumonia, sepsis, and peritonitis are among the most frequent complications, and the development of bowel stasis or ileus is common. A prognosis of a rate of 39 to 44% short-term survival has been reported.6-8 When registered animals are involved, a letter should be sent to the appropriate breed registry stating that the defect has been corrected.
Volvulus of the Large and Small Intestine Around the Mesenteric Root
Volvulus of the large and small intestines around the mesenteric root leads to severe colic and relatively rapid abdominal enlargement.
Circulatory shock develops rapidly. Ruminants of any age are susceptible, but most cases are seen in preruminant neonates. Severe colic is seen, including kicking and vocalization. Affected animals rapidly become recumbent, and hypovolemic shock develops. The heart and respiratory rates increase drastically as shock develops. Variable-pitched resonant sounds may be heard bilaterally over the abdomen with the use of simultaneous percussion and auscultation. In affected adult cattle, the tympany is restricted to the right side. Succussion reveals splashing sounds, particularly on the right side. Rectal examination reveals distended loops of gut. Surgical correction is the only successful treatment option.9 The prognosis depends on the degree of devitalization of bowel. Animals that undergo surgical correction during the early stages respond better.Volvulus of smaller portions of the intestinal tract leads to signs similar to those of complete intestinal volvulus around the root of the mesentery, but often the onset is more progressive. Colic with accompanying tachycardia, ruminal stasis, and anorexia is present to varying degrees. The abdomen is moderately distended on the right, as viewed from the rear. Simultaneous auscultation and percussion on the right side reveal multiple-pitched, resonant pings from the gas accumulated proximal to the obstruction. Rectal examination may reveal scant feces, mucus, or blood. The affected bowel usually is palpable as grossly distended with gas and some fluid. Because of their relatively long mesentery, the spiral colon (or part of it), the distal jejunum, and the proximal ileum may develop an obstructive volvulus. Therapy requires correction of acid-base and electrolyte abnormalities and rapid surgical manipulation by means of celiotomy.
Intussusception
In the development of an intussusception, the oral portion of gut (intussusceptum) usually is engulfed and propelled distally by peristaltic action of the enveloping portion (intussuscipiens).
Constable and colleagues reported that the prevalence is increased among calves younger than 2 months of age in comparison with adults and in Brown Swiss cows in comparison with Holstein cows.10 The condition has also been reported in goats11 and in sheep.12,13 Intussusception may occur in either the large or the small intestine of calves but is much more frequent in the jejunum.10 Clinical signs include colic caused by the tension on the mesentery on the invaginating portion of the intestine. With time, ischemia of this portion leads to pain and eventually loss of sensation. Distention of the intestine with fluid and gas proximal to the obstruction leads to abdominal pain. Therefore an affected cow may show violent behavior or kicking at the abdomen in the first few hours that is eventually succeeded by treading and repeated lying and standing. Over the course of several days, the intussusceptum may become totally devitalized and slough. This is accompanied by focal peritonitis, and in the event of bowel rupture, diffuse peritonitis and toxic shock develop. The exact cause of intussusception remains unknown. Intramural or luminal mass or lesions, viral enteritis, intestinal parasitism, abrupt dietary changes, administration of intestinal motility modifier drugs, and foreign body or prior surgery have all been reported to be potential predisposing factors, but in most cases, intussusception is idiopathic.10Dehydration develops as gastrointestinal secretions accumulate in the gut lumen. In adults, hypochloremic, hypokalemic metabolic alkalosis develops gradually. The rumen becomes distended with fluid as its contents become more finely digested and abomasal reflux accumulates. The right side of the abdomen (or both sides) also enlarges as a result of the distention of the small intestine. Simultaneous auscultation and percussion of the right side of the abdomen reveal areas of variable-pitched resonance. Rectal examination reveals distended loops of small intestine.
The intussusception may be palpable as a firm mass, painful when palpated. Feces may eventually be absent. The examiner may find mucus and blood in the descending colon.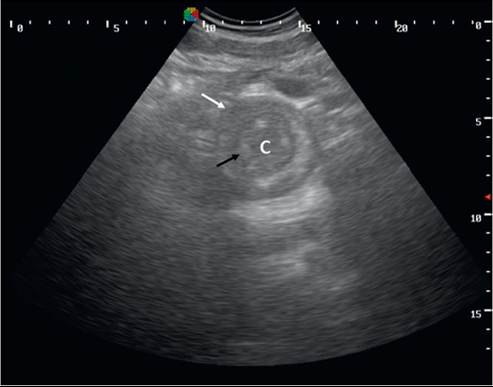
FIG. 32.137 Right abdominal ultrasonography of a cow with an intussusception: intussuscipiens (white arrow), intussusceptum (black arrow), and core (C). (Courtesy Centre Hospitalier Unversitaire Veterinaire de PUniversite de Montreal).
In long-standing cases the scant feces are very dark red and must be distinguished from the black feces (melena) associated with abomasal bleeding. Fluid obtained by abdominocentesis reveals an elevation in erythrocytes and leukocytes counts and an elevated protein concentration. If the condition is longstanding and bowel rupture has occurred, bacteria may be present. CBC may reveal neutrophilia and an elevated plasma fibrinogen level.
In neonates with enteritis, fecal output decreases and appetite is lost when the intussusception develops. A fever may develop as peritonitis occurs. Affected calves and other neonates may not exhibit obvious signs of colic. Percutaneous abdominal palpation with both hands in an attempt to detect a mass is often successful in delineating an intussusception in a neonate. When neutrophilia, hyperfibrinogenemia, and loss of appetite develop after enteritis, intussusception should be suspected.
Findings compatible with an intestinal obstruction are seen on transabdominal ultrasonography (distended intestinal loops, decreased or absent peristalsis). In some cases, the affected intestinal segment may be visualized. At that time, ultrasonographic appearances described as “target-like” or “bull's eye” lesions or as multiple-layered, onion ring-type masses with a “sandwich configuration” are observed in transversal and longitudinal views of the intestine, respectively (Fig. 32.137).14
Treatment requires both surgical correction of the obstruction and parenteral restoration of fluid and electrolyte balance. Because of the losses of chloride and potassium and the development of alkalosis, 0.9% sodium chloride solution with 30 mEq/L or more of added potassium chloride is recommended. Intravenous potassium should not be given more rapidly than 1 mEq/kg/h (conservative rate is 0.5 mEq/kg/h). Once intestinal patency has been restored, oral fluid and electrolyte supplementation usually allows the patient to achieve normal status.
The prognosis is usually good if surgery is performed early in the course of disease. Complications such as peritonitis can occur and need to be treated appropriately to maintain the chance of success. A retrospective study of 336 cases of intussusception demonstrated a postoperative survival rate of 43% and an overall survival rate of 35%.10
Intestinal Incarceration
Intestinal obstruction may occur in ruminants as a result of accidental entrapment of intestinal loops, usually of jejunum, around remnants of embryonic structures or through an acquired defects in mesentery, a ligaments or the abdominal wall. Remnants of the urachus, the omphalomesenteric duct, the left umbilical vein, and the ductus deferens have been described as responsible for incarceration of the jejunum. The authors of one report indicated that 26% of cows examined had a persistent round ligament of the liver and falciform ligament.15 Thus tears in the falciform ligament that lead to intestinal entrapment may be among the most common causes of the relatively rare problem of intestinal incarceration in cattle. Duodenal obstruction caused by malposition of the gallbladder was also reported in a heifer.16 Intestinal adhesions caused by intraperitoneal injections of irritating substances may also lead to intestinal obstruction. Initial signs of colic followed by depression, anorexia, progressive abdominal distention, and absence of feces usually develop. Distended loops of small intestine usually are palpable rectally. Treatment of intestinal incarceration requires surgical intervention.
Cecum Dislocation
Cecum distention may be classified in three ways: (1) In cecal dilation, the cecum is distended only by gas, and the apex of the cecum is displaced toward the rectum and may be palpable transrectally; (2) in cecal retroflexion (which can cause vascular damage and ischemia; i.e., volvulus,: the cecum is distended, displaced, and folded dorsally or ventrally, the apex of the cecum is consequently oriented cranially and is usually not palpable rectally; and (3) in cecal torsion, the cecum is distended and rotated along its long axis, and the apex of the cecum is displaced toward the rectum and can be palpated transrectally.17 In a large study of 461 cases of cecal dilation, the preoperative clinical diagnoses based on rectal palpation were cecal dilation alone in 291 animals (63.2%), cecal dilation and retroflexion in 94 animals (20.4%), and cecal dilation and torsion in 20 animals (4.3%); in the remaining 56 animals, no diagnosis of cecal dilation could be made preoperatively.18 In adult cattle, cecal dilation generally is believed to precede retroflexion or torsion.
The etiologic and pathophysiologic features of cecal dilation and retroflexion or torsion remain unknown. Different feeding or management practices may predispose animals to cecal disease.18 Increased luminal concentration of VFAs was classically believed to play a major role in the etiopathogenesis of cecal disorders. However, results of studies on the effect of VFAs on cecal motility have been contradictory. In one study, increased concentration of VFA had only minimal effect on large intestine motility and was unlikely to play an important role in the development of cecal disorders.19 Factors that affect cecal motility, as described for displaced abomasum, are probably similar.
Cecal dilation produces a more gradual onset of illness than that noted with cecal retroflexion or torsion. The time required for dilation to develop into retroflexion or torsion is unknown. With simple dilation, feed intake and milk production decrease. Mild abdominal pain may be observed. Feces are usually still produced, but the consistency may be loose and the amount reduced. Rumen motility is decreased. Distention of the right paralumbar fossa without the ribs being sprung is frequently observed in the authors' clinic and has been mentioned in different reports. However, Braun and colleagues18 reported that the abdominal shape was modified in only 51 animals of the 461 cattle affected with cecal dilation, retroflexion, or torsion. Of those animals, 22 had a slight distention of the right flank, 20 a bilateral abdominal distention, and 7 a pearshaped abdomen. The most important clinical findings for the diagnosis of cecal dilation are (1) the presence of a large area of resonance (ping), auscultable from the tuber coxae to a variable distance cranially (see Chapter 1), which may or may not be associated with a positive succussion of the right flank18;
and (2) the transrectal palpation in the pelvic canal or nearby of the apex of the gas-filled cecum. Cattle with cecal retroflexion or torsion have more severe clinical signs. They show an abrupt onset of anorexia, agalactia, and severe abdominal pain. Tachycardia and forestomach stasis are also present. Feces are scant or absent. The abdominal distention is usually more severe than in simple cecal dilation. The area of resonance in the right paralumbar fossa is larger, and fluid usually can be detected in the cecum and proximal colon by succussion. In cases of retroflexion, the apex of the cecum is usually not palpable rectally; rather, the distended body of the cecum or proximal colon impinges on the pelvic canal because the apex is directed cranially. In cases of cecal torsion, the apex of the cecum can be palpated rectally as well as a tense ileocecocolic ligament that spirals around the cecum.17 Distention of the small intestine may be palpated with either dilation or retroflexion or torsion.
Although some cows with simple dilation have no acid-base abnormalities, most cases of cecal retroflexion are accompanied by some degree of metabolic alkalosis with hypochloremia and hypokalemia. Hypocalcemia is reported to be observed in approximately 85% of cases of cecal dilation, retroflexion, or torsion.18
Medical management of cecal dilation is usually successful with fluid therapy to restore normal hydration status and correction of electrolyte abnormalities, including hypocalcemia. Administration of NSAIDs to control abdominal pain is also important. Laxatives have also been recommended for the medical treatment of cecal dilation. However, Braun and coworkers20 reported that the use of laxatives (liquid paraffin) for the treatment of cecal disorders delayed the time to first defecation. Moreover, magnesium hydroxide may be responsible for detrimental effects such as metabolic alkalosis,21 increased ruminal pH,22 and decreased ruminal microbial activity.22 Prokinetic drugs that can be used in the management of cecal disorders are presented in the section on the acute abdomen in cattle. Affected animals should be fed a high-fiber diet.
Braun and colleagues18 reported that 122 of 461 animals with cecal dilation, retroflexion, or torsion were first managed medically. Of these 122 animals, 42 eventually required surgery. Considerations for medical versus surgical treatments are presented in the Acute Abdomen in Ruminants section. Cattle with cecal retroflexion or torsion require immediate surgical intervention, IV fluid, and pain management (NSAIDs). The prognosis for surgical patients depends on the degree of ischemic injury to the cecum and other structures involved in the obstruction. The recurrence rates after surgery range from 10% to 13.8% within a year of the first incident.18 In cattle with recurrence of cecal dilation or with devitalized portion of the cecum wall, amputation of the cecum is recommended.
Intestinal Tumors
Intestinal tumors are rare in cattle. The most commonly reported intestinal tumors in cattle are adenocarcinomas. However, lymphosarcoma, adenoma, adenomatous polyps, carcinoid, leiomyoma, leiomyosarcoma, and fibrosarcoma have also been described.23 The incidence of adenocarcinoma in sheep is relatively high in some areas of the world, such as New Zealand.24 The predisposing factors for adenocarcinomas are not known, but different environmental carcinogens have been suspected.24,25 In sheep, no association with infectious agents (herpesviruses, Helicobacter spp., or Mycobacterium avium subsp. paratuberculosis) was found.24 Genetic predisposition is suspected,25 but no significant genetic defects were found in 24
one study.24
Affected cattle or sheep may have a protracted course of weight loss with no other observable signs until near death. Alternatively, there are reports of acute gastrointestinal disturbances manifested by colic, abdominal distention, and auscultable right-sided pings.26 Although these cases are rare, they must be differentiated from other causes of acute obstruction in cattle such as cecal volvulus, intussusception, or abomasal volvulus. In cattle in which rectal examination is possible, the lesion may be detected on routine examination as an intramural mass or annular constriction of the jejunum or ileum. In sheep, the diagnosis is usually made at necropsy. Clinical signs in affected animals might include diarrhea, abdominal distention caused by the accumulation of gas and ingesta proximal to the obstruction, or ascites. The well-characterized lesions in sheep involve local spread of the tumor through the lymphatic system and intraperitoneally. Ultimately, cellular deposits occur on all visceral and parietal peritoneal surfaces, severely impairing lymphatic drainage from the abdomen.
Mesenteric Fat Necrosis
Mesenteric fat necrosis affects cattle of all breeds, but more commonly Aberdeen Angus and Jersey cattle.27 It has also been reported in a pigmy goat.28 The cause remains unknown but dietary factors have been implicated, such as consumption of feed containing long-chain, saturated fatty acids; trace element deficiency; trauma; hormonal disturbance; and ingestion of endophyte-infected fescue.27,28 The lesions develop as an inflammatory response around degenerating adipose cells. The triglycerides in these cells are thought to undergo hydrolysis to glycerol and fatty acids. Fatty acids with longer carbon skeleton have greater degree of saturation and are more resistant to removal by normal cellular mechanisms. Remaining clumps or crystals of fatty acids serve as inflammatory foci for the subsequent necrotic masses.27 Affected cattle have subnormal serum levels of free cholesterol and elevated serum levels of free fatty acids.29 Cattle with fat necrosis may eventually develop an intestinal obstruction. The clinical signs resemble those of progressive intestinal obstruction from other causes. Weight loss, anorexia, diarrhea, bloody stool, abdominal enlargement, and right-sided ping are all possible signs. Fever, tachycardia, and signs of discomfort such as tenesmus, treading, and teeth grinding may be seen as the obstruction becomes more severe. Many affected cattle have no clinical signs, and the condition is discovered during rectal examination for other reasons. Rectal examination may be impossible because of stricture of the rectum, or dystocia may occur as a result of the necrotic fat masses in the pelvic canal. Fat necrosis usually affects mature cattle,27 but there is a report of a 6-month course of illness attributed to fat necrosis in a 13-month-old Black Angus heifer.30 Ultrasonographic appearance of abdominal fat necrosis has been described and appears to be a useful diagnostic tool, combined (or not) with ultrasonography-guided mass biopsy.31
Animals with fat necrosis that becomes clinical usually are not treated. Different treatments have been attempted over the years, but none was considered effective. Experimental therapy of subclinical fat necrosis with a compound that alters lipid metabolism in fungi was successful in one study.29 The fungicide isoprothiolane was given at a dosage of 20 g/day PO for 8 weeks. Approximately half of the treated cows had a 50% reduction in necrotic masses by 12 weeks; at follow-up evaluation in 1 year, the masses were not detectable in half the surviving cows. Cows given such unapproved drugs should not be used for food.
Hemorrhagic Bowel Syndrome (Jejunal Hemorrhage Syndrome)
Hemorrhagic bowel syndrome, also called jejunal hemorrhage syndrome, is an acute enteric disease of cattle characterized by segmental intraluminal hemorrhage with subsequent obstruction of the small intestine. The disease seems to have been described for the first time in 199132 and is now reported in different countries. Hemorrhagic bowel syndrome affects mainly dairy cows, but it is also reported in beef cows and bulls.33,34 It is principally a sporadic disease, but outbreaks in dairy herds have been reported.35,36
The pathogenesis, causes, and clinical presentation of hemorrhagic bowel syndrome is presented in the Diseases Caused by Clostridium perfringens Toxins (Yellow Lamb Disease, Lamb Dysentery, Necrotic Enteritis, Enterotoxemia) section.
The prognosis for animals with hemorrhagic bowel syndrome is guarded. Mortality rates of 100%33 and 77%37 have been described. However, prognosis of 55% (20 of 36)34 and 58% (18 of 31)38 have been reported from two referral centers. In the first study, two animals of five that were treated medically and 18 animals of 30 treated surgically survived.34 In the other study, all dairy cows underwent surgery; among the 18 animals that survived, 6 had a recurrence within the following 12 months and 13 were still alive after 12 months. In this study, short-term prognosis was reported to be significantly improved when the blood clot could be dislodged by massage.38
Functional Ileus (Pseudoobstruction)
Failure to pass feces usually is a sign of intestinal obstruction. However, in adult lactating dairy cattle, a condition of functional ileus (or pseudoobstruction) of the intestinal tract that mimics complete intestinal obstruction is commonly observed. The condition resolves with medical treatment (fluids, calcium, and pain management); in rare instances, surgical decompression of the affected bowel is required. Affected cows are most often in early lactation, and treatment is sought for partial anorexia. Colic sometimes is the presenting sign. Clinical examination reveals a normal temperature, a normal to elevated heart rate, and normal respiratory rate. Ruminal motility is decreased. Slight right-sided abdominal enlargement may be seen early and may progress to extreme distention of the abdomen on the right. No borborygmi is heard on the right side, but fluid tinkling sounds may be audible. Simultaneous auscultation and percussion reveal areas of variable-pitched resonance. Succussion produces sloshing sounds. On transrectal examination a distended spiral colon, cecum, or small intestine may be palpated. Early in the course of the disease, the distention is mild, and compression easily flattens the affected bowel. If abdominal distention is severe, introducing the arm into the abdominal cavity may be difficult because of the pressure of distended bowel at the pelvic inlet. No feces are passed, but the examiner’s arm may be coated with sticky mucus and feces with a stale odor. Serum electrolytes and acid-base status are usually normal or toward a mild metabolica alkalosis. Serum calcium may be decreased. Differential diagnoses to consider include intussusception, intestinal incarceration, intestinal volvulus, and cecal dilation. There is no blood in the feces, and no masses are palpable rectally with functional ileus.
Because most obstructive lesions of the intestine in cattle are not immediately life-threatening, symptomatic therapy combined with close observation may be elected for 24 hours. If surgery is necessary in the absence of an obstructive lesion, the bowel may be decompressed and drained. This is a laborious procedure that requires multiple punctures unless the distention is restricted to the cecum and spiral colon. Despite the lack of correction of a specific underlying defect, many affected cows pass feces soon after an exploratory celiotomy. Manipulation of the intestinal tract alone seems to have beneficial effects. This response is difficult to differentiate from the spontaneous recovery that may occur without surgery in cows. Moreover, medical treatment (IV fluids and pain control medication) is commonly provided during surgery, which makes it difficult to assess the effect of surgery alone. Relief of distention of portions of the intestinal tract may remove reflex inhibition of motility that can occur in response to extreme stretching of mural tension and pain receptors. The cause of functional ileus of the intestine is unknown, and little pathophysiologic information has been elucidated. Medical management is
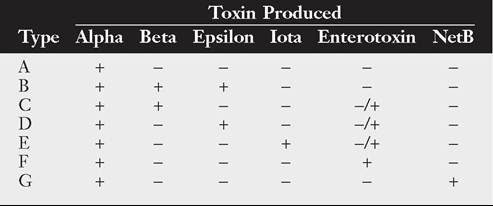
■ TABLE 32.22
New Toxinotyping System for Clostridium perfringens1
described in detail in the Acute Abdomen in Ruminants section. It mainly includes administration of fluids, calcium, and NSAIDs. Numerous practitioners also administer oral laxatives, but as mentioned earlier, the practice of using magnesium salts may be questionable and could have deleterious effects.