ORAL MALIGNANT MELANOMA IN DOGS
Background
Melanoma is the most common oral malignancy found in the dog. Unlike cutaneous melanomas, which are often benign, melanomas of the oral cavity in dogs are very aggressive and commonly metastasize to local lymph nodes and lungs.
Oral melanomas are often poorly responsive to conventional therapy. Although some oral melanomas may appear histologically benign, these tumors may behave very aggressively. Oral malignant melanomas are most common in poodles, dachshunds, Scottish terriers, golden retrievers, standard and miniature schnauzers, Doberman pinschers, and Irish and Gordon setters.In three studies totaling 193 dogs with oral melanoma, there were 94 male and 99 female dogs.This is a disease of old dogs. In one study the median age of affected dogs was 11 years; ages ranged from 4 to 16 years.
Clinical Parameters
Most oral melanomas originate in the gingiva, but these tumors can also arise from the palatine, labial, and buccal mucosa.
Clients may present dogs for an oral mass or more frequently for persistent halitosis, bleeding from the mouth, and (occasionally) dysphagia. Tumors may be quite large, ranging in volume up to 64 cm3 in one study. Although masses are frequently pigmented, amelanotic tumors can occur. Oral melanomas are friable and invasive within the soft tissues of the mouth.
Clinical Work-up
Dogs with oral tumors of any type should be staged using blood work, radiographs of the lesion, a metastasis evaluation of the thorax, and cytologic or histopathologic examination of the lesion and regional lymph nodes. The metastatic rate is very high for oral melanoma, but the time to metastasis varies. At diagnosis, fine-needle aspiration of the mandibular lymph nodes (both ipsilateral and contralateral), as well as any enlarged node, should be performed for cytologic examination. It is important to remember that nodes that are palpably within normal parameters can still demonstrate metastatic disease.The surgical approach for lymph node evaluation has been previously published.
In one study, only 5 (12%) of 41 dogs had metastatic disease in regional lymph nodes at the time of diagnosis. Aspiration cytologic findings that are suspicious should be confirmed by surgical biopsy. Thoracic radiographs may indicate pulmonary metastasis at the time of diagnosis. Pulmonary metastasis, however, frequently occurs late in the course of the disease or may be a micrometastasis at the time of diagnosis and therefore undetectable by radiography. In one study, only 3 (7%) of 41 dogs had evidence of pulmonary metastasis at diagnosis, but at the time of death, metastatic rate for this tumor approximated 80%. Melanoma may also spread systemically, and metastasis has been reported to kidney, myocardium, brain, and other sites.Metastasis due to melanoma probably occurs early in the course of this disease (during clinical stages I and II, indicating small, localized disease); however, metastases are often not detected until long after the primary melanoma is resected. The growth rate of metastases may vary, and it is this variation, rather than the time that metastasis occurs, that determines survival time.
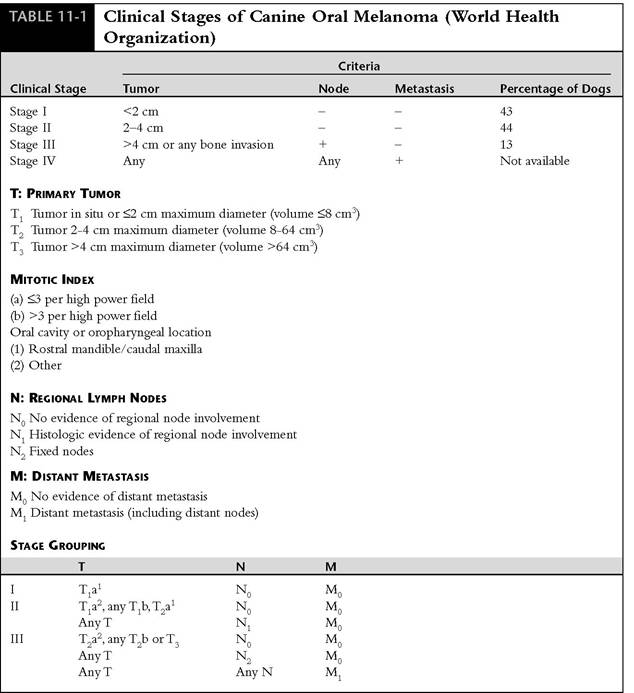
Some investigators have found that the World Health Organization (WHO) staging system provides prognostic information, but an alternative staging system has been proposed that includes the WHO criteria and also uses the mitotic index from histopathologic results and location within the oral cavity. This staging system also offers prognostic information.
Current recommendations for staging oral melanoma therefore include a complete blood count, biochemical profile, urinalysis, lymph node evaluation by cytologic examination or biopsy, thoracic radiographs, and tumor measurements, as well as anatomic location and evaluation of mitotic index as determined by histopathologic findings.
Prognostic Factors
Some studies have demonstrated significantly longer survival for dogs with stage I (small) tumors (median, 511 days) than for dogs with stage II or III tumors (median, 164 days) (Table 11-1).
Small melanomas were also associated with longer survival times in another study.One study found that the location of the tumor was not prognostic, but two other studies indicated that tumors of the rostral mandible and the caudal maxilla had longer remissions and survival after surgery. Another study found longer survival times for dogs with tumors that had fewer than three mitotic figures per high-power field.
Therapeutic Approach
Surgery is the treatment of choice for oral melanoma and should consist of mandibulectomy or maxillec- tomy. Radiation has a role in local tumor control. Chemotherapy with platinum compounds, perhaps combined with liposome-encapsulated muramyl- tripeptide-phosphatidylethanolamine (L-MTP-PE, not yet commercially available) immunotherapy, may offer the best adjunctive treatment for metastatic disease.
Although metastatic rate with oral melanoma is high, metastases frequently are not observed until late in the course of disease, occasionally more than 1 year after local therapy. Most dogs therefore are euthanized because of progression or recurrence of local disease. Surgery should be aggressive from the outset; it may prolong survival and provide palliation. Aggressive local therapy should include resection of underlying bone. In one early study 34 of 49 dogs had local recurrence of tumor, and 33 dogs developed metastases. The recurrence rate of 84% probably reflects the less aggressive nature of the surgery, because more recent studies reported local recurrence rates of less than 15% for melanomas treated by mandibulectomy to 48% for tumors treated by maxillectomy. Both mandibulec- tomy and maxillectomy are tolerated well by dogs, with median hospitalization times ranging from
2 days for simple excision to 8 days for total hemi- mandibulectomy. Eighty-five percent of owners in one study who decided to treat their dogs with mandibulectomy or maxillectomy were very satisfied with the outcome. In three studies, dogs treated with aggressive surgery had a median survival time of 7.3 to 9.1 months, compared with seven dogs that did not have surgery and survived a median of 2 months.
Mandibulectomy or maxillectomy should be the first surgery used to treat oral melanoma in dogs. Less aggressive surgeries do not prolong survival and make subsequent surgery more difficult.Surgical excision was used to treat five dogs with melanoma of the tongue and achieved local control in three dogs, with survival times ranging from
3 months to 45 months (median, 19 months). Only one dog developed metastases.
Within 6 months of surgery the majority of patients will have developed metastatic disease. However, metastases may not be visible for longer than 1 year after surgery. After metastases develop, dogs may still survive for an extended period of time, depending on the growth rate. Dogs may tolerate pulmonary metastatic disease with very little apparent effect on their quality of life.
Radiation therapy has been used and certainly has a role in the treatment of melanoma, particularly for small tumors. In one study 33 dogs with melanoma were treated with 48 Gy of 60Co teletherapy. Five dogs had local recurrence. One dog had regional lymph node metastasis, and 14 developed distant metastasis. Dogs with rostrally located tumors and dogs with smaller tumors had longer remissions. Median progression-free survival was estimated to be 14 months. In another study, dogs were treated with 48 Gy over 4 weeks on an alternate-day schedule with 4-Gy fractions. In 8% of the dogs, severe acute reactions were recognized (tumors other than melanoma were also included). After completion of radiation, dogs with malignant melanoma in this study were 2.6 times
more likely than dogs with squamous cell carcinoma to develop tumor progression. Dogs with larger or more invasive tumors had a worse prognosis. In another study 36 dogs with oral melanomas were treated with 36 Gy given in four fractions of 9 Gy at 7-day intervals. In 25 of the 36 dogs, complete remission was achieved and median survival for these dogs was 37 weeks.
None of the dogs in this study suffered severe acute effects, and most died of metastatic disease. Local control of oral melanoma (53% complete response) has been achieved with coarse fractionation using three 8-Gy fractions.A review of the literature would lead to the conclusion that chemotherapy has demonstrated very little effect on survival times in dogs with oral melanoma. Drugs such as dacarbazine (DTIC) (1000 mg/m2 intravenously every 3 weeks), doxorubicin (30 mg/m2 intravenously every 3 weeks), and melphalan (0.23 mg/lb intravenously every 4 weeks) have not had repeatable success. Platinum compounds may be more efficacious; cisplatin (60 mg/m2 intravenously every 3 weeks) provided partial response for a dog with metastatic disease, and carboplatin (300 mg/m2 intravenously every 3 weeks) appears to have some efficacy, although the response rate is still probably less than 30%. Intralesional chemotherapy with cisplatin in purified bovine collagen matrix material has been used successfully to treat oral melanomas. Dogs were treated with an average of 20 mg of cisplatin delivered over an average of 5.2 treatments. Dogs with complete responses had a mean survival of 54 weeks, whereas those having a partial response had a mean survival of 14 weeks.
Immunotherapy has a role in treating melanoma in many species. Cimetidine, which appears to have an immunomodulating effect by inhibition of suppressor T cells, has been shown to cause regression of melanoma in some horses, although its role in the treatment of the disease in dogs is not defined. Immunotherapy with interleukin-2 has been beneficial in treating humans with melanoma. Combined with tumor necrosis factor, this treatment might be useful for dogs. This combination was administered to 13 dogs with measurable oral melanoma. Five dogs showed reduction in tumor size, although only two had durable responses. One of these dogs had a complete remission for more than 3 years.
Immunotherapy with heat-inactivated Coryne- bacterium parvum (0.045 mg/lb intravenously per week) was used as an adjunct to surgery in 42 dogs. C. parvum activates and increases production of macrophages, which enhances the antibody response. Improved survival over surgery alone has been reported when oral melanoma was treated with a combination of surgery and C. parvum. Immunotherapy with C. parvum was found to benefit dogs with small tumors (stage I). L-MTP-PE, a more specific macrophage activator, improves survival in dogs treated after surgery for oral melanoma, with a median survival of 346 days. L-MTP-PE was administered to 24 dogs after surgery, and 26 dogs received a placebo. Only 8 (33%) of the L-MTP-PE dogs had died at an interim analysis, whereas 14 (54%) of the placebo group had died.
Granulocyte-macrophage colony-stimulating factor (GM-CSF) transfected vaccines using autologous tumor cells have been used in dogs with melanoma. Direct intratumoral injection of GTM- CSG plasmid DNA induced partial or complete tumor regression and prolonged survival times compared with historical controls.
More on the topic ORAL MALIGNANT MELANOMA IN DOGS:
- References
- Tams T.. Handbook of Small Animal Gastroenterology. Saunders,2003. — 496 p., 2003
- PLACENTAL MAMMALS
- Neoplastic Disease