Parathyroid Gland, Calcium, and Phosphorus Regulation in Horses
Ramiro E. Toribio
Calcium
Calcium is the fifth most abundant element in the body, representing ≈1.5% of the body weight. Physiologic functions such as signal transduction, muscle contraction, hormone secretion, enzyme activation, gene transcription, cell division, cell membrane stability, cell migration, neuromuscular excitability, and blood coagulation are calcium dependent.1-3 Processes that result in cell injury and death, such as free radical production, cytokine release, protease activation, excitotoxicity, vasoconstriction, and apoptosis, also require calcium.2,3
Calcium has structural and nonstructural functions, and it is found in three main compartments: the skeleton, soft tissues, and the extracellular fluid.
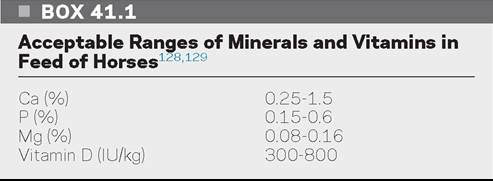
Approximately 99% of the total body calcium (and 85% of phosphorus) is in the skeleton as hydroxyapatite (Ca10[PO4]6[OH]2) in a calcium-to-phosphorus ratio of 2 : 1. As part of the skeleton, calcium provides support against gravity, protects vital internal organs, and houses blood-forming elements. The skeleton is also a reservoir for calcium. Nonstructural functions are related to calcium as a regulatory ion. The remaining calcium is present in the cell membrane, mitochondria, endoplasmic reticulum, and extracellular fluid.1-3 In blood, most calcium is in plasma as a free or ionized form (≈55%), bound to proteins (≈40%), and complexed to anions such as citrate, bicarbonate, phosphate, and lactate (≈5%) (Fig. 41.15).1-4 In adult horses, serum ionized calcium represents 50% to 55% of the total serum calcium, while in foals ionized calcium is 43% to 56% of the total serum calcium.2-8 Free, unbound, or ionized calcium (Ca2+) is the biologically active form of calcium. Of the protein-bound calcium, approximately 80% is associated with albumin and 20% with globulins. Calcium binds to negatively charged or anionic proteins, and this affinity is pH dependent. During acidosis, increased H+ concentrations decrease Ca2+ binding to anions, resulting in increased plasma Ca2+ concentrations. Alkalosis lowers Ca2+ concentrations. Hypoalbuminemia results in total hypocalcemia (pseudohypocalcemia), with Ca2+ concentrations remaining within the normal range.Calcium and phosphorus requirements in horses depend on age, physiologic status, and amount of work or exercise performed (Table 41.2). Serum Ca2+ concentrations are not a reliable indicator of dietary calcium intake. A balanced diet for horses must have 0.15% to 1.5% of calcium and 0.15% to 0.6% of phosphorus in feed DM (Box 41.1). A
Distribution of Calcium in the Body
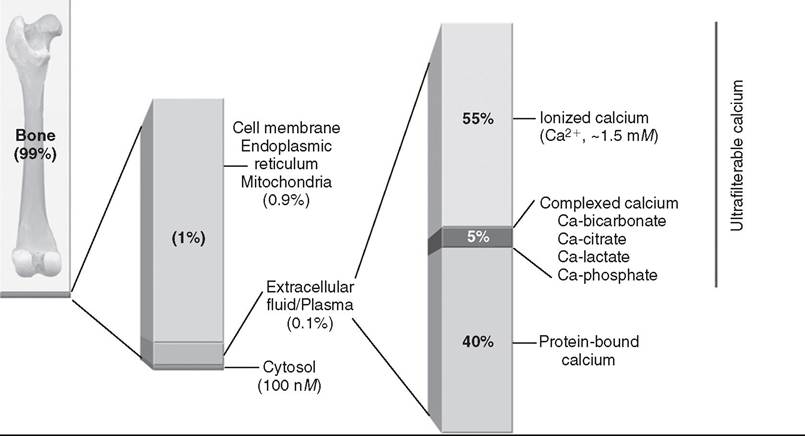
FIG. 41.15 Calcium distribution in the body. Approximately 99% of the total body calcium is in the skeleton. The remaining calcium is present in the cell membrane, mitochondria, endoplasmic reticulum, and extracellular fluid. In blood, calcium exists in a free or ionized form (Ca2+), bound to proteins, and complexed to anions such as citrate, bicarbonate, phosphate, and lactate. In horses, serum Ca2+ represents 50% to 55% of the total serum calcium concentration.
■ TABLE 41.2
■ TABLE 41.4
Calcium and Phosphorous Requirements in the Horse
| Percent in Diet | Daily Intake (Grams) | |||
| Ca | P | Ca | P | |
| Foals (bgcolor=white>0.29 | ||||
| Orchard grass | 0.25 | 0.39 | 0.31 | |
| Barley | 0.05 | 0.37 | 0.15 | |
| Corn | 0.05 | 0.60 | 0.03 | |
| Oats | 0.09 | 0.38 | 0.16 | |
| Wheat | 0.05 | 0.42 | 0.14 | |
| Cottonseed meal | 0.18 | 1.22 | 0.59 | |
| Linseed | 0.43 | 0.90 | 0.67 | |
| Skim milk | 1.36 | 1.09 | 0.13 | |
| Soybean meal | 0.40 | 0.71 | 0.31 | |
| Molasses, cane | 1.10 | 0.15 | 0.47 | |
| Wheat bran | 0.14 | 1.27 | 0.63 | |
Modified from NRC: Nutrient requirements, feedstuff composition, and other tables.
In National Research Council (U.S.), Committee on Nutrient Requirements of Horses, editors: Nutrient requirements of horses, Washington, D.C., 2007, National Academies Press, pp 293-310.
| Common Name | Scientific Name |
| Bermudagrass | Cynodon dactylon |
| Buffel grass | Cenchrus cilaris |
| Dallis grass | Paspalum spp. |
| Elephant grass | Panicum spp. |
| Foxtail grass | Setaria spp. |
| Greasewood | Sarcobatus Vermiculatus |
| Halogeton | Halogeton glomeratus |
| Kikuyu | Pennisetum clandestinum |
| Kochia, summer cypress | Kochia scoparia |
| Lamb’s quarters | Chenopodium spp. |
| Napier, mission grass | Pennisetum spp. |
| Pangola | Digitaria decumbens |
| Panic | Panicum spp. |
| Para grass | Brachiaria spp. |
| Pokeberry | Phytolacca americana |
| Purple pigeon grass | Setaria incrassate |
| Purslane | Portulaca oleraceae |
| Red-rooted pigweed | Amaranthus spp. |
| Rhubarb | Rheum rhaponticum |
| Russian thistle, tumbleweed | Salsola spp. |
| Setaria | Setaria sphacelata |
| Sorrel | Rumex spp. |
| Soursob, shamrock | Oxalis spp. |
| Sugar beet | Beta vulgaris |
aThese plants have an oxalate content higher than 0.5% of dry matter or a calcium-to-oxalate ratio of less than 0.5.
decrease intestinal absorption of calcium, decrease bone resorption, and increase urinary excretion of Ca2+ in horses.20,21
Calcium is eliminated through feces, urine, milk, sweat, and the fetus. In the kidney, approximately 60% calcium is reabsorbed in the proximal tubules by passive mechanisms and 35% is reabsorbed in the thick ascending loop of Henle and distal tubules by active mechanisms.22 The rest (≈5%) represents the urinary fractional excretion of calcium. Endogenous losses of calcium in horses have been estimated around 20 to 25 mg/kg/body weight/day. Assuming a 50% calcium digestibility, a 500-kg horse would require 20 g of calcium to replace losses, or 40 mg/kg/day; growing and lactating horses can double these requirements. Interpretation of the urinary excretion of calcium could be difficult because horses eliminate large amounts of calcium (primarily calcium carbonate) in urine.2,3,23
Phosphorus
Phosphorus represents ≈1% of body weight, with most (85%) located in the skeleton as hydroxyapatite crystals, 15% in blood and soft tissues, and less than 0.1% in the extracellular fluid. In blood, phosphorus exists as organic (intracellular) and inorganic (extracellular) phosphates. Organic phosphate consists of phosphate esters (phospholipids) bound to proteins and blood cells and represents most of the phosphorus in circulation; however, only inorganic phosphate (PO4) is measured. PO4 is found as ionized phosphate (≈50%), complexed with cations (Na+, Ca2+, Mg2+; ≈35%), and bound to proteins (≈15%). At pH 7.4, PO4 exists as divalent (HPO42-) and monovalent (H2PO4-) anions in a 4:1 ratio. In acidosis this ratio is 1:1 and can be as high as 9:1 during alkalosis.24 In soft tissues, most of the phosphate is organic and intracellular.
It is incorporated into nucleic acids, phospholipids, and energy compounds such as ATP and creatine phosphate. Thus, phosphate is important for muscle contraction; neurologic functions; enzyme activity; electrolyte transport; oxygen transport (2,3 DPG); intermediary metabolism of proteins, carbohydrates, and fats; gene transcription; and cell proliferation and differentiation. PO4 regulation is closely associated to Ca2+ homeostasis.Phosphorus requirements depend on age, physiologic status, and amount of work or exercise performed (Table 41.2). In horses, phosphorus absorption ranges from 20% to 55% and occurs in the small and large intestines.17,25 Excess dietary aluminum may reduce PO4 absorption26-28; however, magnesium does not seem to interfere with PO4 absorption in horses.29 In the kidneys, most of the PO4 is reabsorbed in the proximal tubules by a Na+-dependent mechanism and the urinary fractional excretion of PO4 in horses is low (is a common cause of hypophosphatemia in critically ill humans and small animals and occasionally occurs in horses with starvation, refeeding syndrome, and parenteral nutrition (hyperglycemia, hyperinsulinemia).
Chronic phosphate deficiency can be manifested as weight loss, weakness, pica (depraved appetite), lameness, and developmental orthopedic disease (DOD). Rickets, as described in other species with PO4 or vitamin D deficiency, is not a recognized condition in foals. Serum PO4 concentration is more indicative of dietary phosphorus intake and status than serum Ca2+ because PO4 homeostasis is not as precise as that of Ca2+.
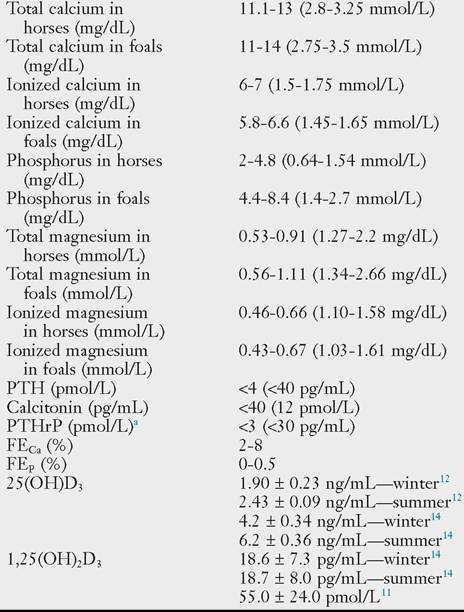
Normal calcium, magnesium, phosphorus, and regulatory hormone concentrations are presented in Table 41.6. Ionized calcium concentrations are lower in foals and pregnant mares
■ TABLE 41.6
Normal Calcium, Magnesium, Phosphorous, and Regulatory Hormone Concentrations in Horses
aMeasured in ethylenediaminetetraacetic acid (EDTA) plasma.
FEca, Urinary fractional excretion of calcium; FEp urinary fraction excretion of phosphorus; PTH, parathyroid hormone; PTHrP, parathyroid hormone-related protein.
Conversion units: Calcium (mmol/L = mg/dL ? 0.25; mg/dL = mmol/L ? 4); magnesium (mmol/L = mg/dL ? 0.4; mg/dL = mmol/L ? 2.43); phosphorus (mmol/L = mg/dL ? 0.323; mg/dL = mmol/L ? 3.1)
Data from the College of Veterinary Medicine, Ohio State University, unless otherwise noted. Foal calcium and magnesium data from recent publications.5,6
than adult horses.5,6,23 Of interest, serum total and ionized magnesium concentrations tend to be higher in foals than adult horses.5,6,23 Serum PO4 concentrations and alkaline phosphatase activity are greater in foals compared with adult horses due to growth, increased intestinal absorption, bone osteoblastic activity, and bone formation.2,6
Calcium and Phosphorus Homeostasis
Extracellular ionized calcium (Ca2+) concentrations are regulated by a homeostatic system that includes three hormones: parathyroid hormone (PTH), calcitonin, and 1,25-dihydroxyvitamin D3 (1,25[OH]2D3, calcitriol); three body systems (kidney, intestine, and bone); and a calcium-sensing receptor (CaR).2,3,23 PTH increases during hypocalcemia and hyperphosphatemia while calcitonin increases during hypercalcemia (Fig. 41.16). Under physiologic conditions parathyroid hormone-related protein (PTHrP), which also activates the PTH-1 receptor, has little effect on Ca2+ homeostasis.31 PO4 regulation is closely associated with Ca2+ homeostasis. Extracellular ionized magnesium (Mg2+) has permissive effects on calcium homeostasis by facilitating PTH secretion and action.
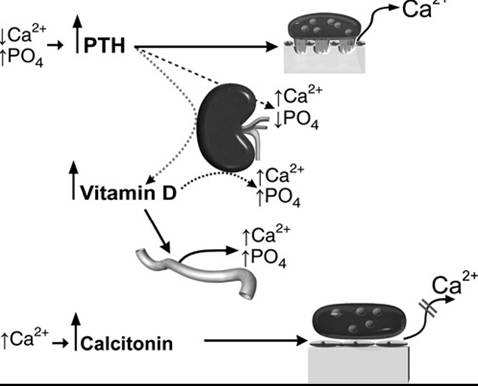
FIG. 41.16 Calcium and phosphate homeostasis. A decrease in serum Ca2+ or increase in serum PO4 concentrations increases PTH secretion. PTH increases renal Ca2+ reabsorption and vitamin D synthesis, decreases renal PO4 reabsorption, and increases osteoclastic bone resorption. In turn, vitamin D increases intestinal absorption and renal reabsorption of Ca2+ and PO4 and facilitates bone resorption. On the contrary, hypercalcemia decreases PTH secretion and stimulates calcitonin secretion to inhibit osteoclastic bone resorption.
Organs involved in PO4 homeostasis include the intestine (absorption), kidneys (excretion), and bone (storage). Extracellular PO4 concentrations are under the control of various endocrine factors including PTH, 1,25(OH)2D3, calcitonin, insulin, and the fibroblast growth factor-23 (FGF-23)/klotho axis.3 In healthy animals, endocrine control of intestinal absorption of PO4 is minimal, but hormones such as 1,25(OH)2D3 can increase absorption in PO4-deficient states. PTH and the FGF-23/klotho axis are considered the main regulators of PO4 concentrations.32-34 Information on phosphatonins (FGF-23), which inhibit renal PO4 reabsorption and 1,25(OH)2D3 synthesis in a number of species,32-35 is limited in the horse.30
PTH is secreted by the chief cells of the parathyroid gland in response to hypocalcemia and hyperphosphatemia. Parathyroid chief cells detect changes in Ca2+ concentrations by a calcium-sensing receptor (CaR).16,36 Through the PTH receptor, PTH increases renal Ca2+ reabsorption (distal nephron), decreases renal PO4 reabsorption (proximal tubules), stimulates renal calcitriol synthesis (proximal tubules), and stimulates osteoclastic bone resorption (see Fig. 41.16). Calcitriol (1,25[OH]2D3) increases intestinal absorption and renal reabsorption of Ca2+ and PO4 and inhibits PTH synthesis and secretion.2,3 PTH secretion is under the influence of Ca2+, PO4, and vitamin D. Biologically active intact PTH is measured with immunometric assays.
Vitamin D plays an important role in Ca2+ and PO4 homeostasis and, to a lesser extent, in magnesium metabolism. Vitamin D2 (ergocalciferol) and vitamin D3 (cholecalciferol) are secosterols derived from photolytic cleavage of the B rings of ergosterol (plants and yeasts) and 7-dehydrocholesterol (animals), respectively. Vitamin D3 is transported to the liver by a vitamin D-binding protein (GC-globulin), where it is hydroxylated (25-hydroxylase) to 2 5-hydr oxyvitamin D3 (25[OH]D3, calcidiol), which is then transported to the kidney to produce the active metabolite, 1,25(OH)2D3 (calcitriol), by 1α-hydroxylase. In mammalians, 25(OH)D3 is considered the main circulating form of vitamin D. However, recent studies found that 25(OH)D2 was the main vitamin D metabolite in equine blood.37,38 Hypocalcemia, hypophosphatemia, and PTH stimulate 1,25(OH)2D3 synthesis by inducing renal 1α-hydroxylase activity, whereas hypercalcemia, hyperphosphatemia, FGF-23, and 1,25(OH)2D3 inhibit 1α-hydroxylase.
Vitamin D stimulates intestinal absorption and renal reabsorption of Ca2+ and PO4 and, to a lesser extent, of Mg2+. 1,25(OH)2D3 increases the expression and activity of proteins important for transcellular Ca2+ transport, including epithelial Ca2+ channels, Ca2+ binding proteins (calbindin D9k, calbindin D28k), Na+∕Ca2+ exchangers, and Ca2+-ATPases.2,3,39 The effects of 1,25(OH)2D3 on intestinal absorption and renal reabsorption of PO4 are mediated by Na+∕PO4 cotransporters.3 In addition, 1,25(OH)2D3 increases Mg2+ renal reabsorption.40 In bone, 1,25(OH)2D3 increases bone matrix synthesis and mineralization and stimulates osteoclastic activity and bone resorption. In the parathyroid gland, 1,25(OH)2D3 inhibits chief cell proliferation, PTH synthesis, and secretion.41 Vitamin D deficiency results in rickets in young animals and osteomalacia in adults; however, the existence of rickets in the horse is not well documented.
Calcitonin is a 32-amino acid peptide secreted by the parafollicular cells (C cells) of the thyroid gland in response to hypercalcemia in a number of species, including the horse.39,42 Calcitonin inhibits osteoclast function and bone resorption, and it decreases renal reabsorption of Ca2+ and PO4 in most 23
species.2,3
Parathyroid hormone-related protein (PTHrP) is produced by almost every tissue in the body and has a broad range of functions that have little to do with Ca2+ homeostasis.31 Under physiologic conditions, PTHrP functions (morphogenesis, cell differentiation) are considered to be paracrine, autocrine, and intracrine. For the most part, the endocrine functions of PTHrP are considered pathologic (humoral hypercalcemia of malignancy; HHM). HHM is a paraneoplastic syndrome that results from excessive secretion of PTHrP by some tumors. By interacting with PTH receptors, PTHrP promotes bone resorption and inhibits renal Ca2+ excretion, causing hypercalcemia in humans and domestic animals, including the horse.43-48
The FGF-23/klotho axis plays central functions in calcium, phosphorus, and vitamin D regulation. FGF-23 is considered the main PO4-regulating hormone and is secreted by osteocytes in response to 1,25(OH)2D and PTH.49-51 It promotes renal PO4 excretion by decreasing renal Na+/PO4 cotransporter numbers and suppressing 1α-hydroxylase activity, therefore reducing 1,25(OH)2D3 synthesis.49,51-54 FGF-23 also inhibits PTH synthesis and secretion.49,51-54 Klotho is a protein that functions as a coreceptor for FGF-23 in the kidney and parathyroid gland.50,51,55 Abnormalities in the FGF-23/klotho axis were recently documented in critically ill foals.30 Foals with high FGF-23 and low klotho serum concentrations had more severe disease and were more likely to die.30
Organs involved in Ca2+ homeostasis (parathyroid gland, thyroid gland, and kidney), known as the calcium-sensing system, express a calcium-sensing receptor (CaR) that is activated by extracellular Ca2+ and to lesser affinity by Mg2+.36 CaR activation inhibits PTH secretion and stimulates CT secretion in various species, including the horse.15,16,39 In the kidney, CaR regulates Ca2+ and Mg2+ reabsorption independently of PTH. Renal CaR activation inhibits the furosemide-sensitive Na+∕K+∕2Cl- cotransporter in the distal nephron, resulting in diuresis and urinary waste of Ca2+ and Mg2+, in humans and horses.36,56
Calcium Disorders in the Horse
Calcium dysregulation in the horse is associated with hypocalcemic and hypercalcemic disorders. Equine pathologic conditions characterized by abnormal calcium homeostasis include hypoparathyroid- ism,57-59 primary hyperparathyroidism,60-62 nutritional secondary hyperparathyroidism,63 renal failure,64 humoral hypercalcemia of malignancy,43-47 vitamin D toxicity,65,66 exercise-induced hypocalcemia,67,68 idiopathic hypocalcemia of foals,69 cantharidiasis,70 gastrointestinal disease-23-70-74 and sepsis.6-8-23-71-73-74 Low Mg2+ concentrations can contribute to calcium dysregulation. Other conditions that may have abnormal calcium and phosphorus regulation include calcinosis-75 idiopathic systemic granulomatous disease (sarcoidosis)-3 and equine bone fragility syndrome.76
Hypocalcemic Disorders
Conditions associated with hypocalcemia in the horse are presented in Box 41.2. Calcium deficiency can be acute or chronic. Horses with acute calcium deficiency develop clinical signs associated with neuromuscular excitability and decreased smooth muscle cell contractility (Box 41.3). A decrease in extracellular Ca2+ concentrations increases cell membrane Na+ permeability- decreasing the resting membrane potential- thus making muscle cells and nerve fibers more excitable. This results in spontaneous and continuous discharges- muscle
■ BOX 41.2
Equine Clinical Conditions in Which Hypocalcemia Has Been Reported
Acute renal failure Bicarbonate administration Cantharidin toxicosis (blister beetles) Chronic renal failure
Colic
During lactation (lactation tetany) During transport (transit tetany) Dystocia
Endotoxemia Endurance exercise Enterocolitis
Furosemide administration Heat stroke
Hypomagnesemia Late pregnancy Liver disease
Magnesium toxicosis Malignant hyperthermia Oxalate ingestion
Pancreatitis Pleuropneumonia Postoperative myopathy Primary hypoparathyroidism Retained placenta Rhabdomyolysis
Sepsis
■ BOX 41.3
Clinical Signs Reported in Horses With Hypocalcemia
| Anxiety | Hyperthermia |
| Asphyxia | Ileus |
| Ataxia | Laryngeal spasm |
| Bruxism | Muscle fasciculation |
| Cardiac arrhythmias | Seizures |
| Colic | Stiff gait |
| Convulsions | Synchronous diaphragmatic |
| Death | flutter |
| Depression | Tachycardia |
| Dysphagia | Tachypnea |
| Dyspnea | Tetany |
| Excitation | Tremors |
| Hyperhidrosis Hypersalivation | Trismus |
fasciculations- tremors- tetany- and seizures. Tachycardia and cardiac arrhythmias may be present- although bradycardia may develop during severe hypocalcemia. Low serum Mg2+ concentrations are a frequent finding in horses with hypocalcemia and can further aggravate neuromuscular excitability. Chronic calcium deficiency in general is manifested as abnormal cartilage and bone development (DOD) and lameness. When calcium deficiency is suspected- feed analysis is recommended to determine if dietary calcium and phosphorus content is adequate.
Synchronous diaphragmatic flutter (SDF) or “thumps” may occur in horses with hypocalcemia associated with gastro- 2370 77
intestinal disease-23-70 endurance exercise- hypoparathyroid-
• 59 78 69 79
ism- - idiopathic hypocalcemia-69 tetany (lactation- transport)-79 23 7080 238182
sepsis-23 blister beetle toxicosis-70-80 retained placenta-23-81-82 and alkalosis.2-3 SDF develops when depolarization of the right atrium stimulates action potentials in the phrenic nerve as it crosses over the heart. Clinically- these animals have a rhythmic movement on the flank from diaphragmatic contractions that are synchronous with the heartbeat.
During alkalosis there is increased Ca2+ binding to albumin resulting in ionized hypocalcemia. Alkalosis also increases Mg2+ binding to proteins. Exercising horses may develop alkalosis from hyperventilation (respiratory alkalosis) and chloride losses in the sweat (metabolic hypochloremic alkalosis). Hypochloremic metabolic alkalosis may develop in horses with proximal gastrointestinal disease due to luminal chloride retention or losses in nasogastric reflux. Hypomagnesemia is common in horses with SDF and hypocalcemia.
Hypocalcemic tetany is the development of sustained skeletal muscular contractions in horses with hypocalcemia. Although hypocalcemic tetany can occur in any horse with hypocalcemialactating mares and horses transported for long distances are at greatest risk. Lactation tetany in mares may occur anytime immediately before foaling up to the end of the lactation period. In particular- mares producing large amounts of milk and eating diets low in calcium- grazing lush pastures- or performing physical work (draft mares) are at risk. Clinical signs may include anxiety- depression- ataxia- muscle fasciculations and tremors- stiff gait- tachypnea- dyspnea- dysphagia- hypersalivation- and hyperhidrosis (Box 41.3).2-3
Hypocalcemic seizures, seen in foals and adult horses- are caused by decreased CNS extracellular Ca2+ concentrations leading to increased neuronal excitability. Clinical signs usually improve with calcium treatment- although some animals may require repeated treatments. In general- horses and foals with refractory hypocalcemic seizures have a poor prognosis for recovery.
Ileus and retained placenta in mares are both believed to result in part from decreased smooth muscle tone and contractility secondary to hypocalcemia.2-3 While in skeletal muscle most of the Ca2+ required for contraction comes from the sarcoplasmic reticulum- in smooth muscle Ca2+ comes from the extracellular space.2 For this reason- any condition that results in hypocalcemia can decrease smooth muscle contractility. Retained placenta in mares occurs in up to 10% of foalings-81 and it has been associated with hypocalcemia.81
Hypoparathyroidism in horses is characterized by hypocalcemia- hyperphosphatemia- hypomagnesemia- and decreased serum PTH concentrations. Primary hypoparathyroidism results from decreased secretion of PTH- while secondary hypoparathyroidism results from magnesium depletion and sepsis. There are few documented cases of primary hypothyroidism in horses.58-78 Hypoparathyroidism should be suspected in any horse or foal with refractory hypocalcemia. Clinical signs include ataxia- seizures- hyperexcitability- SDF- tachycardia- tachypneamuscle fasciculations- bruxism- stiff gait- recumbency- ileus- and colic.2-3-58-83 Laboratory findings include hypocalcemiahyperphosphatemia- and low or normal serum intact PTH concentrations. Hypomagnesemia may be present in some horses and foals.6,23 Secondary (functional or acquired) hypoparathyroidism is poorly documented in the horse; however, some critically ill foals and horses with hypocalcemia have impaired parathyroid gland function,6,8,23 which could be a form of hypoparathyroidism secondary to inflammatory cytokines and/or hypomagnesemia.
A syndrome consistent with hypoparathyroidism, characterized by abnormally low PTH concentrations, hypocalcemia, SDF, and muscle fasciculations, has been recognized in young Standardbred and Thoroughbred horses by the author. The condition develops progressively, initially associated with poor performance and SDF. In some animals it has been reported after a surgical procedure (e.g., castration), while in others it has been linked to excessive calcium supplementation. The underlying cause of this disorder remains unknown. Suppression of mechanisms responsible for calcium homeostasis from excessive calcium administration, immune-mediated parathyroiditis, cytokines, and mutations in the calcium-regulatory system are potential explanations.
A number of critically ill foals develop a form of hypocalcemia that is refractory to calcium treatment.69 These foals have low or normal PTH concentrations despite hypocalcemia, suggesting hypoparathyroidism. This condition has been called neonatal idiopathic hypocalcemia.69 It is believed that abnormal parathyroid gland function may result from increased inflammatory cytokines.6,69 Prognosis for survival in foals with refractory hypocalcemia is poor.
Sepsis and endotoxemia are the most common causes of hypocalcemia in equine patients admitted to veterinary hospitals.6,8,23 Clinical observations also indicate that hypocalcemia 23 71 73 is common in horses with severe gastrointestinal disease.’’ Hypocalcemia in septic patients often results from parathyroid gland dysfunction (insufficient PTH secretion), as well as intracellular calcium sequestration.2,3,23 Inflammatory mediators known to be increased in horses and foals with sepsis and endotoxemia such as TNF-, IL-1, and IL-6 have been shown to increase CaR activation and decrease PTH secretion by equine parathyroid cells.16
Horses under intense exercise develop electrolyte and acid-base abnormalities. Exercise-induced hypocalcemia may result from Ca2+ losses in the sweat; intracellular movement of Ca2+; increased Ca2+ binding to albumin, lactate, phosphate, and bicarbonate during alkalosis; and parathyroid gland dysfunction.2,3,67,68
Oxalate toxicity causes hypocalcemia by interfering with calcium absorption; a diet consisting of 1% of oxalate or higher can reduce most intestinal calcium absorption.84 It is important that the equine diet contains less than 0.5% of oxalate or a calcium-to-oxalate ratio over 1:0. Clinical signs associated with oxalate excess are those of phosphate excess, calcium deficiency, and nutritional hyperparathyroidism. Signs of acute hypocalcemia may develop.85 Neurologic signs from excessive bone loss and vertebral fractures have been documented.85 Oxalates are present in several grasses and toxic plants (Table 41.5).
Equine cantharidiasis (blister beetle toxicosis) is a condition reported in the southwestern and midwestern United States and results from the ingestion of alfalfa contaminated with beetles (Epicauta spp.) that produce cantharidin (cantharidic acid).70,80 Clinical signs develop from the irritant effects of cantharidin on mucosal surfaces (gastrointestinal and urinary tracts). Cantharidin often causes acute hypocalcemia and hypomagnesemia. Thus, clinical signs of severe hypocalcemia (muscle fasciculations, SDF, ataxia, dyspnea, laryngeal spasm, and cardiac arrhythmias) may be present.70,80 It is unclear why these horses develop hypocalcemia; however, it may be a combination of severe gastrointestinal disease associated with acute renal tubular necrosis and parathyroid gland dysfunction.
Hypocalcemia and hypomagnesemia are common findings in horses with acute renal failure.2,3 Reabsorption of Ca2+ and Mg2+ in the kidney is highly dependent on functional tubular cells,2 and these cells are susceptible to various insults (hypoxia, ischemia, toxins).22
The pathogenesis of hypocalcemia in exertional rhabdomyolysis is unknown.86 It is speculated that damage to muscle fibers during intense exercise results in Ca2+ influx and sequestration in the sarcoplasmic reticulum.
Treatment of Hypocalcemia
Calcium deficit, maintenance, losses, and sequestration should be considered when treating hypocalcemia. If parathyroid gland function is normal, minimal to no calcium supplementation may be required. Most horses with hypocalcemia do not show overt signs of hypocalcemia. Lack of therapy, however, can result in development of additional complications, in particular ileus. Horses with functional kidneys can rapidly eliminate large amounts of calcium, and hypercalcemia from excessive calcium administration is rare, particularly if the horse is receiving fluid therapy. When possible, calculate the calcium deficit on the basis of Ca2+ concentrations (mg/dL = mmol/L ? 4). From a practical standpoint, the use of standard formulas for electrolyte deficit can be used (multiplied by 10 as calcium is expressed as mg/dL). Total calcium can be used to estimate calcium deficit, keeping in mind that total calcium has more variability than Ca2+ concentration as it is dependent on plasma protein concentration. A horse can have total hypocalcemia, but serum Ca2+ concentrations may be within the normal range (pseudohypocalcemia), and calcium administration may not be necessary. It is also important to remember that 9.3% of calcium gluconate is elemental calcium, which means that a 23% solution of calcium gluconate contains 2.14% of elemental calcium or 21.4 mg/mL. Avoid the use of injectable calcium chloride as it can cause subcutaneous irritation.
Frequent monitoring of Ca2+ concentration and adjustment of dosage is important. Rapid administration of calcium may result in cardiovascular complications, especially in septic horses, which may be more vulnerable to the toxic effects of calcium. In our experience, horses can handle high calcium dosages. For an average-size horse with mild ionized hypocalcemia (5.0 mg/dL), we administer 50 mL of 23% calcium gluconate per 5 L of crystalloid fluids, at a fluid rate twice maintenance. Oral treatment with calcium salts is feasible in some horses with non-life-threatening, refractory hypocalcemia. Dicalcium phosphate and calcium carbonate (limestone, 200 to 300 g/day) can be used safely (Table 41.3). In horses with refractory hypocalcemia, measuring Mg2+ concentrations is highly recommended.
Hypercalcemic Disorders
Hypercalcemic disorders in horses are divided into two groups: (1) parathyroid gland-dependent hypercalcemia (develops due to parathyroid gland hyperfunction) and (2) parathyroid glandindependent hypercalcemia (develops despite parathyroid gland suppression). This distinction is clinically relevant in the differential diagnosis and interpretation of specific diagnostic tests, including intact PTH, PTHrP, Ca2+, PO4, and vitamin D concentrations. Parathyroid gland-dependent hypercalcemia in the horse is limited to primary hyperparathyroidism, while parathyroid-independent hypercalcemia results from various conditions (secondary hyperparathyroidism, chronic renal failure, hypercalcemia of malignancy, hypervitaminosis D, calcinosis, and idiopathic systemic granulomatous disease).
Primary hyperparathyroidism results from an excessive and autonomous synthesis and secretion of PTH by the parathyroid gland that is not responsive to the negative feedback of Ca2+. Primary hyperparathyroidism has been reported in ponies and 5860628788
horses,58,60-62,87,88 and results from parathyroid adenomas or parathyroid hyperplasia. The elevated PTH concentrations increase renal Ca2+ reabsorption, decrease PO4 reabsorption, increase 1,25(OH)2D3 synthesis, and increase bone resorption (osteodystrophia fibrosa). Laboratory findings include hypercalcemia, hypophosphatemia, hypocalciuria, and hyper- phosphaturia. PTHrP concentrations are within normal limits (low or undetectable). Clinical findings include facial bone enlargement, lameness, and a poor body condition. Radiographic findings include decreased long and facial bone density, fibrous proliferation of the maxilla and mandible, and loss of the lamina dura surrounding the molars.60 Endoscopic examination may reveal narrowing of the nasal passages.
Nuclear scintigraphy and ultrasonography were successfully used to detect and remove a functional parathyroid adenoma in a pony.87 Ultrasonography was useful to identify parathyroid tissue within the thyroid gland of a horse with signs and laboratory findings consistent with primary hyperparathyroidism.88
Postmortem findings include enlargement of the maxilla and mandible, stenosis of the nasal passages, and loosening of premolars and molars. Histologic evaluation of the parathyroid gland is important to confirm the diagnosis of primary hyperparathyroidism; however, finding the parathyroid glands in the horse is a challenge due to their small size and variable location.2,16
Secondary hyperparathyroidism is characterized by excessive secretion of PTH in response to hyperphosphatemia and hypovitaminosis D from chronic renal failure (renal secondary hyperparathyroidism) or hyperphosphatemia and/or hypocalcemia from nutritional imbalances (nutritional secondary hyperparathyroidism). Renal secondary hyperparathyroidism is not a well-recognized disease in the horse. Unlike humans and small animals in which chronic renal failure results in hyperphosphatemia, horses with chronic renal failure (CRF) often have hypophosphatemia. Moreover, the hypercalcemia in horses with CRF is the result of renal Ca2+ retention rather than increased PTH concentrations.2,3,89 The increased Ca2+ concentrations in turn decrease PTH secretion; thus, PTH concentrations in horses with CRF frequently are below or within the normal range.3,57 In contrast, nutritional secondary hyperparathyroidism is a well-documented pathologic condition of the horse2 and is described in more detail as follows.
Nutritional Secondary Hyperparathyroidism
Definition and Etiology
Horses fed diets low in calcium, high in phosphorus, high in oxalates, or with a phosphorus-to-calcium ratio of greater than or equal to 3 : 1 may develop nutritional secondary hyperparathyroidism, also known as bran disease, miller's disease, big head, osteodystrophia fibrosa, osteitis fibrosa, and equine osteoporo- sis.2,3,63,90-94 Pastures and toxic plants with high content of oxalates (Table 41.6) predispose to secondary hyperparathyroidism. The condition remains endemic in some areas in Latin America, North America, Africa, Asia, Australia, and Europe.63,85,90,92,95-99
Pathogenesis
Excessive dietary PO4 reduces intestinal calcium absorption and results in hyperphosphatemia. With advances in animal nutrition, this condition is rarely associated with excessive grain feeding, but more commonly linked to the ingestion of oxalate-rich plants. Large amounts of oxalate (oxalic acid) bind dietary calcium to form insoluble calcium oxalate (CaC2O4), reducing calcium absorption. Oxalate also binds magnesium, but the complex (MgC2O4) is more soluble than CaC2O4 and more likely to be absorbed. Both high-phosphorus and low-calcium diets induce parathyroid cell hyperplasia and stimulate PTH secretion in the horse.3,100 Hyperphosphatemia directly stimulates PTH secretion and inhibits renal 1,25(OH)2D3 synthesis. Because 1,25(OH)2D3 inhibits parathyroid cell proliferation, low 1,25(OH)2D3 concentrations contribute to parathyroid cell hyperplasia and PTH secretion. Hyperphosphatemia also results in the formation of calcium phosphate precipitates, further reducing blood Ca2+ and inducing additional PTH secretion. PTH increases osteoclastic activity, bone resorption, and bone loss (Fig. 41.17).101 There is facial bone loss
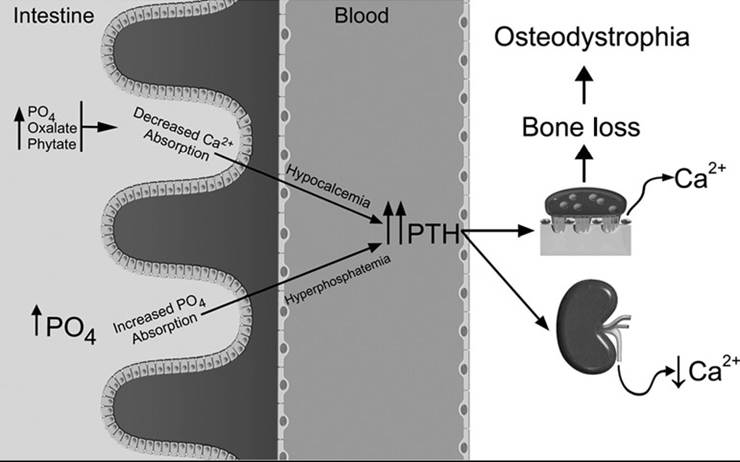
FIG. 41.17 Pathogenesis of nutritional secondary hyperparathyroidism in horses. Excessive dietary phosphorus reduces intestinal absorption of calcium and induces hyperphosphatemia. In addition, phosphate, oxalate, and phytate bind dietary calcium to reduce absorption. Both high-phosphorus and low-calcium diets induce parathyroid cell hyperplasia and stimulate PTH secretion. PTH increases osteoclastic activity and bone resorption, resulting in bone loss (osteodystrophia fibrosa).
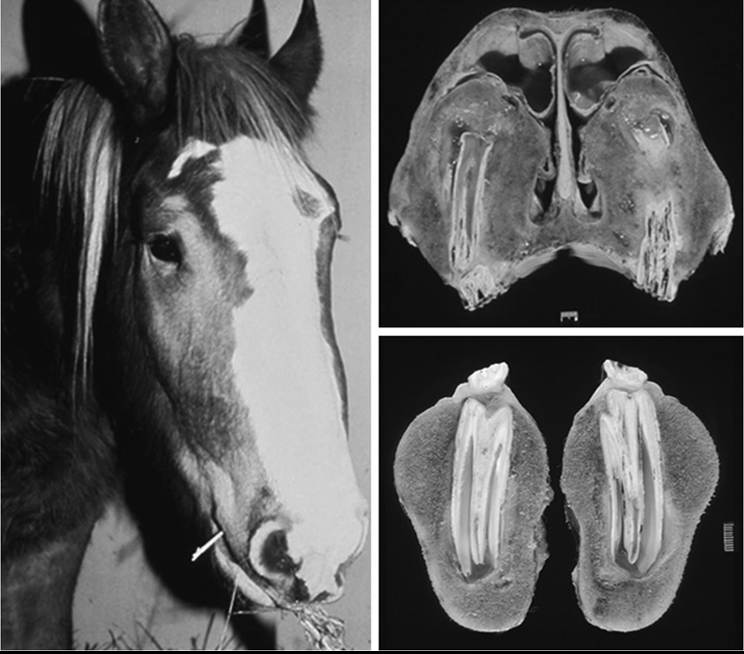
FIG. 41.18 Big head. Two-year-old Belgium horse presented to The Ohio State University Veterinary Medical Center with clinical signs consistent with nutritional secondary hyperparathyroidism, including facial bone enlargement and upper respiratory noise. The horse was fed excessive amounts of grain. There was narrowing of the nasal passages, loss of bone mass, and excessive accumulation of unmineralized bone matrix (osteodystrophia fibrosa) in maxillary and mandibular bones.
with excessive accumulation of subperiosteal unmineralized connective tissue (osteodystrophia fibrosa) resulting in facial enlargement (big head) (Fig. 41.18). Because this is a condition of slow progression, the homeostatic mechanisms that regulate extracellular Ca2+ concentrations (PTH, vitamin D, calcitonin) in general are effective in maintaining Ca2+ within the normal range. These horses preserve normocalcemia at the expense of the skeletal reserves and rarely develop clinical signs of acute hypocalcemia.
Clinical Signs
Clinical signs result from increased bone resorption and include unthriftiness; intermittent, shifting lameness; and a stiff gait. Younger animals may develop physitis and limb deformities. There is a typical and symmetric swelling of the facial bones; however, facial bone enlargement may not be evident in old horses (see Fig. 41.18). The facial changes and increased bone resorption around molars and premolars may result in masticatory problems. These horses are physically weak and may be in poor body condition from the pain associated with lameness and mastication. In severe cases, teeth may become loosened and spontaneous fractures of long bones may occur. Upper airways obstruction, dyspnea, and epiphora may be present.3,63,90-92 Vertebral demineralization and compressive neurologic signs may occur.85
Acute hypocalcemia may develop from high dietary oxalate content combined with a low-calcium diet.85 In addition, absorption of soluble oxalate can chelate calcium in circulation to worsen signs of hypocalcemia. Soft tissue mineralization was described in a foal suspected of having nutritional secondary 102
hyperparathyroidism.102
Laboratory Findings
Typical laboratory changes in horses with nutritional secondary hyperparathyroidism include hyperphosphatemia, hypocalcemia or normocalcemia (hypercalcemia is unusual), and increased intact PTH concentrations, especially if the animal is eating a low-calcium or high-phosphorus or high-oxalate diet at the time of evaluation. The urinary fractional excretion of calcium is low (hypocalciuria) while the excretion of phosphorus is increased (hyperphosphaturia). Urinary excretion of phosphorus greater than 2% is common in horses ingesting oxalate-rich plants.95 Serum alkaline phosphatase activity and collagen degradation products may be increased. Laboratory findings may be within normal limits if the animal is eating a balanced diet.
Radiologic Findings
Decreased bone density is frequent; however, bone mass must be decreased by 30% before it can be detected radiographically.3 Decreased facial bone density along with fibrous proliferation is a consistent finding. Resorption of alveolar sockets and loss of the dental lamina dura may be present before other radiographic changes are present, and long bones are affected only in advanced cases. Radiolucency and osteopenia may be evident in long bones, vertebrae, and ribs early on; however, a patchy osteoporotic pattern may be present, in particular with chronic oxalate toxicity.85
Necropsy
There is increased bone resorption, bone fragility, accumulation of fibrous tissue around facial bones, obstruction of nasal passages, and parathyroid gland hyperplasia (see Fig. 41.18).
Treatment
Diet evaluation is indicated. Eliminate or reduce any grain-based diet and avoid high-containing oxalate feeds. The addition of alfalfa to the diet may be helpful. Supplementation with calcium carbonate (limestone; CaCO3) or dicalcium phosphate may result in improvement.63 Ground limestone, which contains no phosphorus, is recommended as a good source of calcium (35%). An affected animal may require a total of 100 to 300 g/day. The diet should have a Ca:P ratio of 3 to 4:1. Limestone may decrease feed palatability, and adding molasses should be considered. Supplementation with vitamin D has been proposed. Horses may require 9 to 12 months for complete recovery, although some bone changes may not regress. Confinement of severely affected horses is advised. The use of NSAIDs may be indicated in some animals. Bisphosphonates have not been evaluated with this condition.
Hypervitaminosis D
Definition and Etiology
The ingestion or administration of ergocalciferol (vitamin D2) or cholecalciferol (vitamin D3) results in disturbances of the calcium and phosphorus metabolism in horses.65,66,103-105 Ingestion of plants containing 1,25(OH)2D-like compounds results in typical clinical signs of vitamin intoxication.103-109 The ingestion of Solanum glaucophyllum (S. malacoxylon) results in a condition known as “enteque seco” in Argentina and “espichamento” in Brazil.105,106,108,109 In Hawaii, Solanum sodomaeum, and the southern United States, jessamine (Cestrum diurnum) may cause hypervitaminosis D.103,104,107,109 In Europe, the ingestion of golden oat (Trisetum flavescens) results in enzootic calcinosis.110-112
Pathogenesis
Hypervitaminosis D increases the intestinal absorption and renal reabsorption of calcium and phosphorus. Hyperphosphatemia is the most consistent and early laboratory finding in horses with vitamin D intoxication.65,66,102 Serum calcium concentrations may be increased or within the normal range.65,66,102,103,106 Hypervitaminosis D results in parathyroid cell atrophy and decreased PTH secretion. In addition, hypercalcemia contributes to decrease PTH secretion, lowering bone turnover. Azotemia and hyposthenuria may be present.65,66
Clinical Signs
Most clinical findings in horses with hypervitaminosis D are the result of hyperphosphatemia. These horses often have weight loss, poor appetite, lameness, and painful stiffness, and they are reluctant to move. Acute death from severe cardiovascular mineralization has been reported.65,66 Polyuria and polydipsia are frequent findings. In cases with hypercalcemia, mineral deposition in the kidneys may precede mineralization elsewhere, resulting in renal failure. Lameness is probably due to calcification of ligaments and tendons.
Radiologic Findings
These horses often have increased bone density, decreased size of the medullary cavity, and increased calcification of soft tissues.
Treatment
Reducing dietary calcium intake and the use of calcium- binding agents such as sodium phytate has been proposed.105 Glucocorticoids are used in humans with hypervitaminosis D because they may inhibit the vitamin D-mediated intestinal calcium absorption. In equids, glucocorticoids decrease intestinal absorption of calcium, increase urinary excretion of calcium, and decrease bone resorption.20,21 Dexamethasone has been administered to horses with hypervitaminosis D with variable results. Drugs that suppress osteoclastic bone resorption (bisphosphonates) have not been evaluated in horses with hypervitaminosis D. The prognosis for horses with hypervi- taminosis D is poor.
Necropsy Findings
Postmortem examination may reveal mineralization of soft tissues. Mineralization of the endothelium of the aorta and pulmonary vessels, as well as of the endocardium, is frequent. Mineralization may be found in the kidney, liver, lymph nodes, lungs, ligaments, and tendons. Osteopetrosis of epiphyses and metaphyses may be present. Atrophy of the parathyroid gland
Hypercalcemia of Malignancy
Humoral hypercalcemia of malignancy (HHM, pseudohyperparathyroidism) is a paraneoplastic condition in which humans and animals develop hypercalcemia associated with various types of tumors. These malignancies secrete parathyroid hormone-related protein (PTHrP), which interacts with PTH receptors to increase renal reabsorption of Ca2+ and bone resorption.113 In horses, HHM has been associated with squamous cell carcinoma, adrenocortical carcinoma, lymphosarcoma, multiple myeloma, and ameloblastoma.2,3 Laboratory findings include hypercalcemia, hypocalciuria, hypophosphatemia, hyperphosphaturia, normal or low PTH concentrations, and increased PTHrP concentrations. HHM should be suspected in any horse with hypercalcemia, no evidence of renal disease, and normal PTH concentrations.
Neonatal Hypercalcemia and Asphyxia
Clinical observations indicate that a number of critically ill newborn foals develop hypercalcemia associated with peripartum asphyxia (neonatal encephalopathy). The mechanisms underlying this problem remain unknown, although it is speculated to be associated with placental insufficiency.
Idiopathic Systemic Granulomatous Disease
This is an immune disorder documented in horses and ponies (equivalent to human sarcoidosis), in which crusty skin lesions develop along the coronary bands and mucocutaneous junctions. Granuloma formation in multiple organs is the hallmark.114-116 Some animals may develop hypercalcemia.114 Lesion distribution may resemble those of multisystemic eosinophilic epitheliotropic disease of horses. It has been proposed that excessive production of vitamin D or PTHrP by granulomatous cells leads to hypercalcemia in these animals.3,114 Similar lesions have been documented in horses and cattle grazing hairy vetch (Vicia villosa).ιvι,lls
Calcinosis
Soft tissue calcification (liver, heart, kidney, lungs, vessels, muscle), hyperphosphatemia, and elevation of the calcium ? phosphorus product were documented in horses with a number of pathologic conditions.75 This disorder is different than enzootic calcinosis from the ingestion of plants with vitamin D-like activity. The mechanism by which these animals develop calcinosis is unclear, although it is likely that hyperphosphatemia plays a role.
Equine Bone Fragility Syndrome
The equine bone fragility syndrome (BFS) or silica-associated osteoporosis (SAO) is a chronic and progressive disorder of horses characterized by increased respiratory efforts, exercise intolerance, skeletal deformation, lameness, stiffness, and fractures.119,120 (Also see the Equine Bone Fragility section in Chapter 38.) Horses of any age are affected.119,121 Bowing of appendicular bones (scapula in particular), lordosis, and neurologic signs from vertebral deformation and spinal cord compression have been documented.119,120 The pathogenesis remains unclear, but it has been associated with pulmonary silicosis. Radiographically, there is osteopenia and a respiratory pattern consistent with silicosis. Intracellular silica crystals (silica dioxide) in bronchoalveolar cells and pulmonary macrophages, as well as evidence of dystrophic calcification, are consistent with SAO. A high concentration of cristobalite, a fibrogenic form of silicate, is found in regions of California where the condition is more common (Monterey shale soil).76,119,120,122 Histologically, there is excessive osteoclastic activation and bone resorption. In the respiratory tract there is pulmonary granuloma formation, fibrosis, and lymphadenitis.76 The diagnosis of BFS is based on clinical history, clinical findings, geography, and imaging (ultrasonography, radiography, and scintigraphy). Nuclear scintigraphy is the best diagnostic modality, but scapular ultrasonography can be diagnostic in some animals.121 Management of these horses depends on clinical signs and prevention. Nonsteroidal antiinflammatory drugs should be considered in animals with orthopedic pain considering that their use can increase the risk of fractures. Glucocorticoids may be necessary in severe pulmonary disease, but they also enhance bone loss. This is one of the few equine conditions in which bisphosphonates may be indicated.123 Zoledronate has reduced the severity of clinical signs and scintigraphic findings in horses with BFS.123 Decreased physical activity and dietary manipulation are recommended.
Treatment of Hypercalcemia
Hypercalcemia as an equine emergency is rarely presented; however, the differential diagnosis of hypercalcemia is important for its treatment. Few disorders in the horse are associated with hypercalcemia (hyperparathyroidism, CRF, HHM, hypervitaminosis D). Mild to moderate hypercalcemia in general is not life-threatening, and treatment should be directed to the primary cause. Parathyroidectomy will be treatment of choice for primary hyperparathyroidism.87 Bisphosphonates and calcimimetics (cinacalcet) are also recommended in people with hyperparathyroidism124,125; however, information on their use for this condition in horses is lacking. Bisphosphonates can cause renal injury in people and, anecdotally, in horses as well. In theory, calcitonin could reduce serum calcium concentrations, but this effect is transient. Surgical removal of epithelial tumors can be a successful treatment for HHM. Some horses with lymphosarcoma may show improvement with chemotherapy. Bisphosphonates and gallium nitrate have shown benefits in reducing serum calcium and bone resorption in people with HHM.126 Bisphosphonates improved signs in horses with BFS.123 In severe cases of hypercalcemia that may require medical treatment, initial therapy should include the administration of 0.9% saline solution and loop diuretics. Furosemide is the diuretic of choice because it inhibits the Na+/K+/2Cl- cotransporter in the distal tubules, increasing the urinary excretion of calcium. Thiazide diuretics are contraindicated because they stimulate calcium reabsorption. Glucocorticoid administration should be considered, in particular for horses with hypervitaminosis D.
Phosphorus Disorders in the Horse
Disorders of phosphorus homeostasis can be acute or chronic, resulting in hypophosphatemia or hyperphosphatemia. In critically ill horses hypophosphatemia is more frequent, while in foals hyperphosphatemia is more common.6,127
Hypophosphatemic Disorders
Hypophosphatemia develops from reduced intestinal PO4 absorption, increased urinary PO4 excretion, and intracellular shift of PO4 (redistribution). Acute hypophosphatemia often reflects PO4 redistribution from the extracellular to intracellular compartment and not necessarily imply total body PO4 depletion. However, PO4 depletion may occur in animals that have been sick for many days. From personal experience, hypophosphatemia seems to be more common in small equids, usually associated with hyperlipemia and parenteral nutrition. Intestinal PO4 absorption is reduced by gastrointestinal disorders, hypovitaminosis D, PO4-deficient diets, and interfering substances. Urinary excretion of PO4 is increased with hyperparathyroidism, hypovitaminosis D, malignancies that secrete phosphatonins or PTHrP, chronic renal failure, and drugs. Sepsis, carbohydrate-rich diets, hyperglycemia, insulin administration, starvation, refeeding syndrome, hyperlipemia, and parenteral nutrition (hyperglycemia, hyperinsulinemia) decrease serum PO4 mainly through insulin-mediated intracellular shift of PO4 and enhanced glycolysis. Catecholamines act by a mechanism similar to insulin shifting PO4 into the cell. Alkalosis induces hypophosphatemia by stimulating phosphofructokinase activity (glycolysis) and the need for PO4 to synthesize ATP. In horses with a history of malnutrition, close monitoring of serum PO4 concentrations is indicated once caloric intake resumes because they may develop refeeding syndrome. Clinical signs of acute hypophosphatemia in horses often go unnoticed. Signs are consequence of PO4 regulatory functions on energy metabolism, cell membrane stability, and ion transport.3 These include muscle weakness, fasciculations, dysrhythmias, neuromuscular excitability, ileus, and cell membrane fragility and lysis (hemolysis, rhabdomyolysis). Signs from mild hypophosphatemia are difficult to document. Severe hypophosphatemia can result in tissue hypoxia from reduced erythrocyte content of 2,3-bisphosphoglycerate. Chronic hypophosphatemia is rare in horses and manifests as weight loss, weakness, depraved appetite (pica), reduced bone density, DOD, lameness, and hemolysis. Ideally, therapy for hypophosphatemia would be based on the extracellular deficit, which should be overestimated because PO4 is a major intracellular anion and cellular depletion is likely to occur in animals with prolonged hypophosphatemia. Preferred parenteral solutions include potassium phosphate and sodium phosphate. Critically ill horses can be supplemented with oral potassium phosphate or sodium phosphate (chemical grade or with phosphate-based enema solutions). Oral supplementation with dicalcium phosphate is a good option in animals with chronic phosphate deficiency.
Hyperphosphatemic Disorders
Hyperphosphatemia develops from increased PO4 absorption; acute renal injury; hypoparathyroidism; vitamin D toxicity; metabolic acidosis; cell lysis (hemolysis, rhabdomyolysis, tumor necrosis); or iatrogenic causes.3 Lactic acidosis may cause hyperphosphatemia by shifting PO4 to the extracellular compartment. Metabolic acidosis and high intracellular ATP concentrations inhibit phosphofructokinase, a key enzyme in glycolysis that uses PO4 for carbohydrate phosphorylation. Overuse of phosphate-based enemas can cause hyperphosphatemia in foals. Unlike other species, chronic renal failure is an uncommon cause of hyperphosphatemia in horses. Inappropriate blood sample handling can result in spurious hyperphosphatemia. Hemolysis, hyperbilirubinemia, hypertriglyceridemia (hyperlipidemia), and hyperproteinemia can falsely elevate PO4 values (pseudohyperphosphatemia). Multiple myeloma can cause pseudohyperphosphatemia from high circulating immunoglobulin concentrations. Acute hyperphosphatemia may cause hypocalcemia from interactions between PO4 and Ca2+ and reduced renal synthesis of 1,25(OH)2D. Hyperphosphatemia is common in critically ill foals.6,127 The pathogenesis of chronic hyperphosphatemia is described in the Nutritional Secondary Hyperparathyroidism section. Clinical signs of acute hyperphosphatemia are similar to those of acute hypocalcemia and include tetany, hyperexcitability, muscle fasciculations, colic, and dysrhythmias. Signs of chronic hyperphosphatemia are those of calcium deficiency, including lameness, orthopedic pathologies, fractures, and osteodystrophia fibrosa. Treatment of hyperphosphatemia is based on primary pathology and duration, which in some instances may not be necessary. In acute hyperphosphatemia, fluid therapy and diuretics are indicated. Dietary PO4 restriction must be implemented in chronic hyperphosphatemia. Dialysis and phosphate binders are impractical and expensive. Calcium carbonate is a cheap phosphate binder that also provides calcium supplementation. Phosphate-binding polymers (e.g., sevelamer) are the most effective way to treat chronic hyperphosphatemia in other species, but their use is not described in horses.