Parenchymal liver diseases of the dog
erative structures contain both hepatic parenchymal and biliary elements and may reflect either a regenerative proliferation of a hepatic stem cell population or the transformation of regenerating hepatocytes into ductular-like structures.
These regenerative structures generally are most prominent in the periportal areas. With chronic parenchymal damage or extensive loss of hepatocytes, fibrosis and postnecrotic scarring may occur and may be associated with the formation of intrahe- patic portovenous shunts. In such cases, the prolonged regenerative effort will result in regenerative parenchymal nodules.A definitive diagnosis of hepatitis requires histology of the liver. The histopathological diagnosis should include the type, pattern, and extent of the necrosis and inflammation, the possible cause, and in more chronic cases the presence, pattern, and extent of fibrosis and regeneration. The activity of the inflammatory process is defined by the amount of hepatocellular necrosis and inflammation, while the chronicity is determined by the amount of fibrosis.
7.5.1.1.1 AcuteHepatitis
Etiology
Acute hepatitis can be caused by chemicals (the most common ones are organic solvents such as tetrachloromethane [CCl4] and phosphorus), drugs (e. g., benzodiazepine in cats, acetaminophen in all mammals, trimethoprim sulfonamide, carprofen, and the antibiotic nalidixate), viral infection (e.g., infectious canine hepatitis), and mycotoxins (especially aflatoxin B1).10 Hepatitis resulting from sepsis (i.e., reactive hepatitis), leptospirosis, and hemolysis are discussed in other sections below. Drugs containing sulfonamides may induce a severe type of hepatitis, which, however, presents mostly as a chronic disease.
7.5.1.1
Canine hepatitis
Pathogenesis
Hepatitis is a common liver disease in dogs, but is extremely rare in cats.
Therefore, the following discussion on hepatitis is exclusively focused on dogs. The primary inflammatory disease of the hepatobiliary tract in cats is cholangitis, an inflammatory disease of the biliary system, whereas in dogs hepatitis is primarily a parenchymal disease.5,10Any destruction of the hepatic parenchyma either due to apoptosis or necrosis may be followed by an inflammatory reaction, regeneration of the parenchyma, fibrosis, and ductular proliferation. When hepatocellular destruction is limited and the reticulin network remains intact, regeneration with complete restitution of the hepatic structure can occur. However, severe parenchymal destruction with extensive loss of hepatocytes is often followed by ductular proliferation. Many regenDepending on the extent of the hepatocellular necrosis, differing amounts of intracellular enzymes will be released and bile will leak back into the circulation. In an acute hepatitis, all of the serum hepatic enzyme activities are usually elevated. Fever can, but does not always, occur as a result of pyrogens from the necrotic tissue and a reduced removal of endotoxins and bacteria from the portal blood. DIC is also very common. When hepatocellular necrosis is extensive and a significant portion of hepatic function has been lost, the condition is classified as fulminant hepatitis. Fulminant hepatitis leads to the development of HE, DIC, jaundice, and hypoglycemia. The hypoglycemia is due to a lack of glycogen synthesis and glyconeogenesis. Fulminant hepatitis rapidly progresses to coma and death.
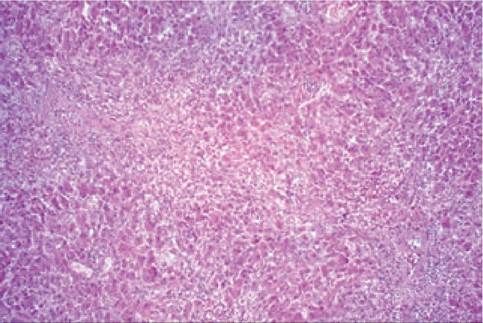
Figure 7.8:
Fulminant hepatitis. This histopathological section from a dog with fulminant hepatitis shows diffuse necrosis of hepatocytes throughout (H&E stain; 40?).
Acute hepatitis is characterized by hepatocellular necrosis that is followed by an inflammatory reaction (Figure 7.8). Depending on the severity of the hepatitis, there may be apoptosis, focal necrosis, and confluent or bridging necrosis.
The inflammatory infiltrate consists of round cells and neutrophils. Infection with canine adenovirus-1 is usually characterized by confluent and bridging necrosis in the centrolobular zone and by the presence of intranuclear inclusions in the hepatocytes and Kupffer cells. The virus can be demonstrated in a histological liver section by the presence of intranuclear inclusion bodies or by immunofluorescence. Acute hepatitis may also be caused by various toxins,49-55 such as mushroom toxins (e. g., Amanita spp.), blue-green algae toxins (e.g., Cyanophyceae), idiosyncratic drug toxicities (e.g., sulfonamides, carprofen, or amiodarone), or dose-dependent drug toxicities (e.g., acetaminophen).Symptoms
Hepatitis is associated with acute illness, apathy, sometimes fever, anorexia, vomiting, dehydration, sometimes icterus, and in severe cases DIC. In its most severe form, fulminant hepatitis, all hepatic functions fail, resulting in rapidly worsening HE, icterus, and bleeding diathesis. The clinical picture, however, is entirely dependent on the severity of the liver damage. Usually, acute hepatitis is a moderately severe disease and most dogs recover completely.
Diagnosis
A serum chemistry profile usually reveals elevations of liver enzyme activities, especially ALT, and sometimes hyperbilirubinemia. The diagnosis is confirmed by percutaneous liver biopsy.
Treatment
As the cause of the hepatitis cannot be identified in most cases, no specific treatment is available or needed. In more severe cases, supportive treatment may include IV fluid administration to correct hypovolemia, shock, acidosis, or alkalosis, hypoglycemia, and electrolyte disturbances. Corticosteroids are contraindicated. In patients with severe liver damage, an antibiotic (e.g., ampicillin) may be a helpful to eliminate bacteremia that can be present due to inadequate hepatic clearance of the portal blood. Phalloidin and acetaminophen intoxication cause oxidative damage and should be treated with sily- marin (50 mg/kg/day PO q 24 h for 3-5 days).
Silymarin has been reported to be less effective when given a few hours after intoxication. Acetaminophen intoxication may also be treated with the combination of N-acetylcysteine (140 mg/kg PO q 6 h for 3 days), vitamin C (25-35 mg/kg PO q 6 h for 2 days), and cimetidine (5 mg/kg PO q 12 h for 4 days). Dogs with acetaminophen intoxication may have hemolysis and a blood transfusion may be required.Follow-up
Patients with acute hepatitis recover spontaneously in most cases, but in about 10% of patients the disease progresses to a chronic hepatitis. The chronic disease usually does not lead to clinical signs in the first few months, but often becomes clinically apparent at a much later stage of hepatic dysfunction. It is, therefore, recommended to perform a second liver biopsy four to six weeks after a diagnosis of acute hepatitis to identify patients with chronic hepatitis at an early stage. Early chronic hepatitis is often not associated with abnormal serum liver enzyme activities or bile acids concentrations, and without a control biopsy these cases may be missed.
7.5.1.2 Leptospirosis
Etiology
Leptospira spp. organisms are transmitted with the saliva and urine from infected rats or dogs. Animals may become asymptomatic carriers transmitting the disease without being ill themselves. Experimentally, infection is mostly pathogenic in young dogs and older dogs often remain asymptomatic. After an incubation of one to three weeks, acute illness ensues with
uremia and icterus, which is caused by intrahepatic cholestasis. Myositis often causes pain upon palpation and also a painful gait. Without treatment, the resulting renal insufficiency is usually fatal, but depending on the strain of the organism that causes the infection, the hepatic lesions are usually not as severe.
In the liver, leptospirosis causes a nonspecific reactive hepatitis. Bacterial enzymes cause detachment of the tight junctions, which stimulate hepatocyte mitosis. Thus, the most characteristic histological finding is an increased number of mitotic figures in the hepatocytes (Figure 7.9).
There is usually extensive intrahepatic cholestasis, and nearly all patients are icteric.Symptoms
The symptoms of leptospirosis are mainly dominated by renal insufficiency or failure, and include acute illness, malaise, fever, vomiting, icterus, muscle pain and sometimes diarrhea or pe- techiations due to thrombocytopenia.
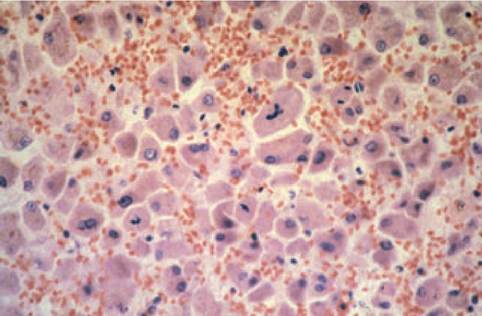
Figure 7.9:
Leptospirosis. This histopathological view shows several mitotic figures of hepatocytes, which is typical for dogs with leptospirosis (H&E stain; 100?).
Diagnosis
Many patients with leptospirosis have icterus. The serum chemistry profile may reveal uremia and cholestasis with elevated serum bilirubin concentrations, AP activities, and bile acids concentrations. Serum creatinine kinase (CK) activities are often elevated, reflecting the myositis. Many patients also show thrombocytopenia. Urinalysis often reveals indicators of nephritis, such as tubular epithelial cells in the sediment and / or proteinuria.
The histopathology of a liver biopsy mostly shows a nonspecific reactive hepatitis, which may occur with any type of sepsis. A definitive diagnosis can only be made by serology. There is a rapid IgM peak, which reaches a maximum after about 4 days of infection, followed by an IgG peak at least 10 days later. The IgM peak remains for 2-3 weeks, and the specific measurement of IgM in the serum is the only method to confirm the diagnosis in an early stage of the disease. IgG is only indicative for infection in animals that have never been vaccinated, or when serum IgG titers increase over time.
Management
Often, penicillin is initially used until hepatic and renal functions are completely recovered, at which point streptomycin is given on two consecutive days. This prevents the continuing excretion of Leptospira in the urine. Leptospira excretion stops after two days of penicillin administration and no more Leptospira are excreted as long as the penicillin is continued.
This is especially important as leptospirosis is an important zoonosis, which can lead to morbidity and even acute renal failure in human patients. Alternatively to penicillin and streptomycin, doxycycline at the standard antibiotic dose can be used.Leptospirosis can be prevented by vaccination, which is important for dogs at risk, such as hunting dogs. However, vaccination only protects from infections due to certain serovars and recently an increasing number of cases have been documented that are due to serovars for which no vaccines are available.
The prognosis depends on the degree of renal damage. Acute illness with jaundice is an indication to examine renal function. Antimicrobial therapy should be started immediately. Despite appropriate therapy, the infection is lethal in many cases. All patients with acute disease associated with jaundice and uremia should be treated as leptospirosis suspects, until leptospirosis has been ruled out.
7.5.1.3 Chronic hepatitis and hepatic cirrhosis
Chronic hepatitis and hepatic cirrhosis are discussed together here because they have the same pathogenesis and their clinical and pathological changes often overlap.5,10 Chronic hepatitis is characterized by periportal fibrosis, infiltration of the hepatic parenchyma with lymphocytes and plasma cells, and periportal liver cell apoptosis or necrosis. Apoptotic liver cells become smaller and acidophilic, and are also known as acidophilic bodies. Expansion of the inflammation may extend to form porto-portal or porto-central bridging fibrosis. If the fibrosis forms septa connecting the portal and centrolobular areas, the normal functional architecture of the hepatic lobules

Figure 7.10:
Micronodular cirrhosis. This figure shows a liver from a dog with inherited copper storage disease. The nodules are diffusely dispersed throughout the liver and are generally very small. This finding of micronodular cirrhosis is typical for copper storage disease as opposed to other causes of cirrhosis in dogs.
become permanently disturbed: this is called cirrhosis. The liver has an enormous regenerative capacity, which is more pronounced than that of most other tissues, but in the case of cirrhosis regeneration is non-organized and forms nodules of hyperplasia (Figure 7.10). These nodules embody almost nonfunctional liver tissue. Cirrhosis represents the end-stage of chronic hepatitis. Macronodular cirrhosis is the most common form of hepatic cirrhosis in dogs, but micronodular cirrhosis can be seen in chronic hepatitis associated with copper storage (Figure 7.10). Chronic hepatitis is associated with fibrosis, and the more fibrosis that occurs, the less capacity the parenchyma has to regenerate. This leads to a permanent loss of hepatocytes and the liver becomes smaller. Fibrosis, especially cirrhosis, also obstructs the normal portal blood flow. Portal blood is required to activate hepatic growth factors, so that decreased portal perfusion also contributes to decreased liver regeneration. Altogether, advanced fibrosis can lead to cirrhosis through a vicious cycle. Therefore, it is crucial that the clinician diagnoses chronic hepatitis during an early stage, permitting intervention. The inflammatory infiltration and the loss of liver cells vary from case to case, depending on the degree of activity of the process. Chronic hepatitis and cirrhosis cause variable degrees of intrahepatic cholestasis, but in most cases there is no icterus.
Etiology
Chronic active hepatitis may be caused by a viral infection.56 Canine adenovirus-1 (CAVl) is the only known canine hepatitis virus. CAVl virus infection in non-vaccinated animals leads to fulminant hepatitis. The author has not been able to identify high titers against CAV1 in most dogs with chronic hepatitis. It is also likely that there are other viruses that can cause chronic hepatitis in dogs. However, the lymphocytic and plasmacytic inflammation and the good response to immunosuppressive drugs indicate that a self-perpetuating autoimmune process plays a role in chronic hepatitis.
Chronic hepatitis and cirrhosis may also be due to chemicals or toxins (e.g., aflatoxin). Metabolic alterations in the liver, primarily inherited copper toxicosis, also can lead to damage of hepatocytes with secondary hepatitis and fibrosis. However, in patients with this condition, lesions begin in Zone 3 of the acini instead of in the portal areas. Our group has recently shown that Doberman Pinschers and Labrador Retrievers, which are also frequently affected by hepatitis, have an inherited form of copper storage disease (see 7.5.1.4). In Doberman Pinschers, this form of chronic hepatitis is very aggressive and sex-linked with a predilection for female dogs. Copper-associated hepatitis also occurs frequently in a variety of Spaniel breeds.
Pathogenesis
The gradually progressive hepatocellular necrosis may cause a continuing elevation of all serum liver enzyme activities and serum bile acids concentration. However, in patients where the hepatitis is not very active or in those with end-stage disease that is associated with cirrhosis, the release of hepatic enzymes into the blood stream may be insignificant and in turn the serum enzyme activities may be normal or only slightly elevated. Icterus does not develop consistently.
Chronic hepatitis is always a diffuse process. Hepatic function is diminished due to the loss of functional tissue mass and also reduced portal blood flow. Often the patient shows low serum albumin and fibrinogen concentrations. HE may develop if portosystemic collaterals are formed (Figure 7.11). Patients with end-stage disease usually develop cirrhosis. Hypoalbu- minemia and portal hypertension may cause ascites.
Chronic hepatitis may occur at any age. In those breeds that have chronic hepatitis due to abnormal copper metabolism, the gradual accumulation of copper usually leads to onset of clinical signs at an age of 4-7 years. Chronic hepatitis can occur in all breeds, but the most frequently affected ones are Labrador Retrievers (Golden Retrievers are affected to a lesser extent), Doberman Pinschers, all Spaniel breeds, Bedlington Terriers, and West Highland White Terriers (see also 7.5.1.4).
The incidence of chronic hepatitis is relatively high. It is one of the most common liver diseases seen in dogs and accounts for approximately 1% of all cases presented to a referral clinic.
Symptoms
The most frequently observed symptoms in patients with chronic hepatitis are apathy, reduced appetite, vomiting, poor endurance, polydipsia, and sometimes icterus. In advanced cases, there may be ascites and HE.
Diagnosis
Physical examination usually reveals no specific findings. All serum hepatic enzyme activities are more or less increased. In advanced cases there may be hypoalbuminemia. The diagnosis can only be made by the histopathological evaluation of liver biopsies. Ultrasonography prior to biopsy is advised. Cirrhosis may be suspected based on the appearance of a small liver with an irregular surface and structure. Many patients with chronic hepatitis, however, show no abnormalities at all on abdominal ultrasonography.
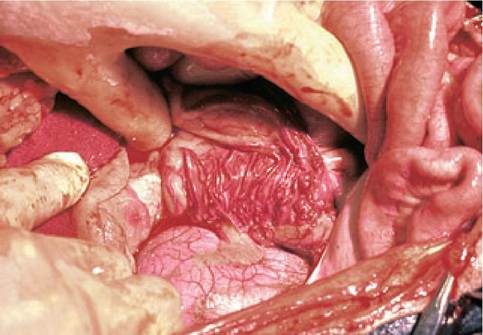
Figure 7.11:
Portosystemic collaterals. Patients with hepatic cirrhosis may develop multiple portosystemic collaterals as the liver can no longer handle physiological portal blood flow. The patient shown here has developed several collaterals near the left kidney.
Prognosis
Management
Prednisolone or prednisone are used as anti-inflammatory (0.5-1.0 mg/kg PO q 12 h) or immunosuppressive (1-2 mg/ kg PO q 12 h) agents. If the side effects of the steroids are intolerable, a combination of prednisone (0.5 mg/kg/day PO) and azathioprine (1.0 mg/kg/day PO) can be used. It is important to carefully evaluate the response to treatment by repeat liver biopsies (e. g., every 6 weeks). Corticosteroids themselves cause changes in the liver, therefore, blood work alone is not suitable to evaluate the response to treatment. Medication must be continued until there is complete histological recovery, which is usually after 8-12 weeks.
Without treatment, the disease progresses to cirrhosis. Apart from specific therapy directed at the hepatitis, more advanced cases also require supportive care directed at dehydration and management of the risks of HE. The risk for HE can be predicted by an ammonia tolerance test. Most therapies for hepatitis in dogs have been poorly evaluated. Based on the pathophysiological considerations, one could also treat dogs with hepatitis with ursodeoxycholic acid (ursodiol, 5-15 mg/kg PO q 24 h) and/or S-adenosylmethionine (SAME) at the manufacturer’s recommended dose. The clinical effect of these medications has not been proven, but it has become common practice by some clinicians to use a combination of prednisone, ursodiol, and SAME in a polypharmaceutical approach.
The prognosis for dogs with chronic hepatitis is dependent on the stage of the disease and can be guarded to good. The disease can often be stopped completely. Sometimes there is a recurrence, requiring repeated treatment. In cases of cirrhosis, the prognosis depends on the activity of the ongoing hepatitis and the degree of hepatic regeneration. If the hepatitis is still active, judged by the number of inflammatory cells, significant improvement may be achieved. Even liver perfusion may improve and the portal hypertension may decrease. There is no proven treatment to reduce fibrosis and dogs with chronic forms of hepatitis will have fibrosis even after they have been treated successfully. Depending on the formation of collateral vessels, canine patients with chronic hepatitis may develop portovascular anomalies and require permanent support with a special diet and /or lactulose.
7.5.1.4 Chronic hepatitis due to copper storage in the liver
Etiology
Hepatitis due to copper storage occurs as a result of an inherited defect in the copper metabolism of hepatocytes, resulting in impaired excretion of copper into the bile. Most foods contain an excess of copper, which is absorbed in the small intestine and cleared from the portal blood by the liver. The copper excess is normally excreted into the bile by the hepatocytes and thereby cleared from the body. Copper is an essential element and, after incorporation into ceruloplasmin by the liver, is distributed throughout the body. The normal metabolic pathways of copper in hepatocytes are only partly known. Intracellular trafficking of copper only occurs in the proteinbound form, since free copper causes oxidative damage to cells. In inherited copper storage disease, the gradual accumulation of copper in the hepatocytes causes oxidative damage and, ultimately, hepatocellular necrosis that induces a secondary inflammatory reaction. The accumulation of copper and inflammation occurs mostly around the central veins, whereas other forms of chronic hepatitis concentrate in and around the portal areas. As with other forms of chronic hepatitis, copper- related hepatitis can also progress to cirrhosis (Figure 7.10). The gradual accumulation of copper leads to the onset of clinical signs at an age of 4-7 years in most breeds. High hepatic copper concentrations (>1,000μg∕g dry liver tissue) indicate an inherited form of copper storage disease. Although copper needs to be excreted with the bile, cholestasis never causes such high copper concentrations in the liver.
Copper storage disease occurs in a variety of breeds: Anatolian Shepherds, Bedlington Terriers, Dalmatians, Doberman Pinschers, Labrador Retrievers, Skye Terriers, all Spaniel breeds, and West Highland White Terriers.11,57-67 In Doberman Pinchers, the disease affects only females. In other breeds with this disease, both sexes are affected, however, usually with a female overrepresentation. The underlying gene defect has only been discovered in the Bedlington Terrier, where it has been shown to be an autosomal recessive disease. Heterozygote carriers cannot be distinguished phenotypically from homozygote healthy animals.Very recently, a reliable DNA test for the causative deletion in the COMMDl gene in this breed has been reported (this test is commercially available through VetGen, Ann Arbor, MI).11 The causative gene is not known for any of the other breeds; therefore, the diagnosis depends on the collection of a liver biopsy, histochemical copper staining, and the quantitative analysis of copper content. The increased copper concentration in the liver of affected dogs can be confirmed only after about 1 year of age, as these dogs may not have stored sufficient copper beforehand.
Pathogenesis
Oxidative damage to cellular organelles causes cell death followed by an inflammatory reaction. A chronic persistent hepatitis develops and as a result the liver loses its regenerative capacity and forms fibrous tissue. In the final stages, cirrhosis may develop.
Bedlington Terriers may develop an acute hemolytic anemia. The hemolysis is probably the result of release of copper from the liver into the blood due to hepatocellular necrosis. Because the liver function is already reduced, this hemolysis usually leads to severe icterus.
Symptoms
The symptoms are the same as those seen in patients with other forms of chronic hepatitis and include apathy, reduced appetite, vomiting, poor endurance, polydipsia, and sometimes icterus.
Diagnosis
Copper hepatotoxicity cannot be differentiated from other forms of chronic hepatitis and hemolysis based on physical examination and blood tests alone. Instead, the diagnosis is based on a histological examination of liver biopsies. The association of the hepatitis with an excessive copper content is based on histochemical copper staining and quantitative copper analysis in a hepatic biopsy. The normal concentration of copper in the dog liver is between 50 and 300 μg∕g dried hepatic tissue. Bedlington Terriers with copper accumulation have concentrations exceeding 1000 μg∕g at one year of age, but in other breeds the accumulation seems to progress much slower and even the highest concentrations seen in these breeds are lower than those seen in Bedlington Terriers.
Management
Copper storage disease should be treated with a copper-binding chelating drug.68 Penicillamine is widely used and is given in two daily doses of 20-35 mg∕kg, 30-60 min before each meal. Penicillamine binds copper and the complex is excreted in the urine. Gradual removal of free excessive copper reduces the degree of hepatitis. Female Dobermans, which used to have a poor prognosis when diagnosed with hepatitis, often recover completely when treated with copper-chelating agents.68 The response to treatment should be evaluated by repeated liver biopsies. For most patients with copper storage disease, a biopsy interval of three months is appropriate.
If the hepatitis appears cured, recurrence should be prevented as the genetic basis for the abnormal copper metabolism remains. Long-term prevention may be achieved with zinc (15 mg/kg PO q 12 h, given with each meal). Zinc induces intestinal metallothionein, which binds copper and prevents copper absorption. Modern low-copper diets are advised for supportive care. There is good evidence from double-blind, randomized and placebo-controlled studies that penicillamine is effective in dogs of different breeds with copper storage disease. There is only limited evidence that trientine, another copper-chelating agent is efficacious in canine patients with copper storage disease and routine use cannot be advised at this point. The beneficial effect of zinc is well proven in different species. Since complete recovery is commonly achieved with penicillamine and zinc there is no need to use other drugs. However, there is no contraindication for the use of ursodiol and SAME in these patients (see 7.5.1.3).
7.5.1.4 Lobular dissecting hepatitis
Etiology
The etiology of lobular dissecting hepatitis is unknown. However, the author has seen this form of hepatitis in kennels where several dogs have had the disease, all at different ages. In the absence of any indication for a toxic cause, this would suggest an, as of yet unknown, infectious etiology.69
Pathogenesis
Lobular dissecting hepatitis is a diffuse hepatitis with pericellular fibrosis around all the hepatocytes. The amount of fibrous tissue is excessive and usually leads to severe portal hypertension, which in turn may quickly cause ascites, acquired portosystemic collaterals, and HE. The progression of this disease is usually much more rapid than the regular form of chronic hepatitis and the course of this disease usually takes weeks rather than months. The clinical picture of lobular dissecting hepatitis closely resembles that of hepatic cirrhosis and congenital portal vein hypoplasia. In fact, this condition more appropriately should be termed cirrhosis rather than hepatitis, as this term more appropriately describes the deranged liver lobe architecture. Macroscopically, the liver is small and has a smooth or finely granular surface.
Symptoms
Lobular dissecting hepatitis can be associated with weight loss, vomiting and polyuria, which can be followed by ascites and HE.
Diagnosis
The abdominal fluid from dogs with lobular dissecting hepatitis is usually clear and colorless, but can also be yellow in icteric patients. A serum chemistry profile may or may not show elevated liver enzyme activities, but bile acids concentrations are usually elevated. Plasma ammonia concentration may also be elevated and the ammonia tolerance test is abnormal in most patients.
Liver biopsy is diagnostic for lobular dissecting hepatitis and reveals characteristic histological changes. Percutaneous liver biopsy with a Menghini needle is usually difficult (i.e., these patients have a small, firm liver that “floats” away in the ascites fluid), so that an ultrasound-guided biopsy with a biopsy gun may be necessary.
Management
The management of lobular dissecting hepatitis is similar to that of chronic hepatitis. However, the prognosis of this condition is much worse than that of chronic hepatitis.
7.5.1.5 Nonspecific reactive hepatitis
Pathogenesis
Nonspecific reactive hepatitis describes a condition that is characterized by focal or diffuse hepatic damage with a secondary inflammatory reaction resulting from toxemia or sep- sis.5, 10 Reactive hepatitis can occur in every patient with toxemia, sepsis, inflammation, or a necrotizing process (including tumor necrosis). When such a process is located in the drainage area of the portal vein, all of the toxins are transported to the liver. In addition, generalized sepsis may also cause this form of hepatitis. Reactive hepatitis develops in most cases of gastroenteritis as a result of increased hepatic toxin absorption. It also develops in patients with peritonitis and other inflammatory diseases of organs that are drained by the portal vein.
Dogs with chronic diarrhea as the major clinical sign usually do not have primary liver disease, but rather a primary intestinal disease with a secondary reactive hepatitis. In contrast, vomiting is a common clinical sign in patients with either primary hepatobiliary disease or primary GI disease. It is important, therefore, to carefully take a history, as this may give clues to decide whether the patient has a primary intestinal or hepatic disease.
Circulating toxins, inflammatory mediators, and bacteria cause a proliferation of the reticuloendothelial system and also an infiltration of the liver with neutrophils. Focal hepatic necrosis can also occur. In chronic cases, there is also a component of lymphocytic and plasmacytic infiltration. Reactive hepatitis can also be associated with mild to severe cholestasis of the canaliculi. In some cases that are associated with sepsis, diffuse foci of necrosis, microabscesses, or granulomas can be seen (e.g., Herpes canis infection, toxoplasmosis, brucellosis, tuberculosis, E. coli infection, or migrating larvae of Toxocara canis). Continuous Toxocara canis infestation can cause a diffuse granulomatous eosinophilic inflammatory reaction. Hematologi- cally, peripheral eosinophilia may also occur in such cases.
The type of inflammatory cells in patients with secondary nonspecific reactive hepatitis (i.e., predominantly neutrophils and sometimes eosinophils) are different from those in patients with primary chronic active hepatitis (i.e., lymphocytes and plasma cells). Also, the localization of the inflammatory reaction within the liver is different with a diffuse distribution in patients with secondary reactive hepatitis and a portal or periportal distribution with primary chronic hepatitis.
Symptoms
The clinical symptoms seen in patients with secondary reactive hepatitis are often determined by the primary disorder. Thus, most patients with reactive hepatitis have diarrhea. In patients with sepsis, fever may also be present. Severe reactive hepatitis may also cause icterus.
Diagnosis
A definitive differentiation between primary hepatitis and secondary reactive hepatitis is only possible by the histological examination of liver tissue.
Therapy
As hepatic functions remain well preserved, there is no specific therapy for reactive hepatitis. If reactive hepatitis is diagnosed, the clinician should search for the underlying primary disease process. After the underlying cause of the reactive hepatitis has been successfully treated, the liver will recover spontaneously within a period of about three weeks.
7.5.2