PATHOPHYSIOLOGIC DERANGEMENTS OCCURRING WITH HEPATIC DISEASE
Bile Pigment Metabolism
Bilirubin Metabolism
Hepatobiliary excretion of bilirubin requires adequate uptake, conjugation, and secretion by the hepatocyte. Hepatic failure leads to hyperbilirubinemia and icterus.
Bilirubin is formed primarily from breakdown products of red blood cells, from other hemoproteins, and other enzymes such as the cytochromes. Red blood cells have a finite life span (usually 120 days in the dog, 90 days in the cat), after which they are removed from the circulation by the body's reticuloendothelial system (especially in the spleen and liver). In the Kupffer's cells of the liver, senescent red blood cells are degraded to free hemoglobin. Similarly, circulating hemoglobin bound to several carrier proteins is phagocytized by Kupffer's cells. The enzyme heme oxygenase catabolizes hemoglobin to biliverdin, which is then converted to bilirubin by the enzyme biliverdin reductase. This lipid- soluble free bilirubin crosses the cell membrane and is released into the circulation, where it is bound to albumin. This circulating complex (termed unconjugated or indirect bilirubin) is eventually actively taken up by hepatocytes. Bilirubin is then bound to intracellular carrier proteins and undergoes conjugation, primarily with glucuronide. Conjugated bilirubin (also called direct bilirubin) is secreted into the bile canaliculus and transported to the gallbladder for storage.There must be considerable hepatocellular disease or increase in the bilirubin load (hemolysis) to result in hyperbilirubinemia, because the liver's reserve capacity for bilirubin processing is up to 30 times the normal bilirubin load. Therefore the serum bilirubin concentration is an insensitive indicator of hepatocellular function, only increasing with severe hepatocellular disease. In general, total bilirubin concentrations above 2 to 3 mg/dl are detectable clinically as jaundice, whereas concentrations above 0.6 to 0.8 mg/dl result in abnormal bilirubinuria and spun serum or plasma to be visibly icteric.
Because unconjugated bilirubin circulates in plasma bound to albumin, it does not undergo glomerular filtration and does not appear in the urine (unless there is coexisting glomerular disease). Conjugated bilirubin, however, is freely filtered and appears in the urine and is readily detected with urine dipsticks. The dog has a very low renal threshold for conjugated bilirubin excretion; thus urine concentration of bilirubin increases far more readily than plasma concentration. It is normal to find a small amount of bilirubin in the urine of dogs, especially in a concentrated sample. Therefore there must be a considerable increase in the bilirubin load to increase plasma concentrations. Slight elevations in plasma bilirubin are significant, suggesting hepatobiliary disease. In the cat the renal threshold is much higher, so the finding of any degree of bilirubinuria is always abnormal. Renal tubular cells of the dog also possess a limited ability to convert hemoglobin into unconjugated bilirubin, which then appears in the urine. This can thus account for some of the bilirubinuria that occurs with hemolytic disease.
Hyperbilirubinemia is categorized into prehepatic, intrahepatic, and posthepatic causes. Prehepatic hyperbilirubinemia occurs when production exceeds the liver's capacity for metabolism and secretion. Causes of this include immune-mediated hemolytic anemia, heavy metal toxicity (lead, copper), and methylene blue toxicity. There will be evidence on the hemogram of increased production of bilirubin, with the most notable change being a decreased hematocrit.
Intrahepatic causes of hyperbilirubinemia occur when there is abnormal hepatic uptake, conjugation, or secretion of bilirubin. In most hepatocellular diseases there is usually coexisting impairment of bilirubin uptake, conjugation, and secretion. Therefore there is usually a mixture of conjugated and unconjugated hyperbilirubinemia. The increase in conjugated bilirubin results from impaired bilirubin secretion from damaged hepatocytes or from impairment of bile flow through bile canaliculi due to hepatocyte swelling, inflammation, or fibrosis.
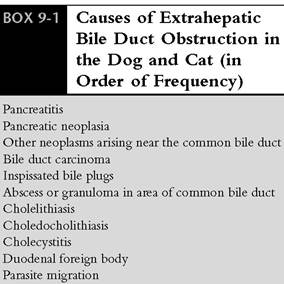
The increase in unconjugated bilirubin results from coexisting impairment of hepatic uptake and conjugation or from deconjugation of conjugated bilirubin by lysosomal enzymes released from injured hepatocytes or by inflammatory cells invading the liver. Therefore there can be an increase in primarily unconjugated bilirubin, conjugated bilirubin, or a mixture of both depending on the nature of the intrahepatic lesion.Intrahepatic or extrahepatic biliary obstruction causes posthepatic hyperbilirubinemia. When this occurs, conjugated bilirubin is regurgitated into the systemic circulation, so that there is primarily a conjugated hyperbilirubinemia. However, there can also be concurrent unconjugated hyperbilirubinemia with posthepatic causes. This can result from deconjugation of bilirubin by damaged hepatocyte lysosomal and inflammatory cell enzymes (bile is hepatotoxic and cholestasis results in secondary hepatocellular damage and inflammation) or because conjugated bilirubin once absorbed into the systemic circulation recirculates and competes with unconjugated bilirubin for uptake by hepatocytes. The causes of extrahepatic biliary obstruction are listed in Box 9-1.
The relative increases of conjugated or unconjugated bilirubin are variable with all three general categories of hyperbilirubinemia and therefore do not aid the clinician in localizing the nature of the lesion. Ultrasonography, laparoscopy, and laparotomy localize the cause of hyperbilirubinemia.
288 chapter 9 I DiseasesoftheliverandhepatobiliarySystem
Delta-Bilirubin. Delta-bilirubin is a novel form of bilirubin first noticed when the sum of conjugated and unconjugated bilirubin was less than the total bilirubin concentration when measured by high-performance liquid chromatography. The difference has been attributed to conjugated bilirubin covalently bound to albumin, subsequently called delta-bilirubin.
This form of bilirubin is mainly seen with cholestatic hepatic diseases. The life span of delta-bilirubin is dependent on the half-life of albumin (approximately 14 days).Because of the strong covalent bond to albumin, delta-bilirubin does not appear in the urine or have significant hepatocellular uptake. Thus, because of these features and the long half-life of albumin, delta-bilirubin remains elevated even after cholestasis is completely resolved. There is marked variability in the amount of delta-bilirubin among dogs. This explains the persistent elevation in total bilirubin concentration (and clinical icterus) following surgical correction of biliary obstruction in some patients. The finding of increased total bilirubin concentration without concurrent hyperbilirubinuria suggests the presence of delta-bilirubin (excluding artifact). In these patients resolution of bilirubinuria may be the best marker of resolution of cholestasis.Bile Acid Metabolism and Pathophysiology
Bile is composed of bile acids (salts), bile pigments (primarily bilirubin), cholesterol, phospholipids (primarily lecithin), and hepatic enzymes (such as alkaline phosphatase). Of these, bile acids are the most abundant and are the major solute in bile, constituting three fourths of the total solids. They are synthesized in the liver as a result of cholesterol metabolism and secreted into the bile. Feeding is a normal stimulus for bile acid secretion. They enter the intestine and undergo an efficient entero- hepatic circulation following passive and active absorption from the ileum. Both unaltered bile acids and those deconjugated and dehydroxylated by intestinal bacteria are reabsorbed and enter the enterohepatic circulation. They are efficiently removed by the liver, reconjugated if necessary, and resecreted in bile. Hepatocellular uptake is a highly efficient process with large excess capacity, operating far from saturation under physiologic conditions. During a typical meal the total bile acid pool is recycled two to three times through this entero- hepatic pathway.
Only small amounts of bile acids are lost in the feces. Normally the liver synthesizes enough bile acids to compensate for fecal losses, which are minimal with respect to the total bile acid pool. Although bile acid formation depends on hepatic synthesis, the liver reserve capacity for this is never exceeded because of the small amounts needed for physiologic purposes.Fecal loss of bile acids represents the major pathway for cholesterol excretion from the body. In addition to their role in lipid absorption, bile acids also stimulate pancreatic enzyme release and activity.
Factors important in governing bile acid metabolism include hepatic function, the portal blood supply, the small intestine, intestinal bacteria, and dietary factors. The pathophysiologic effects of bile acids are hepatotoxicity, gastric hyperacidity, and diarrhea.
Abnormal hepatic function, biliary excretion, or portal circulation can interrupt the normal enterohepatic circulation and lead to an increase in serum bile acid concentration. This occurs with many hepatobiliary diseases. When the liver parenchyma is diseased, the inability of normal uptake, conjugation, and secretion results in decreased extraction of bile acids from the portal circulation and leads to increased systemic concentrations. With intrahepatic or posthepatic cholestasis, bile acids diffuse from bile into the systemic circulation in a manner similar to that of bilirubin. With portosystemic shunting (either congenital or acquired), the enterohepatic circulation is directly interrupted and bile acids fail to be extracted by the bypassed liver. In this setting, hepatic synthesis of bile acids continues in order to maintain a normal bile acid pool. This can result in tremendous increases in systemic concentrations, especially following feeding. As will be discussed in the section on laboratory evaluation of hepatic disease, serum bile acid concentrations represent a sensitive indicator of hepatic function.
Protein Metabolism
Albumin Metabolism
Albumin is an important protein synthesized by the liver that is important in many homeostatic functions, such as maintenance of plasma colloid oncotic pressure and as a plasma transport carrier for many electrolytes, hormones, pigments, and drugs.
Albumin represents approximately 25% of all the proteins synthesized by the liver. Because albumin has a relatively high priority for synthesis, the synthesis of other proteins will decrease before that of albumin with hepatocellular disease or with protein-calorie malnutrition.Albumin concentration decreases with severe hepatic disease because of decreased synthesis and because ammonia (when elevated with hepatic disease) inhibits albumin release from hepatocytes. In addition, the abnormal insulin and glucagon concentrations that occur with hepatic disease also result in inhibition of albumin release from hepatocytes. Also, when ascites is present, there is an increased volume of distribution of albumin.
Clotting Factors
The liver is responsible for synthesizing many of the clotting factors, including factors I, II, V, VII, IX, and X. The liver also synthesizes activators and inhibitors of the fibrinolytic system (such as antiplasmins). In addition, the liver is involved in the synthesis, catabolism, and clearance of both procoagulants and anticoagulants (such as antithrombin III, fibrin degradation products, and plasminogen activators). With hepatic disease, derangements of these processes can lead to a variety of hemostatic abnormalities. Causes of coagulopathies associated with hepatic disease are listed in Box 9-2.
Although spontaneous bleeding in patients with hepatic disease is unusual, excessive bleeding following surgical trauma or liver biopsy may occur. In clinical cases of hepatic disease, there may be multiple abnormal hemostatic tests. Prothrombin time, partial thromboplastin time, and activated clotting time can be prolonged with hepatic failure because of lack of synthesis of clotting factors. This usually occurs with massive
BOX 9-2
Causes of Coagulopathies With Hepatic Disease
Decreased synthesis of clotting factors Disseminated intravascular coagulation (DIC)
Decreased antithrombin III synthesis
Excessive fibrinolysis (decreased antiplasmin synthesis, decreased clearance of plasminogen activator)
Circulating anticoagulants normally removed by the liver remain elevated, such as fibrin degradation products (FDPs)
Decreased vitamin K availability
Increased tissue thromboplastin with massive hepatic destruction
Abnormal platelet function acute hepatic necrosis and with cirrhosis. In a published study, dogs with chronic hepatitis that died within 1 week of presentation had significantly prolonged prothrombin and partial thromboplastin time compared with dogs that survived.
Decreased absorption of fat-soluble vitamin K leads to prolongation of clotting times. This cofactor is necessary for the hepatic synthesis and activation of factors II, VII, IX, and X. Chronic biliary obstruction can cause vitamin K malabsorption. However, intestinal bacteria synthesize vitamin K, making a deficiency of this vitamin a less common cause of bleeding during hepatic disease (unless the use of long-term intestinal antibiotics decreases bacterial vitamin K synthesis). If clotting times are prolonged, administration of parenteral vitamin K1 followed by normalization of clotting times within 24 hours confirms vitamin K deficiency as a contributor to the coagulopathy. Recently reported studies in dogs and cats using the PIVKA test (proteins induced by vitamin K antagonism/absence) suggest that this test is the most sensitive in detecting coagulopathies in patients with hepatic disease. In these studies the PIVKA test was more than twice as sensitive in detecting coagulopathies in dogs and more than three times as sensitive in detecting coagulopathies in cats compared with routine coagulation tests (prothrombin time, activated partial thromboplastin time).Vitamin K administration may be helpful in certain situations. In one report, Vitamin K administration improved PIVKA times in 10 of 23 dogs with hepatic disease and normalized PIVKA times in 12 of 48 cats. It has been my experience that bleeding following hepatic biopsy does not correlate with coagulation findings, including the PIVKA test. Patients with coagulopathies are no more likely to bleed than patients without coagulopathies. In most cases of significant bleeding following hepatic biopsy, there are technical problems. In my experience, the rapidity of bleeding and/or necropsy examination suggest that a large vessel has been damaged rather than hemorrhage being due to persistent oozing from needle biopsy sites. The exception to this is that patients with disseminated intravascular coagulation (DIC) often have significant hemorrhage regardless of biopsy technique used. Controlled studies in veterinary patients will be necessary to make final conclusions regarding postbiopsy hemorrhage in the patient with a coagulopathy.
DIC is the most common coagulopathy occurring with hepatic disease in my experience and the one most likely to result in hemorrhage following hepatic biopsy. Thrombosis and hemorrhage are both potential sequellae of DIC. DIC can result from decreased hepatic synthesis of antithrombin III, decreased clearance of activated clotting factors, and increased release of tissue thromboplastin associated with massive hepatic destruction. These mechanisms may be further complicated by events leading to excess fibrinolysis. The latter situation can occur from excessive activity of the fibrinolytic enzyme plasmin (occurring because of increased plasminogen activator and decreased antiplasmin concentrations). The net result of excessive fibrinolysis is the formation of fibrin degradation products (FDPs), which have potent anticoagulant effects and are not cleared efficiently by a diseased liver. Laboratory test results suggesting the presence of DIC include prolongation of prothrombin, partial thromboplastin, and thrombin times, thrombocytopenia, elevated FDPs, hypofibrinogenemia, and schisto- cytosis.
Abnormal platelet function can also occur with hepatic disease. These defects may be evaluated by platelet aggregation studies, but these studies are not routinely performed in clinical patients because of the lack of equipment availability. Platelet function defects may explain bleeding tendencies in patients with normal coagulation tests. Platelet function can be estimated by evaluating toenail or lip bleeding time.
Spontaneous hemorrhage is unusual with hepatic disease with the exception of gastrointestinal (GI) hemorrhage. The latter can result from increased gastrin concentration (due to decreased hepatic clearance of gastrin and increased gastrin release stimulated by elevated bile acid concentrations), which causes an increase in gastric acid production. In addition, DIC can lead to abnormal GI mucosal microcirculation due to microthrombi formation, thus decreasing the ability of the mucosa to withstand injury. One of the consequences of GI hemorrhage is exacerbation of hepatic encephalopathy because blood is a substrate for ammonia production in the large intestine. In addition, GI hemorrhage can result in partial depletion of clotting factors, and, when reduced further by hepatic biopsy, massive or prolonged bleeding can result.
When evaluating patients with hepatic disease for hemostatic abnormalities, the clinician must be aware of the relative insensitivity of clotting times. These times are prolonged only when coagulation factors are reduced to 30% of normal. In addition, multiple defects may be present, some of which are not detected by routine coagulation tests, such as abnormal platelet function and excessive fibrinolysis. Sudden demand for clotting factors, as would occur following hepatic biopsy or laparotomy, may precipitate massive or prolonged hemorrhage in a patient with normal coagulation test results. Because the exact nature of the defect is often unknown or multifactorial, treatment with fresh whole blood collected in a plastic blood collection bag (to preserve platelet activity and prevent activation of factor XII) is usually indicated to treat these patients. If possible, efforts such as this should be taken before hepatic biopsy to correct a known coagulopathy.
Ammonia Metabolism
Ammonia has long been considered one of the most important encephalopathic toxins in patients with hepatic disease. The most important source of ammonia is the large intestine, where intraluminal bacteria convert proteins and other nitrogen-containing compounds to ammonia. Once the ammonia is absorbed into the portal circulation, the liver normally extracts most of it, converting it to urea via the urea cycle. Hepatic failure results in increased blood ammonia and decreased blood urea nitrogen (BUN) concentrations.
Gram-negative enteric bacteria are quantitatively the most important organisms for converting nitrogenous substrates to ammonia, although certain anaerobes are also capable of synthesizing ammonia. Dietary proteins are the most important substrate for ammonia production, but other substrates such as urea (which freely diffuses from the systemic circulation into the colon), sloughed intestinal epithelial cells, and GI hemorrhage are also quantitatively important. Therefore reduction of these substrates and of large intestinal bacterial numbers will have a beneficial effect on ammonia absorption. Treatment measures used to decrease ammonia absorption are discussed in the section on management of hepatic disease.
Portal blood in the dog normally contains approximately 350 μg∕dl of ammonia (and about double this in the cat because of the higher dietary protein content of this species). The liver is normally able to extract approximately 85% of this, resulting in a systemic venous ammonia concentration of approximately 50 μg∕dl (± 30 μg∕dl). Because the liver has a large capacity for ammonia removal, there must be considerable hepatic dysfunction or abnormal portal circulation to raise systemic plasma concentrations. The normal liver can tolerate up to twice the normal ammonia load. This degree of tolerance can be a sensitive indicator of hepatic function and is used clinically when performing the ammonia tolerance test.
Hepatic Encephalopathy
Hepatic encephalopathy is defined as a clinical syndrome characterized by abnormal mental status occurring in patients with severe hepatic insufficiency. This can result from primary hepatocellular disease or from portosystemic shunting of blood away from the liver. Clinical signs in patients with this condition include a wide variety of behavioral changes, ranging from only mild depression and anorexia to coma. Many signs are nonspecific and can be seen with a wide variety of unrelated disorders. These include depression, anorexia, vomiting, diarrhea, polydipsia, and polyuria. Neurologic signs are also common. These signs are variable and often cannot be localized to a specific anatomic lesion.When this occurs, or when the nature of the neurologic abnormalities vary with time, hepatic encephalopathy should be considered as a cause. The most common neurologic manifestation is decreased mentation and responsiveness. Often patients will appear confused, have compulsive pacing and wandering, and appear transiently blind. Some patients will have abnormal patterns of urination and defecation and appear no longer housebroken. Signs can progress to include seizures, severe dementia, and coma. The severity of these signs often wax and wane, sometimes in response to feeding, but do not always correlate with the severity of the hepatic lesion.
Etiology of Hepatic Encephalopathy Several factors have been implicated in contributing to hepatic encephalopathy. Most of these factors relate to an accumulation of neurotoxic substances that have not been metabolized properly by the liver, including ammonia, benzodiazepine-like substances, amino acids, mercaptans, and fatty acids. Other causes include changes in the blood-brain barrier, abnormal neurotransmitter balance, abnormal cerebral metabolism, and metabolic abnormalities.
There is experimental and clinical evidence that hepatic encephalopathy is multifactorial. The concentrations of ammonia, mercaptans, and free fatty acids necessary to produce coma individually are much higher than when more than one or all are elevated. Both mercaptans and free fatty acids will increase ammonia concentration. Likewise hyperammonemia will contribute to amino acid imbalances. In addition to the synergistic effects of encephalopathic toxins, metabolic derangements augment these effects. These changes include azotemia, hypoxia, electrolyte imbalances, hypoglycemia, tranquil- ization, alkalosis, and hypovolemia. Patients with these derangements are more likely to develop encephalopathy, and correction of these derangements will significantly improve the encephalopathic state. For example, the hypokalemia that frequently accompanies hepatic failure is one of the most common metabolic derangements that contribute to depression and anorexia.With potassium supplementation there is often dramatic clinical improvement in appetite and attitude. Factors that can precipitate metabolic changes that lead to encephalopathy include increased dietary protein intake, GI hemorrhage, diuretic administration, sedative administration, uremia, infection, constipation, large intestinal bacterial overgrowth, and methionine administration.
The importance of synergistic effects and multiple interactions of encephalopathic factors help explain the different clinical presentations and severity of encephalopathy with varying blood concentrations of encephalopathic toxins. It also explains the occurrence of encephalopathy in the absence of a striking abnormality in any single factor, including ammonia concentration. The therapeutic manipulations of all these factors represent the cornerstone of symptomatic management of hepatic encephalopathy. These will be discussed in the section on management of hepatic disease.
Ascites and Portal Hypertension
Ascites (the accumulation of free fluid in the peritoneal cavity) is a common sign of hepatic disease and occurs as a result of chronic portal hypertension, hypoalbuminemia, and increased renal salt and water retention. The development of ascites occurs when there is an alteration of Starling’s forces, including increased venous or lymphatic hydrostatic pressure, decreased capillary oncotic pressure, increased vascular permeability, and increased intraperitoneal oncotic pressure.
Portal hypertension is one of the most important factors leading to the development of ascites in patients with hepatic disease. Portal hypertension can be caused by increased total portal blood flow; increased resistance to portal, intrahepatic, or posthepatic blood flow; or a combination of these changes. The most common cause of portal hypertension is cirrhosis, resulting in increased resistance in sinusoidal vessels caused by swelling of hepatocytes or fibrosis around sinusoids causing postsinusoidal outflow block. The combination of increased portal pressure and blood flow causes an increase in hepatic lymph formation.When this is excessive, ascites results. Another common effect of chronic portal hypertension is the development of acquired portosystemic shunts.Unlike congenital portosystemic shunts, acquired shunts are usually multiple, extremely tortuous, and variable in their location.
It was formerly thought that portal hypertension and hypoalbuminemia initiate ascites formation. This results in decreased effective circulating plasma volume. The compensatory response to this is renal conservation of fluid and electrolytes, mediated by changes in renal blood flow, glomerular filtration rate, and activation of the renin- angiotensin-aldosterone axis. This retention of salt and water perpetuates the problem by leading to increased splanchnic lymph and portal blood flow.
However, more recent evidence contradicts this theory and suggests that the renal mechanisms leading to retention of water and electrolytes are the primary initiating events in the formation of ascites with hepatic disease. In this setting there is renal salt and water retention before the development of ascites, thus expanding the circulating plasma volume and contributing to the development of portal hypertension. Eventually portal hypertension leads to the development of ascites, with hypoalbuminemia continuing to perpetuate it. Factors that may initiate renal salt and water retention include increased sensitivity to aldosterone and failure to release or respond to natriuretic hormone in response to an expanded circulating plasma volume. The latter situation results in the inability to excrete a salt and water load in response to volume expansion. In addition, the normal negative feedback system that governs the renin-angiotensin-aldosterone system does not shut off and reduce aldosterone secretion in the presence of portal hypertension and ascites. This is because the high concentrations of aldosterone do not return effective circulating plasma volume to normal in the presence of ascites, despite the retention of sodium. Because of these mechanisms, therapeutic interventions for managing ascites include salt restriction and inhibition of the renin-angiotensin-aldosterone axis with drugs such as spironolactone, enalapril, and benazepril. This will be discussed in the section on management of hepatic diseases.
The presence of ascites acts to increase albumin’s volume of distribution, which lowers blood albumin concentration. This lowers plasma oncotic pressure and exacerbates the formation of ascitic fluid. The presence of portal hypertension is necessary for the development of ascites and leakage of albumin into the abdominal cavity. In this setting, ascites is present when plasma albumin concentrations are higher than when ascites can be attributed to hypoalbuminemia alone.With normal portal pressure, plasma albumin concentration must be below approximately 1.5 g/dl to result in ascites, as occurs with GI or renal protein loss. When this occurs, subcutaneous edema often predominates over ascites.
Other Metabolic Abnormalities
Carbohydrate Metabolism
The liver plays a central role in carbohydrate metabolism. It is the primary organ for glucose storage (converting glucose by glycogenic enzymes) and also provides glucose during fasting (through glycogenolysis). When there are inadequate stores of glycogen, as might occur with hepatic disease, the glucose need is supplied through catabolism of muscle proteins to amino acids and conversion to glucose via gluconeogenic pathways. This causes muscle wasting and increases the nitrogen load and aggravates hyperammonemia. Because of the importance of gluconeogenesis in the liver for maintaining blood glucose concentrations, complete hepatectomy rapidly results in death from hypoglycemia.
Hepatic failure can result in either preprandial hypoglycemia or postprandial hyperglycemia. Loss of approximately 70% of the hepatic mass may cause fasting hypoglycemia because of inadequate glycogen storage and gluconeogenesis. Additional causes of hypoglycemia include congenital deficiency of glycogen-metabolizing enzymes (as occurs with glycogen storage diseases), tumor hypoglycemia, and portosystemic shunts (associated with decreased hepatic mass and lack of tropic portal blood to the liver). In patients with hypoglycemia associated with hepatic disease, it is usually easy to get the blood glucose concentration into the normal range with intravenous glucose supplementation, in contrast to patients with insulin-producing tumors in which it can be very difficult to get the blood glucose concentration into the normal range despite aggressive intravenous glucose administration.
Causes of postprandial hyperglycemia with hepatic disease include deficient hepatic enzymes to handle the carbohydrate load, leading to inadequate glycogenesis, and increased plasma concentration of glucocorticoids (because of decreased hepatic clearance).
Fibrinogen
Fibrinogen is a protein that is synthesized by the liver. Synthesis of fibrinogen is diminished only in the late stages of severe hepatic failure. Other factors are usually more important in determining fibrinogen concentration than the rate of hepatic synthesis. Factors that will more commonly lead to decreased fibrinogen concentration include increased fibrinogen consumption, as occurs with DIC or primary fibrinolysis. Factors that result in increased fibrinogen concentration include inflammatory diseases (involving or not involving the liver) and major surgery. In this setting there is increased synthesis and release by the hepatocyte.
Drug and Hormone Metabolism
The microsomal enzyme system of the liver is important for drug and hormone metabolism. Hepatic failure can result in abnormally delayed drug metabolism and clearance. In addition, drugs that are highly protein bound can have increased biologic effects when there is hypoalbuminemia associated with hepatic disease. In this setting there is less albumin to bind to the drug and therefore more unbound (active) drug to exert its effects. Therefore drugs that undergo hepatic clearance or that are highly protein bound should be administered with caution in patients with hepatic failure.
Many hormones are metabolized by the liver and can be abnormally elevated with hepatic disease. The more important hormones to have prolonged clearance are the steroid hormones, including cortisol, estrogens, androgens, and progesterones. As with many drugs, the degree of protein binding and therefore the concentration of unbound, active hormone can be altered with hypoalbuminemic states. Other hormones that undergo altered metabolism in patients with hepatic disease include insulin, glucagon, thyroxine, pituitary hormones, gastrin, and aldosterone. Many of these alterations were discussed in reference to their specific physiologic effects.
Reticuloendothelial System Function
The reticuloendothelial system (RES) removes toxic or foreign substances, cellular debris, bacteria, drugs, and endotoxins from the blood. The hepatic RES is more important than that in the rest of the body for appropriate processing of these materials. Primary hepatocellular disease or portosystemic shunting (either congenital or acquired) can cause failure of the hepatic RES. With hepatic disease other tissues with RES activity can only partially compensate for the diminished hepatic RES function. Deficiencies of specific roles of the hepatic RES function can lead to characteristic changes that other RES tissues cannot compensate for. The liver is directly responsible for clearing absorbed GI products, because they pass through the liver before gaining access to the systemic circulation. These products include intestinal bacteria, endotoxins, and GI mucosal antigens. The effects of decreased clearance of GI products can be the systemic access of bacteria or their toxins, resulting in potential sepsis and/or endotoxemia. In addition, there can be positive bacterial growth from hepatic biopsy specimens even when the underlying cause of hepatic disease is not bacterial in origin. In my experience it is not unusual to culture Escherichia coli or other enteric bacteria from hepatic biopsy specimens obtained from patients with various hepatic diseases.
One of the consequences of abnormal exposure of GI antigens to the systemic circulation is the development of hyperglobulinemia. These immunoglobulins are produced by nonhepatic tissues in response to the systemic antigen load. Another potential source of hyperglobulinemia occurring with hepatic disease is the release of antigens from injured hepatocytes. Many of the intracellular structures of the hepatocyte, especially the nucleus and mitochondria, are recognized as foreign and elicit an immune response characterized by an influx of lymphocytes and plasma cells. The effects of this cellular infiltration include the potential for further hepatocyte damage and thus perpetuate a vicious cycle (this will be discussed further in the section on chronic active hepatitis). In addition, the plasma cells will manufacture gamma globulins, which lead to a hyper- globulinemia.
Loss of Compartmentalization Function
The maintenance of the integrity of the hepatocyte membrane is an important function. Any insult that damages the cell membrane can lead to loss of intracellular contents, including organelles, enzymes, and antigens. In addition to loss of intracellular contents, hepatocyte function may be compromised.
Loss of intracellular enzymes (with the exception of certain proteases) does not lead to abnormal function or clinical signs but can be a useful laboratory test for diagnostic purposes. Those enzymes that leak into plasma following increased hepatocellular membrane permeability include alanine aminotransferase (ALT, formerly glutamic- pyruvic transaminase [GPT]), aspartate aminotransferase (AST, formerly glutamic-oxaloacetic transaminase [GOT]), arginase, sorbitol dehydrogenase (SDH), lactic dehydrogenase (LDH), and ornithine carbamoyltransferase (OCT). Enzyme activities that increase with biliary obstruction include alkaline phosphatase (ALP), gamma glutamyl transpeptidase (GGT), and 5'- nucleotidase.