diagnostic EVALUATION OF HEPATIC DISEASE
Historical Findings
Historical findings in patients with hepatic disease are often vague and nonspecific. In patients with toxic hepatopathies, there may be a history of exposure to known hepatotoxins, including corticosteroids, anticonvulsants, thiacetarsemide, mebendazole, acetaminophen, or certain chemicals.
Clinical signs associated with hepatic disease are listed in Box 9-3. The most common signs in cats with hepatic disease are nonspecific, including lethargy and inappetence. In some patients manifesting neurologic signs, signs may be precipitated by eating (especially high-protein meals), thus suggesting hepatic encephalopathy as the cause. This historical finding is often absent, however, even in severe cases of hepatic failure, including terminal hepatic cirrhosis and portosystemic shunts. The presence of signs and laboratory abnormalities suggestive of hepatic disease in certain breeds may suggest diseases for which these breeds are predisposed, such as copper-storage disease in the Bedlington terrier, West Highland white terrier, and possibly Doberman pinscher.Physical Examination Findings
Physical examination findings in patients with hepatic disease are often variable and nonspecific. The findings most suggestive of hepatic disease include icterus, ascites, and abnormal hepatic size. However, these signs may be seen in other diseases unrelated to the liver.
| BOX 9-3 | Clinical Signs Associated With Hepatic Disease | |
| Depression | Acholic feces | Behavior changes |
| Lethargy | Dark or orange urine | Dementia |
| Anorexia | Jaundice | Other neurologic disturbances |
| Vomiting | Petechiae | Polyuria |
| Diarrhea | Bleeding tendencies | Polydipsia |
| Weight loss | Melena | Ascites |
Icterus
Prehepatic causes of increased bilirubin concentration, such as immune-mediated hemolytic anemia, can result in icterus (jaundice).
The presence of icterus in a patient without anemia is diagnostic of hepatic or posthepatic biliary disease. The clinical manifestation of icterus usually occurs when serum total bilirubin concentration reaches 2 to 3 mg/dl, although this varies with the individual. Mucous membranes and skin appear yellow at lower serum bilirubin concentration if most is present in the conjugated state. The sclerae, soft palate, area under the tongue, and penis are usually the most sensitive areas to look for icterus. The magnitude of elevation in bilirubin concentration does not always correlate with the intensity of icterus observed on physical examination. Likewise, it can take several days for icterus to resolve following return of serum bilirubin to normal. This is especially true following resolution of biliary obstruction due to the presence and persistence of delta-bilirubin (see earlier section on pathophysiologic derangements occurring with hepatic disease).Ascites
Portal hypertension, hypoalbuminemia, and renal retention of salt and water cause ascites in patients with hepatic disease. It is important to consider other causes of ascites in the differential diagnosis, including right-sided heart failure, pericardial disease, hypoalbuminemia resulting from nonhepatic causes, abdominal neoplasia, heartworm disease, pancreatitis, increased lymphatic or vascular permeability, and certain infectious diseases (such as feline infectious peritonitis and abdominal abscesses). The presence of ascites can be confirmed with radiography, ultrasonography, or abdominal paracentesis. Subsequent fluid analysis is helpful to rule out many of the disorders mentioned above.
Abnormal Hepatic Size
Hepatomegaly may be detected on physical examination, but normal or small hepatic size cannot be palpated. Causes of increased hepatic size include neoplasia, passive congestion (secondary to rightsided heart failure), increased corticosteroid concentration (exogenous or endogenous), lipid accumulation (diabetes mellitus, feline hepatic lipidosis, other metabolic abnormalities), diffuse inflammation, glycogen storage diseases, hepatic abscess, hepatic or biliary cyst, or liver lobe torsion.
Puppies and kittens normally have a larger liver relative to their body size than adults. Causes of decreased hepatic size include portosystemic shunts (congenital or acquired), cirrhosis, or hepatic necrosis. Apparent decreased hepatic size may also be normal in some patients.Laboratory Evaluation of Hepatic Disease
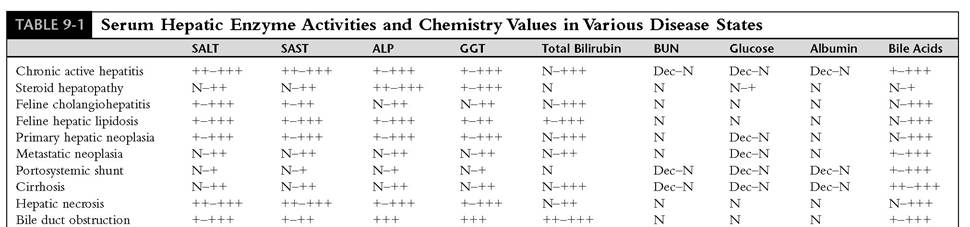
Laboratory tests are often essential to identify that hepatic disease exists, to assess its severity, and to monitor progression. An understanding of the pathophysiology of hepatic disease is necessary to interpret laboratory test results and to make clinical decisions regarding further diagnostic efforts and patient management. No laboratory test identifies a specific problem, helps determine specific therapeutic management, or predicts outcome. This is because different diseases produce similar alterations in hepatic function or in laboratory test results. Biochemical tests usually determine the liver's excretory or functional ability or measure the integrity of the hepatocyte by virtue of leakage of intracellular enzyme systems. Once biochemical tests identify that hepatic disease exists, the diagnosis must be pursued with a morphologic diagnosis obtained by biopsy specimen analysis. Results of laboratory tests in various disease states are summarized in Table 9-1.
Tests of Hepatic Function
Many biochemical tests are available to evaluate the liver's anabolic and/or catabolic functions and hepatic circulation. These include measurement of serum bile acid concentrations, plasma ammonia concentration, bile pigment (bilirubin) concentration, and the ability to excrete organic dyes. Hepatic function can be markedly abnormal despite maintenance of the hepatocellular membrane (and therefore normal serum activities of hepatic enzymes). Examples include portosystemic shunts, terminal cirrhosis, and metastatic hepatic neoplasia. Likewise, the liver can continue normal anabolic or catabolic function despite severe hepatocyte leakage of intracellular enzymes because of its marked reserve capacity.
For example, this situation can occur with certain cases of hepatocellular necrosis, primary hepatic neoplasia, or trauma.Serum Bile Acids
See the earlier section on pathophysiologic derangements occurring with hepatic disease for a detailed discussion of normal bile acid metabolism and changes occurring with hepatic disease. Briefly,
296 chapters ∣ DiseasesoftheliverandhepatobiliarySystem
SALT, Serum alanine aminotransferase; SAST, serum aspartate aminotransferase; ALP, serum alkaline phosphatase; GGT, gamma glutamyl transpeptidase; BUN, blood urea nitrogen; + mild increase; ++, moderate increase; +++, severe increase; Dec, deaease; N, normal.
bile acids are synthesized in the liver as a result of cholesterol metabolism and secreted into bile. Feeding is a normal stimulus for bile acid secretion. Bile acids enter the intestine and undergo an efficient enterohepatic circulation following active absorption from the ileum. Once absorbed, they are removed from the portal circulation by the liver and reexcreted into bile. During a typical meal, the total bile acid pool is recycled two to three times through this enterohepatic pathway. Only small amounts of bile acids are lost in the feces. Normally the liver synthesizes enough bile acids to compensate for fecal losses, which are minimal with respect to the total bile acid pool. Although bile acid formation depends on hepatic synthesis, the liver reserve capacity for this is never exceeded because of the small amounts needed for physiologic purposes. Thus measurement of bile acid concentration is a reliable test even in end-stage liver disease.
Abnormal hepatic function, biliary excretion, or portal circulation can interrupt the normal enterohepatic circulation and thus lead to an increase in serum bile acid concentration. This occurs with many hepatobiliary diseases.When the liver parenchyma is diseased, the abnormal uptake, conjugation, and secretion of bile acids result in decreased extraction from the portal circulation and lead to increased systemic concentrations.
With intrahepatic or posthepatic cholestasis, bile acids diffuse from bile into the systemic circulation in a manner similar to that of bilirubin. With portosystemic shunting (either congenital or acquired), the enterohepatic circulation is directly interrupted and bile acids fail to be extracted by the bypassed liver. In this setting, hepatic synthesis of bile acids continues in order to maintain a normal bile acid pool. This can result in tremendous increases in systemic concentrations, especially following feeding.Both solid-phase radioimmunoassay (RIA) and direct enzymatic spectrophotometric methods of bile acid determinations have been validated for the dog and cat. These methods have made serum bile acid determinations a routine part of evaluating hepatic function. In my laboratory, normal fasting concentrations are approximately 2.5 μmol∕L in the dog, and 1.5 μmol∕L in the cat. Two-hour postprandial concentrations rise to approximately 8.5 μmol∕L in the dog and cat. Serum is stable for measurement for several days at room temperature. Several artifacts can affect bile acid measurement. Moderate to marked lipemia artifactually increases the serum bile acid measurement determined by the enzymatic method but artifactually decreases the measurement when determined by the RIA method. Moderate to marked hemolysis artifactually decreases the serum bile acid value determined by the enzymatic method but probably does not affect the measurement determined by the RIA method. Bilirubin has little effect on the measurement of bile acid concentration unless the serum bilirubin concentration is greater than 5 mg∕dl, in which case there may be a small (less than 20%) decrease in measurement at low bile acid concentrations. If there is hyperbilirubinemia due to hepatic disease, measurement of serum bile acids is not indicated.
Bile acid measurements have certain advantages over other tests of hepatic function. They do not require the administration of exogenous compounds (such as sulfobromophthalein [BSP] and indocyanine green [ICG] dyes and oral ammonium chloride) or meticulous sample handling (as is required for plasma ammonia determination).
The indications for measuring serum bile acid concentrations include the identification of occult hepatic disease when enzyme determinations are normal (as can occur with portosystemic shunts, cirrhosis, and metastatic hepatic neoplasia), evaluation for the possibility of a portosystemic shunt in patients with suggestive symptomatology, monitoring of hepatobiliary function to assess progression of hepatic disease, and identification of abnormal hepatic function in patients in which enzyme activity elevations may be due to extrahepatic causes.
To maximize the diagnostic information from total serum bile acid measurement, both a 12-hour fasting and a 2-hour postprandial sample should be obtained. In general it is recommended that a normal-size meal be fed. However, minimum amounts of food that should be consumed have been established. Patients weighing 10 lb or less should be fed a minimum of 2 tsp, and those over 10 lb, 2 tbsp. Foods that are high in protein and fat should be fed because they most consistently challenge the bile acid enterohepatic circulation at the 2-hour postprandial level.
If inappetence is a problem, it may be necessary to force-feed the patient. For cats, special steps to avoid anorexigenic stimuli may be necessary (e.g., offer food in a quiet environment away from dogs, have the owner hand feed in a private area).
Warming the food may help coax an inappetent cat to eat.
In patients with encephalopathic tendencies, where there is concern about feeding high-protein foods, a low-protein meal may be fed. If vomiting is a problem and its frequency precludes feeding, initial testing is limited to a fasting sample. If the result is above normal, then a significant hepatic disorder remains a consideration. However, if the fasting sample is normal, liver disease cannot be ruled out.
Several studies have shown serum bile acid measurements to be a sensitive and specific indicator of hepatic function in the dog and cat. In dogs, fasting serum bile acid concentrations are significantly increased with congenital portosystemic shunts, glucocorticoid-induced hepatopathy, hepatic neoplasia, hepatitis, cholestasis, hepatic necrosis, and cirrhosis. Of these diseases, dogs with glucocorticoid-induced hepatopathy have the lowest increase in concentration of serum bile acids. Therefore marked increase in elevations (i.e., greater than 75 to 100 μmol∕L) are unlikely to be caused by glucocorticoid-induced hepatopa- thy. Although serum bile acid concentrations are a sensitive indicator of hepatic function, they do not distinguish the cause of the disease process. The magnitude of elevation in serum bile acid concentrations is weakly correlated with histologic severity. Furthermore, dogs with intestinal disease and normal hepatic function have normal serum bile acid concentrations. This is important in cases of “reactive hepatopathy” associated with intestinal or pancreatic disease. The determination of 2hour postprandial concentrations further increases the sensitivity of this test in most diseases and should be done routinely in conjunction with the preprandial sample.
In cats the measurement of fasting serum bile acids concentrations has a specificity approaching 100%.Bile acid concentration is also the most sensitive test for most feline hepatic diseases, although it only approaches 60% to 70%. The value of serum bile acids for detecting hepatic disease is also increased when combined with standard biochemical tests, and visa versa. As in dogs, the magnitude of elevation does not help in the differential diagnosis of hepatobiliary disease.
In detecting portosystemic shunts, serum bile acid concentrations have the best diagnostic accuracy compared with conventional biochemical tests and BSP excretion and sensitivity equal to the ammonia tolerance test. The accuracy is improved when postprandial bile acid concentrations are measured in conjunction with the preprandial sample.
In summary, serum bile acid concentrations are a sensitive and specific indicator of hepatobiliary function and hepatoportal circulation and are a clinically useful tool in the diagnosis of these disorders. Serum bile acid concentrations are especially valuable in anicteric hepatic disease. They are more conveniently measured than blood ammonia concentration because specimen handling is routine. They are more sensitive than BSP retention and do not require the injection of a foreign compound (which is becoming increasingly more difficult to obtain). In my laboratory, when postprandial concentrations exceed 30 to 40 μmol∕L in the dog and 20 to 30 μmol∕L in the cat, further diagnostic efforts, such as hepatic biopsy, are warranted.
Plasma Ammonia and the Ammonia Tolerance Test
Because ammonia is metabolized primarily in the liver, blood ammonia concentration represents a sensitive test of hepatic function. Ammonia is produced from bacterial action in the colon on substrates such as dietary proteins, sloughed intestinal epithelial cells, and urea, which freely diffuses into the colon from the plasma. Once absorbed into the portal circulation, ammonia is extracted by the liver and converted to urea through the urea cycle enzyme pathway. Normally this extraction process is very efficient, with only a small amount of ammonia escaping into the systemic circulation. The concentration of ammonia in the portal vein is approximately 350 μg∕dl in the dog (and approximately 700 μg∕dl in the cat), whereas the normal concentration in the systemic circulation is approximately 20 to 120 μg∕dl. When there is abnormal hepatocyte function or abnormal portal circulation (as would occur with portosystemic shunting), the liver cannot efficiently extract portal ammonia and systemic plasma levels increase.
Increasing the demand on the liver by increasing portal vein ammonia concentration can increase the sensitivity of plasma ammonia concentration in detecting abnormal hepatic function. This can be done by measuring ammonia concentration in the postprandial state or by administering an oral or rectal ammonia load. The latter provocative test is known as the oral ammonia tolerance test. The test is performed by taking a resting plasma ammonia sample, then administering oral ammonium chloride (NH4Cl) at a dosage of 45 mg/lb body weight, with a maximum dose of 3 g. Ammonium chloride is available from most chemical reagent suppliers or as the main ingredient of some urinary acidifiers. It is dissolved in 20 to 50 ml tap water and administered via orogastric tube, then flushed with 20 ml water. Alternatively, it can be administered in empty gelatin capsules. A plasma sample is then obtained 30 minutes later for ammonia measurement. A rectal ammonia tolerance test has been described. This is performed by administering 1 ml/lb body weight of a 5% solution of NH4Cl following cleansing enemas. A plasma sample is then obtained 20 to 40 minutes later. Theoretically, rectal administration has the advantage that vomiting of the orally administered solution is not a problem. However, in my experience, vomiting following oral NH4Cl administration is rarely a clinical problem, especially when the solution is diluted with water as described above, and does not invalidate the test if it occurs. Often the cause of vomiting is hyperammonemia, and therefore ammonia measurements are diagnostic of hepatic failure. In normal patients, there should be little or no increment in plasma ammonia concentration following administration of ammonium chloride (less than 32% increase).
Sample handling is critical for plasma ammonia determinations. It is important that the venipuncture be rapid and atraumatic. Prolonged stasis of blood can result in ammonia generation. When the sample is obtained, it must be placed in an ammonia-free heparinized tube and immediately placed in an ice bath, then centrifuged as soon as possible (within 30 minutes). Red blood cells elaborate ammonia (they contain two to three times as much ammonia as plasma), and, when the sample is not separated in a prompt manner, falsely elevated concentrations will result. Likewise, hemolysis will result in a falsely increased ammonia concentration. Ideally the sample should be assayed for ammonia as soon as possible (within 2 hours) to eliminate artifacts, because the ammonia concentration can increase or decrease with storage and thus yield unpredictable and unreliable results. Ammonia concentration may increase because of deamination of proteins such as glutamine, breakdown of adenyl pyrophosphate and/or adenylic acid, or hydrolysis of other ammonio- genic substances. Plasma ammonia may decrease during storage because of vaporous loss.
The main clinical usefulness of the ammonia tolerance test is in detecting patients with portosystemic shunts, in assessing hepatic function in anicteric hepatic disease (especially when hepatic enzyme activities may be normal), and in assessing the role of ammonia (and therefore hepatic function) in patients with encephalopathic signs. The test is as sensitive as measuring serum bile acid concentrations in assessing hepatic function and more sensitive than measuring BSP excretion. The ammonia tolerance test has been shown to be virtually 100% sensitive in detecting portosystemic shunts, whereas approximately 10% of dogs with congenital portosystemic shunts can have normal resting ammonia concentrations or normal BSP retention. Its main limitation is the need for meticulous sample handling and the need for the determination to be performed soon after obtaining the sample. In addition, it requires the administration of an exogenous compound (NH4Cl), which in rare instances can worsen encephalopathy and induce hepatic coma. If the latter complication is anticipated, a resting ammonia determination can be performed first, and the need and safety of NH4Cl administration can then be determined.
Serum Hepatic Enzyme Activities
The routine use of measuring serum hepatic enzyme activities as an indication of hepatic disease has been made possible by automated biochemistry profiles. It must be pointed out that enzyme activities do not reflect hepatic function. They reflect either the integrity of the hepatocyte membrane or the patency of the biliary system. Severe hepatic dysfunction can occur in the face of normal enzyme activities, whereas hepatic function may be near normal despite marked increases in serum enzyme activities. Therefore the limitations and usefulness of hepatic enzymes must be appreciated. Loss of intracellular enzymes (with the exception of certain proteases) does not lead to abnormal function or clinical signs but can be a useful laboratory test for diagnostic purposes. The enzymes that leak into plasma following increased hepatocellular membrane permeability include ALT,AST, SDH, LDH, and OCT. Enzyme activities that increase with biliary obstruction include ALP, GGT, and 5'-nucleotidase.
Serum Alanine Aminotransferase
Serum alanine aminotransferase (SALT; formerly serum glutamic-pyruvic transaminase [SGPT]) is the most liver-specific enzyme in the dog and the cat. It is used to detect hepatocyte membrane damage and necrosis. This enzyme is found only in the cytoplasm. Serum activity increases when there is increased permeability of the hepatocyte membrane, resulting in leakage from the hepatocyte. The extent to which enzyme leakage occurs depends on both the severity and number of cells damaged (i.e., how diffuse the lesion is) but does not indicate the reversibility of the injury or the functional status of the liver. The activity of SALT is most marked with chronic active hepatitis, primary hepatic neoplasia, and hepatic necrosis (see Table 9-1). There is often normal or only mildly increased SALT activity with portosystemic shunts, cirrhosis, and metastatic neoplasia. In rare cases, increased SALT activity can occur with severe muscle disease.
Although the activity of SALT usually parallels the degree of hepatocyte necrosis, there is often poor correlation with the serum enzyme activity and the degree of morphologic change on a light microscopic level, especially during the recovery phase. Likewise, there is often poor correlation between the serum activity of SALT and the degree of hepatocyte dysfunction and clinical signs. For example, there can be severe increases in SALT activity following automobile trauma or certain toxins, yet the patient often shows no signs of hepatic failure and other tests of hepatic function (such as serum bile acids or blood ammonia concentrations) remain normal. In these patients the magnitude of increase in SALT activity reflects the number of hepatocytes affected (i.e., the diffuseness of the lesion), although they maintain their ability to perform other intracellular functions. On the other hand, patients with portosystemic shunts, cirrhosis, or metastatic neoplasia often have normal SALT activity despite severe hepatic failure. In these patients the normal enzyme activity reflects either an intact hepatocyte membrane or, in the case of terminal cirrhosis, intracellular enzyme depletion.
There is often a mild to moderate increase in SALT activity with certain systemic diseases that result in hypoxia (such as right-sided heart failure with secondary ischemic injury to the hepatocyte, severe anemia, or severe pulmonary disease), endotoxemia, or sepsis. There is also a mild to moderate increase in SALT activity with biliary obstruction, probably as a result of the toxic effects of bile acids that diffuse back into the hepatic parenchyma. Pancreatitis and inflammatory intestinal diseases also may result in increased SALT activity. These cases are sometimes referred to as a “reactive hepatopathy.”
Serum Aspartate Aminotransferase
AST, like ALT, has high activity in the liver. However, there is also high AST activity in muscle and red blood cells, and serum aspartate aminotransferase (SAST; formerly serum glutamic oxaloacetic transaminase [SGOT]) activity is therefore less specific than SALT activity in detecting hepatocellular leakage. Increased activity of SAST occurs with both hepatocyte and muscle damage, as well as with hemolysis (in vitro or in vivo). AST is found both free in the cytoplasm and within mitochondria of the hepatocyte. With hepatic disease, SAST activity usually parallels that of SALT. Usually the magnitude of increase in SALT activity exceeds that of SAST activity. This may be due to the shorter half-life of SAST and because SAST is also found in the mitochondria of the hepatocyte. Therefore a more severe insult is required to cause mitochondrial damage and thus release of SAST from this site compared with damaging the hepatocellular membrane only. When the activity of SAST exceeds that of SALT, muscle or red blood cell, rather than the liver, should be considered as the source of the isoenzymes.
Serum Alkaline Phosphatase
The serum activity of ALP usually increases with biliary stasis, steroid hepatopathy, and bone lesions. ALP is found in many tissues, including the liver, bone, intestine, placenta, and kidney. However, in clinical situations only the isoenzymes found in the liver and in bone are important. This is because the serum half-lives of the other isoenzymes are only 3 to 6 minutes, whereas the halflife of the hepatic isoenzyme is 3 days in the dog. Serum activity of bone ALP increases with osteoblastic activity (and is therefore elevated in young, growing animals), bone tumors, osteomalacia, and hyperparathyroidism.
The serum activity of ALP increases with hepatic disease primarily when there is biliary obstruction (intrahepatic or extrahepatic). Unlike the transaminases (SALT and SAST), ALP is not a leakage enzyme associated with increased hepatocyte permeability. Rather, its production is induced by biliary obstruction, produced by cells lining the bile canaliculi. This increase in production is accompanied by inability to excrete the enzyme through the biliary system, thus resulting in increased serum activity. In addition to primary biliary obstruction, serum ALP activity is often elevated with primary hepatocellular disease of many causes due to swelling of hepatocytes (e.g., associated with inflammation, cloudy swelling, lipid accumulation, neoplastic infiltration) resulting in intrahepatic cholestasis (see Table 9-1). Diseases that are periportal in location tend to cause more marked increases in serum ALP activity than centrilobular disorders, because they tend to affect bile flow through canaliculi more.
In addition to the isoenzyme induced by biliary obstruction, there is also a steroid-induced isoenzyme of ALP. Although this isoenzyme is also produced in the liver, it is a separate entity from that induced by biliary obstruction. The dog is very sensitive to the effects of glucocorticoids in this regard as opposed to the cat. A single injection of a glucocorticoid can increase the serum activity of the steroid-induced isoenzyme of ALP. This increase in activity can last for several weeks with short-acting preparations and for several months with long-acting preparations. The magnitude of increase depends on the dose administered, duration, route, and individual sensitivity. In addition, dogs with spontaneous hyperadrenocorticism (Cushing's syndrome) usually have marked increases in serum ALP activity. Assays are now available to readily distinguish the isoenzyme induced by biliary obstruction from the steroid- induced isoenzyme. These assays generally report the percentage of total ALP activity that is accounted for by the steroid-induced isoenzyme. However, this is not a reliable test to distinguish patients with steroid hepatopathy from those with other hepatopathies because the serum activity of the steroid-induced isoenzyme of ALP is variably increased with many types of hepatic diseases and nonhepatic illness. Alternatively, hepatic biopsy specimen analysis in dogs readily distinguishes steroid-induced hepatopathy from primary hepatobiliary disease of other causes.
Certain drugs will also induce increases in serum ALP activity. The most common drugs to have this effect are glucocorticoids, barbiturates, and anticonvulsant drugs, including phenobarbital, primidone, and phenytoin. These drugs will result in increased serum ALP activity, with or without morphologic changes in the liver or alterations in hepatic function (as documented with hepatic function tests).
Unlike the dog, the activity of ALP is much lower in feline serum. This is because the half-life is much shorter in the cat (6 hours versus 3 days) and less feline ALP is produced secondary to biliary obstruction than in the dog because the feline liver contains only one third the concentration of ALP per gram of liver that the canine liver contains. Therefore even mild elevations of serum ALP activity in the cat are indicative of marked hepatobiliary disease. The magnitude of increase in serum ALP activity is most marked with feline hepatic lipidosis, almost always exceeding the magnitude of increase in serum GGT activity in this syndrome. Other diseases in the cat that result in increased serum ALP activity include hepatic malignant lymphoma, feline cholangiohepatitis complex, bile duct obstruction, and hyperthyroidism.
Gamma Glutamyltranspeptidase
GGT measurement is now available on chemistry profiles from many commercial laboratories. Its serum activity increases with biliary stasis and steroid hepatopathy. In most cases the activity of serum GGT parallels that of serum ALP and its measurement is of only occasional value in the dog and cat. There is GGT activity in liver, kidney, pancreas, and intestine; however, the half-life of the hepatic isoenzyme is the only one long enough to account for significant serum activity. Therefore elevated serum GGT activity is specific for hepatobiliary disease or hepatic induction from drugs. As with serum ALP, elevations are most marked with biliary obstruction, but activity can also increase with primary hepatocellular disease if it results in intrahepatic cholestasis. The serum activity of GGT may increase earlier in biliary disease than ALP activity. In addition, there is also marked elevation in serum GGT activity with glucocorticoid administration or spontaneous hyperadreno- corticism. Other drugs (such as anticonvulsants) will also increase serum GGT activity.
In the cat, serum GGT activity has a higher sensitivity but lower specificity than serum ALP activity for detection of hepatobiliary disease. Only in feline hepatic lipidosis does the magnitude of increase in serum ALP activity generally exceed that of serum GGT activity. In the dog, serum GGT activity is generally more specific but less sensitive than serum ALP activity for the detection of hepatobiliary disease. Thus serum GGT activity has a higher positive predictive value, whereas ALP activity has a higher negative predictive value for evaluating hepatobiliary disease. The diagnostic performance is best when both enzyme activities are evaluated together. In general, serum GGT activity is less influenced by nonhepatic diseases or enzyme-inducing drugs.
Other Biochemical Tests
Many of the tests routinely obtained on automated serum biochemistry profiles give information regarding hepatic function, including determinations of bilirubin, albumin, BUN, and glucose (see Table 9-1).
Serum and Urine Bilirubin
Hepatobiliary excretion of bilirubin requires adequate uptake, conjugation, and secretion by the hepatocyte, as well as a patent biliary system. There must be considerable hepatocellular disease or increase in the bilirubin load (hemolysis) to result in hyperbilirubinemia, because the liver's reserve capacity for bilirubin processing is up to 30 times the normal bilirubin load. Conjugated bilirubin is water soluble and readily excreted by the kidneys. The dog has a very low renal threshold for bilirubin excretion; thus the finding of +1 to +3 bilirubinuria in a concentrated sample is normal. Therefore the concentration of bilirubin in the urine increases before that of the serum. Thus the serum bilirubin concentration is an insensitive indicator of hepatocellular disease, and serum concentrations are not increased until there is marked decrease in hepatic function. Therefore slight elevations in serum bilirubin concentration are significant, suggesting hepatobiliary disease. The exception to this is with artifactual increases in serum bilirubin concentration, as would occur with lipemia or hemolysis. If there is not significant bilirubinuria associated with a serum bilirubin concentration greater than normal, artifact should be considered. The cat has a high renal threshold for bilirubin excretion, and any bilirubin in the urine is abnormal. When serum bilirubin is in the normal range (anicteric hepatic disease), other tests of hepatic function discussed earlier are needed for detection, such as serum bile acid or blood ammonia measurements. However, when serum bilirubin concentration is elevated, there is no need to run additional function tests if hemolysis can be excluded. In this setting, bilirubin represents an accurate and specific indicator of hepatic function.
Increased serum total bilirubin concentration can result from prehepatic (hemolysis), intrahe- patic (primary hepatocellular disease), or posthe- patic (biliary obstruction) causes. The relative amounts of conjugated or unconjugated bilirubin are variable with all three general categories of hyperbilirubinemia because secondary events can change the relative concentrations of the two forms. Therefore their measurement does not aid the clinician in localizing the nature of the lesion. The magnitude of increase in serum bilirubin concentration also is not helpful in localizing the nature of the lesion. Other methods of localizing the cause of hyperbilirubinemia include measuring the hematocrit (to rule out hemolysis) and ultrasonography, laparoscopy, cholecystography, and laparotomy (to distinguish intrahepatic from posthepatic causes).
In general, serum bilirubin concentration increases most markedly with extrahepatic biliary obstruction. Hepatocellular diseases that may result in cholestasis and therefore hyperbilirubinemia include chronic active hepatitis, certain cases of primary neoplasia, feline cholangiohepatitis, feline hepatic lipidosis, and cirrhosis (see Table 9-1). Other hepatic disorders that generally have normal serum bilirubin concentration include portosystemic shunts, hepatic necrosis, steroid hepatopathy, and metastatic neoplasia (see Table 9-1). In general, disorders involving the periportal areas are most likely to result in increased bilirubin concentration.
Serum Albumin
Albumin represents approximately 25% of the proteins synthesized by the liver. Because albumin has a relatively high priority for synthesis, severe hepatocellular disease must exist before serum albumin concentration falls. Hypoalbuminemia resulting from hepatic disease suggests chronic dysfunction. Because the serum half-life of albumin is 7 to 21 days (depending on the disease state and the serum concentration), there must be prolonged hepatic disease before serum concentration decreases. In addition to lack of production occurring with hepatic disease, albumin concentration can drop from protein-calorie malnutrition (sometimes associated with an extremely low protein diet, often used in the therapeutic management of hepatic disease) and from an increased volume of distribution due to ascites, resulting in a dilutional effect on serum albumin concentration. Although serum albumin concentration is an insensitive and nonspecific test of hepatic function, hypoalbuminemia may be the only change on a serum biochemistry profile in certain cases of hepatic failure (such as cirrhosis and portosystemic shunts), and its presence may justify specific hepatic function tests (e.g., serum bile acid assay), which may subsequently identify hepatic failure. In one study the presence of hypoal- buminemia in dogs with chronic hepatitis was a predictor of shorter survival time.
Blood Urea Nitrogen
A low BUN concentration may indicate chronic hepatic disease. The liver manufactures urea by extracting portal vein ammonia and converting it to urea through the urea cycle enzyme pathway. With hepatic failure this process fails, and BUN concentration falls. However, because there are many other factors that influence urea metabolism (including renal function, dietary protein concentration, catabolic states, systemic perfusion and hydration status, and GI function), BUN concentration is an insensitive and nonspecific test of hepatic function. However, like serum albumin concentration, a low BUN concentration may be the only abnormality on a serum biochemistry profile and may be an important clue as to the presence of hepatic disease. Subsequent specific hepatic function tests would then be used to document hepatic failure.
Serum Glucose
The liver plays an important role in glucose metabolism. Hepatic failure can result in either preprandial hypoglycemia or postprandial hyperglycemia. In dogs with chronic hepatitis the presence of hypoglycemia is an accurate predictor of early death. When there is abnormal glucose concentration, causes in addition to hepatic disease must be explored. In patients with hypoglycemia associated with hepatic disease, it is usually easy to get the blood glucose concentration into the normal range with intravenous glucose supplementation, as opposed to patients with insulin-producing tumors, in which it can be very difficult despite aggressive intravenous glucose administration.
Radiographic Evaluation of the Liver
Survey Radiographs
Survey radiographs are often informative when evaluating the liver. They give information about the size, shape, position, and radiodensity of the liver. Survey radiographs are also useful to screen for other abnormalities, including ascites, renal calculi (present in some cases of portosystemic shunts), thoracic metastasis, and abdominal lymphadenopathy. Radiographic signs of abnormal hepatic size are listed in Boxes 9-4 and 9-5. Causes of abnormal hepatic size are listed in Boxes 9-6 and 9-7. In addition to hepatic size, abnormalities in hepatic radiodensity can also be determined from survey radiographs. These abnormalities include (1) calcification (cholelithiasis, parasitic cysts, neoplasia, or granulomas), (2) gas accumulation (cholecystitis, gas in the portal veins, hepatic abscess, or necrotic tumors), and (3) inability to visualize hepatic borders (ascites or emaciation). Radiography is reviewed in detail in Chapter 2.
BOX 9-4
Radiographic Signs of Decreased Hepatic Size
Decreased distance between the diaphragm and stomach
Displacement of the stomach cranially or upright angulation of the stomach axis in the lateral view Displacement of the stomach to the right in the dorsoventral view
Cranial displacement of the cranial duodenal flexure, right kidney, and transverse colon
Liver and stomach entirely within the chest cavity
BOX 9-5
Radiographic Signs of Increased Hepatic Size
Extension of the liver margin caudal to the costal arch
Rounding of the caudal margins on the lateral view Displacement of the stomach caudally and dorsally on the lateral view
Displacement of the stomach caudally and to the left on the ventrodorsal view
Caudal displacement of the cranial duodenal flexure, right kidney, and transverse colon
BOX 9-6
Causes of Radiographic
Signs of Decreased
Hepatic Size
Cirrhosis
Portosystemic shunt
Acute and subacute necrosis
Hernias (diaphragmatic and peritoneal-pericardial)
Deep-chested breeds (normal)
Evaluation of Hepatic Blood Flow
Along with nuclear scintigraphy and laparotomy, contrast radiography is a reliable method to determine whether there is a portosystemic shunt present. There are several techniques to evaluate hepatic blood flow, including intraoperative mesenteric portography, percutaneous splenoportography, and cranial mesenteric arterial portography.
Intraoperative Mesenteric Portography
The indications to perform intraoperative mesenteric portography are to confirm the existence, number, and location of portosystemic shunts. In
BOX 9-7
Causes of Radiographic Signs of Increased Hepatic Size
Neoplasia (primary or metastatic)
Congestion (right-sided heart failure)
Fatty infiltration
DiffUse inflammation
Hyperadrenocorticism
Storage diseases
Abscess
Hepatic or biliary cyst
Liver lobe torsion
Puppies and kittens (normal)
Deep inspiration (normal) addition, the residual portovenous flow into the liver can be assessed for prognostic importance. If a portosystemic shunt is identified, surgical correction may be performed during the same anesthetic procedure.
Technique
Intraoperative mesenteric portography is a technique that can readily be performed in general practice, because no special equipment is needed. A mesenteric or jejunal vein is catheterized at laparotomy. A vessel that can eventually be sacrificed is selected, and as large a catheter as possible is used. Once the catheter is secured, an intravenous extension set is attached and the abdomen temporarily closed (with the extension set exiting through the abdominal wall). A total of 0.25 to 0.5 ml/lb body weight of an iodinated radiographic contrast media is injected as rapidly as possible through the extension set. A radiograph is obtained just at the end of the injection. Unless a portable radiographic unit is available, it is usually easiest to perform the laparotomy on the x-ray table. With portosystemic shunting, contrast media passes directly into the systemic venous circulation and bypasses the liver. If the caudal extent of the shunt is cranial to T13, it is probably an intrahe- patic shunt; if it is caudal to T13, it is probably an extrahepatic shunt.
Percutaneous Splenoportography
The indications for percutaneous splenoportography are similar to those described for intraoperative mesenteric portography. Splenoportography often yields a lesser quality study but has the advantage of not requiring a laparotomy. This is especially important in a hypoalbuminemic patient that is at risk for wound dehiscence.
Technique
General anesthesia or heavy sedation is required for splenoportography. The spleen is localized by transabdominal palpation, or ultrasound or laparoscopy can be used to aid in needle placement. Approximately 0.25 to 0.5 ml/lb body weight of an iodinated radiographic contrast media is injected directly into the splenic pulp at the rate of 1 to 2 ml/sec. Radiographs are taken immediately and approximately 10 seconds after the end of the injection.
Cranial Mesenteric Arterial Portography Cranial mesenteric arterial portography is an excellent method of evaluating the entire portal system and evaluating hepatic blood flow. The technique is less invasive than operative mesenteric portography; however, it requires fluoroscopy, serial films, and special injection equipment.
Ultrasonographic Evaluation of the Liver
Ultrasonography is now widely used to evaluate the liver because it is ideally suited for soft tissue imaging. It gives specific information regarding structural abnormalities in the liver and can readily distinguish fluid-filled structures from solid soft tissue structures, including visualization of the gallbladder, hepatic vessels, and adjacent parenchyma. Hepatic ultrasonography is discussed in Chapter 2. Also see the References for additional information regarding basic principles of ultrasound and the ultrasonographic appearance of the liver.
The main reasons I use ultrasonography to evaluate hepatic disease are to distinguish focal from diffuse disease (and thus help determine an appropriate biopsy method) and to distinguish intrahepatic causes of cholestasis from extrahepatic causes of cholestasis (the former being a potentially medically treatable problem, the latter a surgically treatable problem). Additional indications for an ultrasound evaluation of the liver include any abnormality in hepatic function, size, or radiodensity. Diffuse changes in hepatic echogenicity (compared with falciform fat, the renal cortex, and spleen) may suggest certain hepatic diseases. Diffuse hyperechogenicity is seen with fatty change, steroid hepatopathy, fibrosis, and cirrhosis. Hypoechogenicity is seen with passive congestion, lymphoma, and suppurative hepatitis. Ultrasonography can also be a useful method to obtain a biopsy specimen of the liver, because it can be used to guide a biopsy needle into an appropriate portion of the liver. Normal structures and abnormalities detectable by ultrasonography are listed in Boxes 9-8 and 9-9.
Nuclear Scintigraphy to Evaluate the Liver
Nuclear scintigraphy is primarily used to evaluate hepatic blood flow and aids in the detection of portosystemic shunts. Scintigraphy may in some cases localize the shunt and distinguish intrahep- atic from extrahepatic shunts. It also represents a noninvasive method of proving the existence of a shunt. It may be followed by more invasive studies, such as mesenteric portography or surgery. Nuclear scintigraphy equipment is primarily available at referral centers.
Technique
Technetium-99m pertechnetate is an inexpensive, available radioisotope that is absorbed across the colonic mucosa. When administered in high concentration into the colon, dynamic imaging during the first 1 to 2 minutes can provide a nuclear angiogram of the portal system. These images in normal dogs result in sequential visualization of the portal vein, liver, and several seconds later the heart and lungs. In patients with portosystemic shunts, heart and lung activity occur before liver activity.
The procedure is well tolerated and does not require sedation. In many cases the study allows distinction between intrahepatic shunts, single extrahepatic shunts, and multiple extrahepatic shunts. Although the study does not give the anatomic detail of radiographic contrast studies, the information is usually specific enough to determine whether the patient is a good operative
BOX 9-8
Normal Structures
Detectable by Hepatic
Ultrasonography
Diaphragm
Hepatic parenchyma
Gallbladder
Hepatic and portal veins Intrahepatic bile ducts (variable) Cystic duct (variable) Common bile duct (variable)
BOX 9-9
Abnormalities Detectable by Hepatic Ultrasonography
Ascites
Hepatic enlargement
Hepatic fibrosis
Neoplasia (focal or metastatic)
Distended gallbladder and biliary tree
Portal or hepatic venous distension
Hepatic cysts
Hepatic abscess
Calcification
Portosystemic shunts
Lipidosis/vacuolar hepatopathy
Nodular regeneration candidate. In addition, the radioisotope enters the portal system more caudal to the liver than in angiographic studies, so distal or caudal shunts are not missed. The study can also be performed on cats but may require a higher imaging frequency.
A similar procedure has also been described in dogs using transcolonic 123I-iodoamphetamine (IMP). This is a radiolabeled amine that binds to liver and lungs following absorption from the colon. Imaging within 10 minutes of administration and counting activity in liver and lung allows a direct calculation of portal blood flow that is bypassing the liver. This method is also noninva- sive and accurate. However, disadvantages compared with transcolonic administration of 99mTc pertechnetate are the high expense and relatively long half-life of the radioisotope 123I.
An alternative technique involves analysis of an intravenous injection of radiocolloid. Radiocolloids are removed from the circulation by the RES of the body. It has been shown that the uptake of radiocolloid by the liver is a reflection of hepatic blood flow rather than phagocytic properties of Kupffer's cells. Thus radiocolloid scintigraphy is a sensitive technique to screen for portosystemic shunts. The procedure is safe, does not require sedation, and is relatively rapid. Radiocolloid scintigraphy is performed by injecting 3 to 5 mCi 99mTc sulfur colloid intravenously and subsequently scanning the organs of the body with a gamma camera. A computer is used to plot activity in the lungs and liver against time.
In normal dogs there is initial activity in the lungs, which rapidly decreases during the initial passage of the bolus (60 seconds) as the radiocolloid is cleared from the circulation by the spleen and liver. There is subsequent gradual increase in activity in the liver, reflecting uptake of the radiocolloid. In dogs with portosystemic shunts, there is increasing activity in the lungs after the initial passage of the bolus, indicating pulmonary uptake. The rate of hepatic uptake is considerably less than that seen in normal dogs. Unfortunately, there are many indeterminate and false-positive results with this method compared with transcolonic administration of the radioisotope. In normal cats, extrahepatic uptake in the lungs occurs, preventing adequate images of the liver.
Hepatic Biopsy
Hepatic biopsy specimen analysis is the only way to accurately diagnose and classify hepatic disease. Biochemical tests, radiographs, and ultrasonography determine that hepatic disease exists. None of these tests accurately determines the cause or appropriate treatment or predicts prognosis (with the exception of angiography or scintigraphy for detecting portosystemic shunts). Recent advances in biopsy methods and in noninvasive imaging of the liver have made hepatic biopsy a routine and essential tool in the diagnosis and management of patients with hepatic disease. Many types of hepatic diseases are treatable, and a definitive diagnosis allows the clinician to make appropriate clinical decisions with regard to specific treatment, rather than just supportive care. Hepatic biopsy specimen analysis helps determine whether the abnormality is (1) reversible or irreversible, (2) progressive or static, (3) primary hepatic or secondary, (4) treated with specific therapy or only with supportive therapy and whether there is a need for follow-up biopsy posttreatment.
Indications
The most common indication for performing hepatic biopsy is abnormal hepatic function and/or increased serum hepatic enzyme activities of unknown origin. This is usually identified by hepatic function tests (such as serum bile acids or blood ammonia measurements) and serum biochemical profile findings obtained in patients showing signs compatible with hepatic disease or in routine preanesthetic blood work. If clinical illness is attributed to hepatic disease, a biopsy is warranted.
In patients with persistently abnormal serum hepatic enzyme activities, efforts to rule out nonhepatic causes of enzyme elevations should be made first, such as hyperadrenocorticism, diabetes mellitus, congestive heart failure, and feline hyperthyroidism. In an asymptomatic patient, when increased hepatic enzyme activities are detected on routine biochemical profiles, I generally assess hepatic function with serum bile acid measurements. If these are not grossly elevated, the biochemistry profile is repeated in 4 to 6 weeks. If there is a persistent increase in hepatic enzyme activity at this time, hepatic biopsy is justified.
Abnormal hepatic size of unknown cause (either microhepatica or hepatomegaly) is another indication for hepatic biopsy. If hepatomegaly is present, efforts must be made to rule out nonhe- patic causes, such as hyperadrenocorticism, diabetes mellitus, and congestive heart failure. Even in the presence of these disorders, it might be clinically indicated to assess hepatic involvement in these multisystem diseases with hepatic biopsy specimen analysis. In many cases of hepatomegaly (with either diffuse or focal enlargement), the purpose of the biopsy is to confirm suspected neoplasia. Recent advances in chemotherapy have made this an important step in proper management.
Finally, hepatic biopsy specimen analysis is important to document the progression of disease. Often multiple or serial biopsies are necessary to document remission (as in certain cases of chronic active hepatitis [CAH] or hepatic malignant lymphoma) and therefore determine appropriate treatment.
Precautions
Most contraindications to hepatic biopsy are relative contraindications and depend on the biopsy method. When these factors are present, the clinician must weigh the potential benefits of obtaining the biopsy (i.e., a definitive diagnosis and the opportunity to begin rational specific therapy) with the risks of the complications that could potentially occur. However, with experience and knowledge of various methods of hepatic biopsy, these risks can be minimized.
The most common contraindication to hepatic biopsy is a coagulopathy. Determining the nature of the coagulopathy is important in minimizing its influence. The most common coagulopathy associated with hepatic disease is DIC. When DIC is present, knowledge of the underlying disease is essential in long-term management, and thus obtaining the biopsy is essential. In this setting I recommend high volumes of intravenous fluids to maintain tissue perfusion in the face of microthrombi, platelet function inhibition with aspirin to minimize the hypercoagulable state, and a transfusion with fresh crossmatched whole blood collected in a plastic collection bag (glass activates factor XII) with 125 units of heparin added per 500 ml of blood to activate antithrombin III (to minimize the hyper- coagulable state). Methods of obtaining the biopsy that require a minimal incision yet allow control of bleeding, such as laparoscopy-guided or the keyhole method, are preferred.
When there are prolonged clotting times unaccompanied by DIC, there may be decreased clotting factor synthesis or vitamin K deficiency. Vitamin K administration may be helpful in certain situations. In one report vitamin K administration improved PIVKA times in 10 of 23 dogs with hepatic disease and normalized PIVKA times in 12 of 48 cats. It has been my experience that bleeding following hepatic biopsy does not correlate with coagulation tests, including the PIVKA test. Patients with coagulopathies are no more likely to bleed than patients without coagulopathies. In most cases of significant bleeding following hepatic biopsy, there are technical problems. In my experience the rapidity of bleeding and/or necropsy examination suggest that a large vessel has been damaged rather than hemorrhage being due to persistent oozing from needle biopsy sites. The exception to this is that patients with DIC often have significant hemorrhage regardless of technique. Controlled studies in veterinary patients will be necessary to make final conclusions regarding postbiopsy hemorrhage in the patient with a coagulopathy.
An unstable patient that cannot be safely anesthetized is another relative contraindication for performing a liver biopsy. In these patients blind percutaneous or ultrasound-guided biopsy methods may be considered because these can often be done with minimal or no sedation.
Complete biliary obstruction with dilation of intrahepatic bile ducts is a contraindication described in humans because of the potential for bile peritonitis. Theoretically this occurs because there is increased intraductal pressure, and therefore inadvertent duct rupture following biopsy results in bile leaking into the abdominal cavity. In my experience, however, this complication has not been recognized in cases when percutaneous biopsy was performed in animals with biliary obstruction.
Finally, hepatic abscess, cyst, or vascular tumors are contraindications to percutaneous biopsy methods. Unfortunately, it is usually not known that these are present until it is too late, unless an imaging modality such as ultrasonography or laparoscopy is available.
Prebiopsy Considerations
Appropriate biochemical and hepatic function tests must be performed to assess the need for the biopsy and identify concurrent disease. Once the need for hepatic biopsy is determined, several considerations must be made. History, physical examination, laboratory, and ancillary findings determine the overall health status of the patient. This is important in deciding an appropriate anesthetic regime. Certain biopsy methods require minimal to no sedation (blind percutaneous or ultrasound- guided), some require short general anesthetics (keyhole or laparoscopy-guided), whereas others require a long general anesthetic (laparotomy). In addition, patients with extremely low serum albumin concentration are at greater risk for wound dehiscence and therefore biopsy is more appropriately performed with percutaneous methods.
Abdominal radiographs are helpful to assess hepatic size. This information is useful to narrow the list of differential diagnoses and also to help plan the biopsy approach. For example, with microhep- atica the transthoracic percutaneous approach may be preferred over the transabdominal percutaneous approach and laparoscopy-guided biopsy may be preferred over ultrasound-guided biopsy. The reverse is true with hepatomegaly. Thoracic radiographs are helpful to rule out metastatic neoplasia.
Coagulation profiles should be performed before hepatic biopsy because of the multitude of abnormalities possible with hepatic disease. These were discussed in detail in the section on pathophysiologic derangements occurring with hepatic disease. Ideally PIVKA time, prothrombin time, partial thromboplastin time, platelet count, and fibrin degradation product determinations should be made before hepatic biopsy. If there are significant cost and time concerns, a less acceptable alternative is the measurement of activated clotting time and toenail bleeding time. The former test assesses the intrinsic and common clotting pathways but is only abnormal when clotting factor activity drops below 10% of normal (whereas partial thromboplastin time is abnormal when clotting factor activity drops below 30% of normal). The management of coagulopathies when obtaining hepatic biopsy was discussed in the section on precautions for hepatic biopsy.
Because chemical restraint is sometimes necessary to insure a safe procedure, the patient should be clipped before sedation. For general anesthesia I prefer isoflurane or sevoflurane induction by face mask or induction chamber. If an injectable anesthetic is desired, I prefer the combination of ketamine and diazepam. Although oxymorphone provides adequate restraint and can be reversed if necessary, excessive panting often occurs, which interferes with the biopsy procedure and therefore is not recommended.
Biopsy Methods
The five basic methods of obtaining a hepatic biopsy are blind percutaneous, keyhole technique, ultrasound-guided, laparoscopy-guided, and laparotomy biopsy. Each method has certain advantages and disadvantages. Knowledge of these, as well as practice and expertise in each respective method, allow the clinician to select the most appropriate and safest method to obtain hepatic tissue.
Blind Percutaneous Biopsy
The advantages of blind percutaneous biopsy are that it is very rapid, requires minimal sedation, and is low cost. Disadvantages of this method are that there is the potential for inadvertent trauma to other organs, focal lesions may be missed, and detection of bleeding may be delayed.
Equipment
Various biopsy needles can be used for percutaneous biopsy. In general, newer automated needles are preferred. These are spring-loaded needles that are similar in style to manual Tru-Cut (Baxter) or ABC (Monoject) needles. Automated needles can be completely automatic or semiautomatic. Automated cutting needles include the Monopty (Bard), ASAP (Microvasive), and Biopty (Bard) needles. Completely automatic needles thrust the inner obturator (containing the biopsy tray or specimen notch) followed by the outer cutting sheath into the organ in a fraction of a second. These needles can easily be operated with one hand. Because the action is so quick, there is minimal displacement of the organ, a shorter intra- parenchymal phase, and much more reliable yield of tissue. This allows the biopsy of the organ to be performed with minimal manual mobilization, allows a smaller diameter needle to be used, and allows a lighter degree of sedation.
Semiautomated cutting needles include the Vet-Core needle (Cook). Semiautomatic needles require manual thrusting of the internal obturator (containing the biopsy tray or specimen notch) into the organ, followed by an automatic thrusting of the outer cutting sheath by the spring-loaded mechanism. These needles have some of the advantages of the completely automatic needles and have the additional advantages of having more control over final needle position and being lighter with a smaller handle. These characteristics also make these needles well suited to computed tomography (CT) guidance because the handle can be let free by the operator for intraprocedural scanning without the weight of the handle causing the needle to move. In addition, the tip of the needle can be precisely localized before the outer cutting sheath is “fired.” The older manual cutting needles (Tru-Cut or ABC needles) offer no advantages over these newer needles.
Aspiration needles are generally used to obtain smaller samples that would be suitable for cytologic preparations (rather than histopathologic preparations), or for Menghini and Westcott needles, used to obtain small samples for histopathologic examination (see below). These needles are also well suited to obtain samples of fluid, such as intraparenchymal cysts and gallbladder puncture. Usually these are smaller-gauge needles (20 to 22 gauge) and therefore tend to be less traumatic. Aspiration needles employ suction to obtain fluid or cut the core of tissue. The Menghini needle is especially suited for transthoracic hepatic biopsy but can be used for transabdominal techniques as well. The tip of the needle is slightly oblique and convex and cuts a core of tissue when suction is applied as the needle is rapidly thrust into the liver and immediately withdrawn. The intrahepatic phase should last just a fraction of a second. A sliding screw acts as a depth gauge and prevents the needle from entering too deeply into the parenchyma. For the Westcott needle, suction is used to draw tissue into a specimen notch at the distal end. Gentle back-and-forth movement allows a core of tissue to be cut.
Transthoracic Technique
Because of the short intrahepatic phase, the transthoracic technique is especially suitable for patients in which sedation is too risky or undesirable and in patients with microhepatica, in which the transabdominal technique may be difficult. The patient is given corn oil orally (1 ml/lb body weight) to cause the gallbladder to contract and thus minimize the risk of inadvertent puncture. A Menghini needle is used to obtain the biopsy specimen. The patient is placed in left lateral recumbency, and the right hemithorax clipped and surgically prepared. A local anesthetic is injected subcutaneously at the needle puncture site: just dorsal to the costochondral junction of the fifth through seventh intercostal space (depending on the size of the patient and distance to the diaphragm). Using a No. 11 blade, a skin incision is made to prevent dulling of the biopsy needle.With the stylet of the Menghini needle in place, the needle is “popped” into the pleural space and then directed caudally and parallel to the rib cage until it contacts the diaphragm (respiratory movements will be felt). Care is taken to avoid lacerating the intercostal vessels that lie along the caudal aspect of each rib. Upon making contact with the diaphragm, the needle depth gauge is slid to within approximately 1.5 cm of the skin so that the depth of penetration into the liver is limited to this distance. The stylet is then removed and quickly replaced with a 12-ml syringe filled with 5 to 6 ml of sterile saline. Negative pressure corresponding to approximately 3 ml of fluid volume is produced by drawing on the plunger. At the peak of expiration, the needle is rapidly thrust into the liver (with the distance limited by the depth gauge) and immediately withdrawn from the patient in one swift motion, maintaining negative pressure throughout. This entire step (i.e., the intrahepatic phase) should last only a split second. The core of hepatic tissue should rest within the fluid in the syringe or in the needle. The plunger is removed and the contents poured into culture broth, onto a slide for impression cytologyic study, and/or into a jar containing 10% formalin. The patient is then immediately turned onto its right side for approximately 5 minutes to allow the weight of the liver to control hemorrhage.
Possible complications with this technique include gallbladder puncture (and possible bile peritonitis and pleuritis), pneumothorax, and excessive bleeding. In patients with firm fibrotic livers, this technique may not yield a suitable sample. In this situation a cutting type of needle used with a transabdominal approach may be successful.
Transabdominal Technique (Blind)
The transabdominal technique is especially useful when the size of the liver is normal or large. It has a longer intrahepatic phase than the transthoracic technique if a cutting type of needle is used, and therefore a higher degree of sedation may be necessary in an uncooperative patient. The patient is given corn oil orally (2 ml/kg body weight) to cause the gallbladder to contract and thus reduce the risk of inadvertent puncture. I prefer to use automated cutting type of needles such as the Monopty or ASAP needles. The patient is placed in right dorsal oblique recumbency at a 45-degree angle. In this position the stomach falls down toward the right side. A large area around the xiphoid cartilage is clipped and surgically prepared. A local anesthetic is injected subcutaneously at the needle entry site: just caudal and to the left of the xiphoid cartilage, in the middle of the “V” formed by the xiphoid cartilage and the rib cage. If the needle enters too far cranially, it may inadvertently enter the thoracic cavity. If there is hepatomegaly, the entry site is moved cau- dally as appropriate for the hepatic size. The skin is incised with a No. 11 blade to prevent dulling of the biopsy needle. The biopsy needle is inserted and advanced just through the body wall and aimed in a craniolateral direction towards the left shoulder. The needle should be advanced during inspiration. The liver should be very close to the body wall, and the needle need not be advanced very far. Penetration of the liver is often not felt. The most common error using this technique is inserting the needle too far and going completely through the liver. Once the liver is entered the biopsy needle is operated to cut the sample. This is done during peak inspiration. The needle is removed after each attempt. The core of hepatic tissue should be resting within the specimen notch of the needle. If the initial attempt fails to obtain hepatic tissue, the needle is redirected based on perceived location of the liver, body conformation (i.e., deep chested), and direction of previous attempts. Tissue is carefully removed with a 25-gauge needle and placed into culture broth, onto a slide for impression cytologic study, and/or into 10% formalin. The patient is immediately placed in sternal recumbency to allow the weight of the liver to control hemorrhage.
Possible complications of this technique include puncture of the stomach, gallbladder rupture (and possible bile peritonitis), puncture of the diaphragm and lung (and possible pneumothorax), and excessive bleeding.
Keyhole Technique
The keyhole technique offers the advantages of providing more guidance of the needle than blind percutaneous biopsy, being relatively rapid, and being low cost. Disadvantages of this method include the requirement for more sedation compared with blind percutaneous biopsy, the possibility of causing inadvertent trauma to other organs, the possibility that focal lesions may be missed, and the possibility that detection of bleeding may be delayed. This technique is especially suitable for individuals who lack the experience to perform a blind percutaneous biopsy.
The keyhole technique and equipment are similar to that described for the blind transabdominal percutaneous biopsy. Under a general anesthetic a small incision into the abdominal cavity is made just caudal to the site of needle introduction. A gloved finger is inserted into the abdomen to palpate the liver and stabilize it for biopsy. The needle is inserted through the same incision or through a separate incision just cranial to the first incision. The finger then guides the needle into the liver, and the biopsy specimen is cut. I prefer an automated cutting needle for this technique because it can be operated with one hand, whereas the Tru-Cut needle would require an assistant to operate the needle. Complications are similar to those described for blind percutaneous biopsy.
Ultrasound-Guided Biopsy
Ultrasound-guided biopsy offers the advantage of providing more guidance to the needle than is possible with blind percutaneous biopsy, is relatively rapid, and requires minimal sedation. Because intraparenchymal lesions can be visualized, biopsy of them can be selectively performed. In addition, other intrahepatic structures such as the gallbladder and portal vessels can be avoided. Disadvantages of ultrasound-guided biopsy include the requirement for expensive equipment and that detection of bleeding may be delayed. As with other biopsy methods, success is operatordependant. Ultrasound-guided biopsy is easier when the liver is normal or large in size. When there is microhepatica, overlying gas in the stomach often makes visualization of the liver difficult. In this setting, laparoscopy would offer a more appropriate image-guided biopsy method.
Technique
Most dogs require minimal sedation for ultrasound-guided biopsy. I use a low dose of ketamine for cats (10 to 20 mg intravenously) or isoflurane or sevoflurane administered by face mask. A careful ultrasound examination is performed before biopsy. This allows planning of the procedure based on the type of echo pattern, size of the lesion, proximity to other organs, proximity to blood vessels, determination of cystic or solid tissue, and determination of the needle path. For focal liver biopsy the location of the lesion will determine the position of the scan head and needle path. For diffuse lesions the transducer is usually placed just caudal and to the left of the xiphoid and aimed at the left medial or lateral lobes. In patients with extremely small livers, it may be difficult to adequately visualize the needle without stomach gas interfering. In this case placing the patient in a 45-degree right ventral oblique position often helps reduce interference from the stomach. Otherwise the patient is usually placed in dorsal recumbency for most procedures. A rubber trough or V tray assists in positioning. In addition, if the patient is under gas general anesthesia, an assistant compresses the rebreathing bag to hold the patient in deep inspiration. This moves the diaphragm and liver caudally to improve visualization. If a lesion cannot be seen due to overlying gas or bone, changing patient or transducer position usually allows adequate visualization.
The area to be scanned, including the needle entry site, is surgically prepared. The ultrasound transducer is covered with sterile plastic wrap (or a sterile glove) after a small amount of coupling gel is placed on the transducer surface. A biopsy guide may be used if desired, allowing accurate placement of the needle in the same plane as the scan. However, it is sometimes desirable to have the needle enter in a different plane due to overlying structures in the plane of the scan, in which case a biopsy guide cannot be used. Biopsy guides also limit the angle of insertion of the needle, and the entry site is usually 2 to 3 cm from the scan head. Therefore for superficial lesions or those in the center of the scan, a biopsy guide should not be used. Furthermore, when the needle is in a rigid biopsy guide, inadvertent trauma to the organ may result if the patient moves or takes a deep breath.
A small amount of sterile coupling gel or water-soluble lubricant is placed on the skin, and the ultrasound examination is repeated to verify the needle path. A small stab incision is made in the skin at the needle insertion site. Automated needles are generally preferred because they can be easily operated with one hand. Therefore the needle must be loaded before entry into the abdomen. While one hand maneuvers the transducer, the other hand advances the needle into the organ under direct ultrasound visualization. If the needle tip cannot be seen, gentle movement of the transducer should allow visualization. To allow distinction of the needle from other echogenic structures in the image, the needle can be gently moved in and out. Ideally this should be minimal and just enough to move the organ within the abdominal cavity rather than moving the needle within the organ. If a spinal needle is used, moving the stylet in and out of the stationary needle increases the echogenicity and visualization of the needle tip without creating tissue trauma. Occasionally the needle cannot be visualized. Indirect evidence of organ puncture can be used, including movement of the organ or visualization of motion at the organ border. The needle is directed so the trajectory will avoid other structures when it is fired. Care must be taken to prevent going too deep with the needle, or it will be seen to penetrate the diaphragm and enter the thoracic cavity. Once the biopsy specimen is obtained, the needle is removed. The core of liver should be resting within the specimen notch of the needle. A 25-gauge needle is then carefully used to transfer the tissue into culture broth, onto a slide for impression cytologic study, and/or into 10% formalin. The number of biopsy specimens obtained will depend on the coagulation status of the patient, types of diagnostic tests planned, and adequacy of tissue retrieved. After completion of the procedure, an ultrasound examination is performed to check for excessive hemorrhage. External digital pressure or an abdominal compression wrap may be used to control hemorrhage. Possible complications of this technique are similar to those described above for the blind transabdominal percutaneous biopsy.
Laparoscopy-Guided Biopsy
The main advantage of laparoscopy-guided biopsy is the ability to visualize the liver, biliary tree, and other abdominal organs. With experience the gallbladder can be examined, palpated with a blunt probe, and the bile duct traced to its entry into the duodenum. In this manner it can be determined whether there is a common bile duct or cystic duct obstruction. In addition, because focal lesions on the liver can be directly visualized, an appropriate biopsy site can be selected, and other intrahepatic structures such as the gallbladder and portal vessels can be avoided. Hemorrhage can be observed and, when excessive, controlled with direct compression with a blunt probe over the biopsy site, with electrocautery, or with application of gel foam. Compared with laparotomy, there is much less anesthetic time.With experience the operator can perform a complete laparoscopic examination and obtain multiple biopsy specimens in 10 to 15 minutes in most cases, and because there is only a 1.0-cm incision, there is much less risk for wound dehiscence. Disadvantages of laparoscopy are the requirement for a general anesthetic and the need for expensive equipment. Details of the equipment and techniques for performing laparoscopy are found in Chapter 3.
Potential complications of the procedure include those related to a general anesthetic, excessive bleeding, overdistention of the abdomen with gas, air embolism, and a tension pneumothorax if the diaphragm is inadvertently punctured (as abdominal gas enters the thoracic cavity). In my experience these complications are extremely rare.
Laparotomy Biopsy
Advantages of a laparotomy biopsy include the ability to view the entire abdominal cavity and to treat disease when surgically correctable. Therefore one can visualize and select the biopsy site. If there is excessive hemorrhage, it can be controlled. However, if there is a known coagulopathy, laparotomy is not advised because of the size of the incision and therefore high potential for additional bleeding. In this setting laparoscopy is the preferred method for obtaining the biopsy specimen. Laparotomy offers the additional advantage of being able to obtain large biopsy specimens. Disadvantages of laparotomy biopsy include the requirement for a long general anesthetic and therefore more risk to the patient. In addition, there may be poor wound healing if severe hypoalbuminemia is present and therefore increased risk for dehiscence.
The techniques to obtain hepatic tissue at laparotomy are beyond the scope of this chapter. The reader is referred to surgical textbooks for further information on this subject.
Postbiopsy Monitoring
The most important complication to monitor for following hepatic biopsy is excessive hemorrhage and subsequent hypovolemic shock. Hematocrit and total solid measurements are an unreliable means of identification of hemorrhage, because several hours are necessary for extravascular fluid redistribution to occur following acute bleeding and therefore changes in hematocrit are delayed. By the time the hematocrit drops, it might be too late to begin a life-saving blood transfusion. Therefore clinical monitoring, including assessing mucous membrane color and capillary refill time,
is most helpful. Intravenous fluid support and/or blood transfusion may be necessary to treat hypovolemic shock. If the patient has a known coagulopathy before biopsy, crossmatching should be performed and compatible blood made available. If at all possible, blood transfusion with stored blood should be avoided because it contains a high concentration of ammonia resulting from elaboration from red blood cells. Therefore fresh blood should be collected in plastic collection bags (platelets stick to glass, and glass activates factor XII and can therefore worsen DIC). In my experience if there are no complications from hemorrhage within 5 hours of the biopsy procedure, the patient is unlikely to experience bleeding problems.
Biopsy Specimen Handling
Hepatic biopsy samples are often quite friable and need to be handled with care to avoid excessive fragmentation. Depending on the biopsy method, the amount of tissue submitted may be small. The pathologist must be familiar with interpreting small samples. Therefore representative sections of the liver must be submitted. A portion of all hepatic biopsy samples should be cultured for both aerobic and anaerobic bacteria. Therefore appropriate culture media should be available. Bacterial infection of the liver can be a primary event or can be secondary to abnormal clearance of portal bacteria associated with abnormal hepatic reticuloendothelial cell function.
A portion of the biopsy sample can be placed on a glass slide to obtain an impression smear for cytologic study before placing the sample in 10% formalin. Several diseases can be readily diagnosed by cytologic examination before histopathologic confirmation, including feline hepatic lipidosis, hepatic malignant lymphoma, hepatic carcinoma, and fungal hepatitis.
In addition to routine hematoxylin-eosin (H & E) staining, copper stains may be helpful, including orcein, rhodamine, rubeanic, or Timm's stains. Use of these stains is indicated in suspected cases of primary copper-storage diseases (as occurs in the Bedlington terrier and West Highland white terrier) or to assess whether chelation therapy will be necessary in cases of chronic active hepatitis (especially in Doberman pinschers). It is recommended that copper stains be requested anytime a hepatic biopsy sample is obtained from any of these breeds.
Biopsy Specimen Interpretation
Controversy exists as to whether fine needle aspirates, needle biopsy specimens, laparoscopic “spoon” biopsy specimens, and surgical wedge biopsy samples give similar results. There appears to be strong institutional bias in regard to this question, usually depending on expertise and experiences of the entire team of clinicians involved (e.g., internist, radiologist, pathologist). My impression is that fine needle aspirates are only helpful for certain conditions, such as to confirm the diagnosis of hepatic lipidosis and certain types of neoplasms (lymphoma and mast cell tumor). However, fine needle aspirates usually fail to define lobular architecture, the location of inflammation within the lobule, degree of fibrosis, degree of cholestasis, vascular pathologic condition, and so on. Fine needle aspirates are also often unreliable in mixed lesions. A recent study comparing fine needle aspirates for cytologic study with surgical biopsy specimens suggested that cytologic examination is unreliable in all categories of hepatic disease in dogs and cats. Needle biopsies may also be limited in their usefulness in some situations as well, depending on the quality and quantity of the biopsy samples obtained. I occasionally receive results of needle biopsy specimen analysis that do not adequately explain the clinical and laboratory features of the patient. It is likely that some of these cases simply have sampling error. Needle biopsy specimens procured via ultrasound guidance are typically obtained from the portion of liver that can be seen best (usually the left medial lobe), with minimal attempts to sample other sites. Geographic diversity and the limited sample size may explain failure in these cases. For example, needle biopsy specimens of regenerative nodules often can be suggestive of a metabolic disorder. Several portal triads need to be included to be of most benefit, often from several areas.A recent study showed only 49% concordance between needle biopsy and surgical biopsy specimen analysis.
Clearly laparoscopic and surgical wedge biopsies give the most information because of the size of biopsy specimens obtained. Caution must be used when obtaining a biopsy sample from the edge of a lobe. There is often an increase in fibrous tissue at the surface due to blending of fibrous tissue of the capsule with portal fibrous tissue. Therefore the center of lobes should be included in sampling with laparoscopic or surgical biopsy procedures. In addition, laparoscopic biopsy allows the sampling of multiple lobes. I typically obtain at least seven “spoon” biopsy specimens with most laparoscopic examinations.
The most common histopathologic abnormalities encountered in the experience of many clinicians are listed in order of frequency in Box 9-10. From a clinical perspective the biopsy specimen analysis has the following purposes:
1. To categorize the disease (inflammatory, neoplastic, degenerative, dysplastic, or metabolic abnormality such as lipidosis or steroid hepatopathy)
2. To establish a specific cause if possible
3. To determine the prognosis
4. To direct institution of appropriate specific therapy
Information that must be determined from hepatic biopsy specimen analysis includes the following:
1. Chronicity (acute or chronic)
2. Severity
3. Involvement of structures within individual lobular units (bile canaliculi, blood vessels and lymphatics, hepatocytes in each major zone of the lobule, or the hepatic capsule)
4. Distribution, severity, and nature of inflammatory cells
5. Degree of degeneration and necrosis
6. Distribution and severity of fibrosis
7. Presence of pigment
8. Vacuolar changes (fat, steroids)
9. Presence of organisms
10. Need for special stains (copper, amyloid, glycogen, or fibrous tissue)
BOX 9-10
Histopathologic Abnormalities Seen in Hepatic Biopsy Specimens (in Order of Frequency)
Vacuolar hepatopathy (steroid hepatopathy) Chronic active hepatitis (dog)
Hepatic lipidosis (cat)
Cholangiohepatitis complex (cat) Neoplasia (lymphoma most common) Focal necrosis with inflammation
Cholestasis
Cirrhosis
Passive congestion (ischemia)
Other