Performing the Electrocardiogram
No single electrocardiographic lead system has been universally accepted for use in large animals. Bipolar leads (I, II, III, base-apex, X, Y, and Z of the orthogonal lead system) and unipolar leads (aVF, aVR, aVL, thoracic) have been described, but the amplitude, duration, and configuration of the different waveforms vary widely depending on an animal's breed, size, body type, and sex.
In addition, there is lability of certain waveforms within each animal depending on its level of exercise, excitement, or organic heart disease. Large animals have a deeply penetrating Purkinje system, and depolarization from the ventricular endocardium to the epicardium occurs explosively and in many directions at once. This period of ventricular activation is responsible for the electrocardiographic criteria that indicate ventricular enlargement in small animals but contributes little to generating the QRS complex of large animals. Establishing specific diagnostic criteria for chamber enlargement in large animal species has been difficult, because changes in the QRS complex are not sensitive or specific for ventricular enlargement.The electrocardiogram (ECG) is used primarily to detect cardiac arrhythmias. For this purpose, a single-channel machine can be used, and the lead system chosen can be any that generates distinctive P, QRS, and T complexes. If an arrhythmia is detected, other leads should be obtained to further characterize the QRS and T complexes and confirm their origin. The lead system should be easy to apply, and the tracing free of artifacts created by muscle tremors, skin movement, shifting of weight, and changes in limb position. Two such leads commonly used to obtain a rhythm strip for the diagnosis of cardiac arrhythmias are the base-apex lead1 and the Y lead of the orthogonal lead system.2 The base-apex lead is attached by placing the positive electrode from one of three standard bipolar leads (lead I, II, or III) on the left thorax in the fifth intercostal space at the level of the elbow or at the location where the apex beat is most readily palpable.
The negative electrode is attached to the skin of the right jugular furrow two thirds of the way from the ramus of the mandible to the thoracic inlet or at the top of the right scapular spine. The ground electrode can be attached to any site remote from the heart. Electrical contact is improved by clipping hair or wetting the skin with alcohol. The base-apex lead ECG is recorded by switching the machine*The author would like to thank Dr. Sheila McGuirk for her original contributions to this article. to the bipolar lead that has been attached to the horse and recording the ECG (Table 30.1). Lead Y is attached by placing the positive electrode over the xiphoid and the negative electrode cranially to the front of the chest. Smartphone-enabled ECGs are useful to obtain a rhythm strip by placing the microphone end of the recording device at a 30-degree angle craniodorsally over the heart in the left fifth intercostal space.3
Continuous electrocardiographic recording over a 24-hour or longer period (Holter monitoring) or with telemetry is also useful for evaluating horses with arrhythmias. Continuous ECG recording can be performed with high-quality sticky electrodes applied to the skin underneath the surcingle, electrode patches that are held against the skin with a surcingle, or electrode patches attached to shaved skin with a cyanoacrylate adhesive and protected underneath a surcingle.4,5 In the latter two situations, a dry sponge may help absorb motion, yielding a cleaner tracing. With sticky electrode patches, the electrodes may be applied directly to the skin or are taped to a small square of cardboard to provide them with some support and embedded in foam to minimize motion artifacts. The best recording with a three-lead system is usually obtained with the left arm electrode placed on the sternum, the right leg electrode on the right side in the fifth intercostal space at the level of the point of the shoulder, and the right arm electrode placed on the left side in the fifth intercostal space at the level of the point of the shoulder.
These electrodes are then held in position with a tight surcingle. The electrodes are connected to a digital recorder that records the animal's heart rhythm for the entire monitoring period (Holter monitor) or a telemetry device that sends the ECG signal back to the receiver to be displayed on a monitor. To obtain an exercising ECG, high-quality sticky electrodes are applied to clean, dry hair. Several ECG placements enable a more motion-free tracing. The positive electrode (left arm) is placed near the left cardiac apex, and the negative electrode (right arm) is near the left shoulder area. The right leg electrode is placed near the positive electrode (left arm), and the ground electrode (right leg) is placed near the left shoulder electrode. Positioning the electrodes so that the negative (right arm) is under the surcingle or girth on the right shoulder region enables lead three to have a larger amplitude on the three-lead telemetry system. With this configuration, the ground electrode is under the surcingle on the left dorsal thoracic region, the positive electrode is over the cardiac silhouette, and the right leg is ventral to this; both electrodes are underneath the surcingle or girth. Electrode placement will vary somewhat with the tack that is applied and whether the horse is being ridden or driven. The entire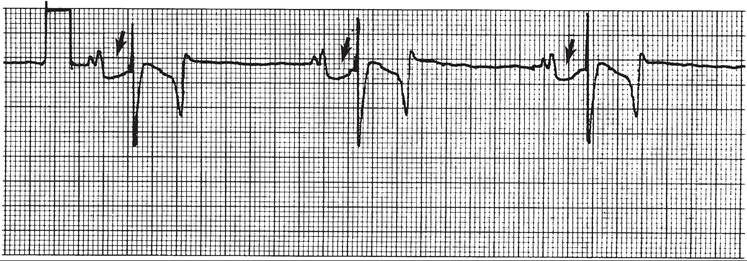
FIG. 30.1 Base-apex lead electrocardiogram recorded from a horse. Arrows point to the atrial repolarization wave (Ta) frequently seen in normal horses. It follows the notched P wave and precedes the QRS complex. Paper speed 25 mm/s, calibration 1 cm/mV
■ TABLE 30.1
Standard Bipolar Electrocardiographic Leads
| Lead | Positive Electrode | Negative Electrode |
| I | Left arm | Right arm |
| II | Left leg | Right arm |
| III | Left leg | Left arm |
recording or monitoring period can be stored on a smart card for subsequent analysis.
The continuous 24-hour Holter ECG is useful for diagnosing arrhythmias that occur intermittently or monitoring cardiac rhythm during exercise for later analysis. Telemetry electrocardiography is useful for real-time cardiac rhythm monitoring during treatment or exercise.In the base-apex lead, the P wave is positive in most horses and ruminants. The P wave is most frequently bifid in horses. In many horses a Ta wave, indicative of atrial repolarization, occurs as a negative deflection after the P wave (Fig. 30.1). The QRS complex begins with a small positive deflection (rS) and is followed by a large negative deflection that terminates in the ST segment. The T wave is variable and can be positive, negative, or biphasic in horses and ruminants. Frequently the appearance of the T wave is variable within one recording. Fig. 30.2 illustrates a typical base-apex ECG recorded from both a cow and a horse at a 25-mm/s paper speed with the gain set at 10 mm/mV.
A systematic approach is used to analyze the ECG. The following step-by-step approach is recommended:
1. Identify all the QRS complexes. Each QRS complex should be followed by a T wave, and the QT interval should be similar for all QRS configurations unless there is a marked change in heart rate. Identify the remaining complexes. Are P waves, “F” (flutter) waves, or “f” (fibrillation) waves present? Are there any artifacts?
2. Determine the atrial and ventricular rates. Are they identical? Is one too fast or too slow? This determines whether there is a tachycardia or bradycardia.
3. Are the P-P and R-R intervals regular? Determine whether an irregular rhythm has underlying regularity that is interrupted by irregular intervals or whether the rhythm is consistently irregular. Second-degree atrioventricular block (AVB) and atrial and ventricular premature beats are arrhythmias with underlying regularity, whereas atrial fibrillation (AF), sinus arrhythmia, and sinus arrest are truly irregular rhythms.
4. Are P waves present? If so, is there a P wave preceding every QRS complex? If not, there are premature depolarizations, ventricular tachycardia (VT), escape beats, or AF.
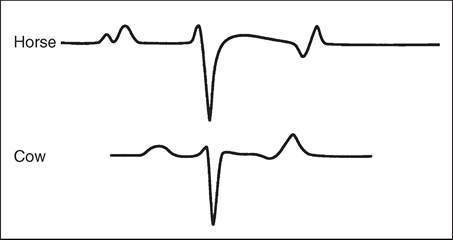
FIG. 30.2 Schematic representation of a typical base-apex lead electrocardiogram recorded from a cow and horse. In horses the P and T waves may be variable in appearance.
Are all P waves followed by QRS complexes? If not, second- degree AVB may be present. Is the resultant P-R interval constant? If not, there may be a wandering pacemaker or first-degree AVB.
5. Are all P waves and QRS complexes identical or normal in contour? If not, this signifies more than one pacemaker, premature depolarizations, or escape beats.