routes of ADMINISTRATION
As a general rule, the closer one comes to the oral route of food intake and digestion, the more efficient is the assimilation and digestion of nutrients and the greater the flexibility in formula composition.
Conversely, the further aboral one gets, the less efficient is the assimilation and digestion of nutrients and the greater the care that must be taken when choosing formula composition. Route of administration also dictates feeding tubeOral
As a general rule, oral feeding is the method of choice if adequate amounts of nutrients can be consumed to meet the patient’s protein and calorie needs. Several techniques have been used to successfully coax a patient to eat. Sending the patient home if the disease state permits and if owners are capable of managing the patient may prove successful. Petting and vocal reassurance is also helpful in stimulating patients to eat; however, it is time consuming (Figure 12-2). Highly palatable foods or food coverings (e.g., gravy) may stimulate appetite; adding water to food increases palatabil- ity for dogs (Figure 12-3).Warming foods to near but not above body temperature (e.g., with a microwave oven) will increase aroma and palata- bility. Nutrition may also be provided by syringe feeding, but the diet must be semiliquid in consistency and there is a risk of aspiration pneumonia (Figure 12-4). Drugs may be used successfully to stimulate appetite sometimes; however, if they do not work immediately, then more aggressive forms of nutritional support should be considered.A list of drugs and their recommended dosages are given in Table 12-3.

Figure 12-2 Petting and vocal reassurance may help stimulate oral intake of food.

Figure 12-3 Using a variety of diets or highly palatable foods may stimulate appetite.
Appetite stimulant drugs are generally not adequate in promoting replacement of a patient’s caloric needs; however, they may provide the stimulus necessary for the patient to resume eating. Appetite stimulants are contraindicated in patients suffering from severe malnutrition or in those patients that cannot tolerate the medication. Diazepam should be used cautiously in patients with preexisting liver disease because its use has been associated with inducing hepatocellular necrosis. Glucocorticoids stimulate appetite; however, they are catabolic and induce diuresis and hepatic lipid accumulation. Megestrol acetate may induce diabetes mellitus, adrenal suppression, and mammary neoplasia in cats. None of these drugs work consistently, and none have been evaluated in a controlled manner.

Figure 12-4 Syringe feeding a semiliquid diet to an adult cat.
In addition to appetite stimulants, patients may be force-fed by hand feeding or syringe feeding. Boluses of food in the oropharynx will stimulate swallowing. Using “meatballs” of canned food or using a syringe may accomplish this. Canned food gruels or convalescent canned veterinary products may be administered via syringe. Force-feeding is easy to perform; however, it may add additional stress to a sick patient. Furthermore, it is difficult to do for more than a couple of days, and it is difficult to meet nutritional needs of large dogs using this technique.
Orogastric Tube
Passing a feeding tube through the mouth into the distal esophagus or stomach is technically easy to do; however, it is usually stressful to adult dogs and cats (Figure 12-5). It is often used to provide nutrition to orphaned puppies and kittens. A 5 Fr infant feeding tube can be used for orphans weighing less than 300 g,an 8 to 10 Fr infant feeding tube can be used for orphans weighing over 300 g, or an appropriate-size, soft, male urethral catheter may be used.
An appropriate size syringe should be used to avoid disconnecting the syringe from the feeding tube to refill it while feeding and to prevent administering formula too rapidly. Once weekly the feeding tube should be clearly marked to indicate the depth of insertion to ensure gastric delivery; that is, the distance from the last rib to the tip of the nose can be measured and marked off on the feeding tube as a guide.To insert an oro- gastric feeding tube in a neonatal puppy or kitten, the clinician passes the feeding tube through the mouth into the stomach. The feeding tube must be in the GI tract and not the respiratory tract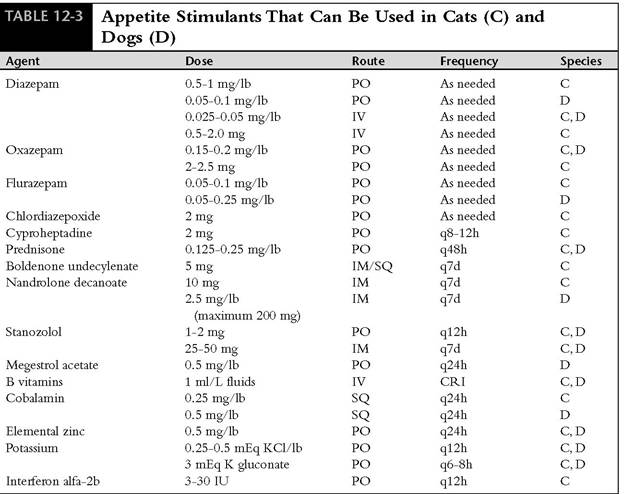
PO, Orally; IV,intravenously; IM, intramuscularly; SQ, subcutaneously; CRI, constant rate infusion.
before feeding; it can often be palpated in the cervical esophagus. If an obstruction is felt while passing the tube before reaching the mark, the tube is in the trachea. After inserting the feeding tube to the premeasured mark, the clinician places the flared end of the tube in a glass of water and observes for bubbles while the neonate breathes. If the feeding tube has been inadvertently inserted

FlGURE 12-5 Orogastric feeding tube placement in an adult cat. into the respiratory tract, bubbles will appear in the water as the neonate breathes. If the tube is properly placed, then the neonate may be fed. When feeding, the clinician fills a syringe with warm formula and fits it to the feeding tube, being careful to expel any air in the tube or syringe, then aspirates back on the tube to make sure there is no residual formula remaining from the previous feeding.When certain that the tube is in the stomach, the clinician slowly administers the formula over a couple of minutes to allow sufficient time for slow filling of the stomach. Regurgitation of formula rarely occurs, but if it does, the feeding tube is withdrawn and feeding is interrupted until the next scheduled meal.
Nasoesophageal/Nasogastric Tube
Nasoesophageal tube placement is an easy, effective, and efficient means of providing enteral nutritional support (Figure 12-6).The availability of small-bore, soft polyvinyl and Silastic feeding

Figure 12-6 Use of a nasoesophageal feeding tube in an adult dog.
tubes (i.e., 3.5 to 5 Fr) and low-viscosity, nutritionally complete liquid diet formulations and patient tolerance of tube placement have made nasoesophageal tube placement a popular avenue for feeding malnourished patients. Nasoesophageal tube placement is indicated in any conscious patient with protein-calorie malnutrition that will not undergo oral, pharyngeal, esophageal, gastric, or biliary tract surgery.
Technique. Local nasal anesthesia, sedation, or light general anesthesia may be necessary for placement of a nasoesophageal tube in dogs and cats. In the majority of cases, topical anesthetic is all that is necessary for proper tube placement. In cats the clinician places 0.5 to 1 ml of 0.5% proparacaine hydrochloride (topical local anesthetic) or in dogs the clinician places 1 to 2 ml of 0.5% proparacaine or 2% lidocaine into the nasal cavity and tilts the head up to encourage the local anesthetic to coat the nasal mucosa (Figure 12-7, A). Application of local anesthetic is repeated to ensure adequate anesthesia of the nasal mucous membrane. If the patient will not tolerate nasal intubation (i.e., if excess stress is required to place the nasoesophageal tube, particularly with debilitated cats), light sedation or a light plane of anesthesia is induced.
Tube. An appropriate-size polyvinyl chloride feeding tube is selected. For cats a 5 Fr, 91-cm tube works best. For dogs between 4.5 and 22 lb, a 5 Fr, 91-cm tube is best, and an 8 Fr, 91-cm tube is best for dogs greater than 22 lb. The clinician estimates the length of tube to be placed in the esophagus or stomach by placing the tube from the nasal planum along the side of the patient’s body to the last rib (Figure 12-7, B).
The distal end of the feeding tube may terminate in the thoracic esophagus or the stomach. Because of the small diameter of the tube, gastroesophageal reflux rarely occurs. If the tube is to terminate in the distal esophagus, the clinician pulls the tube back 1 to 2 cm. A tape butterfly is placed on the tube as a marker once the appropriate measurement has been taken. The tip of the tube is lubricated with 5% lidocaine viscous before passage. The patient’s head is held in a normal functional position (i.e., avoiding hyperflexion or hyperextension).Tube Placement—Cat. The clinician places the tube in the ventromedial aspect of the external nares (Figure 12-7, C) and passes it in a caudoven- tral medial direction into the nasal cavity (Figure 12-7, D).The tube will generally “drop” into the oropharynx and stimulate a swallowing reflex. When the patient swallows, the clinician flexes the patient’s head to facilitate passage of the tube into the esophagus and passes the tube to the predetermined mark.
Tube Placement—Dog. The clinician identifies the prominent alar fold and directs the tube from a ventrolateral location in the external nares to a caudoventral and medial direction as it enters the nasal cavity. When the tube is introduced 0.5 to 1 cm inside the nostril, the clinician feels it contact the median septum at the floor of the nasal cavity. At this moment the clinician pushes the external nares dorsally to facilitate opening the ventral meatus, elevates the proximal end of the tube, and continues to advance the tube (Figure 12-8). Once the tube is inserted an additional 3 to 5 cm, the clinician discontinues pushing the nares dor- sally. The clinician flexes the patient’s head while continuing to insert the tube to facilitate passage through the nasopharynx into the esophagus and inserts the tube to the predetermined measurement mark.
Confirming Esophageal Placement. The clinician confirms esophageal placement by injecting 3 to 5 ml of sterile saline through the tube.
If a cough is elicited, the tube is removed and replaced. Alternately, the clinician places 6 to 12 ml of air in the tube and auscultates for borboryg- mus at the xiphoid to confirm tube placement. Esophageal placement can also be confirmed by taking a lateral thoracic radiograph. If the patient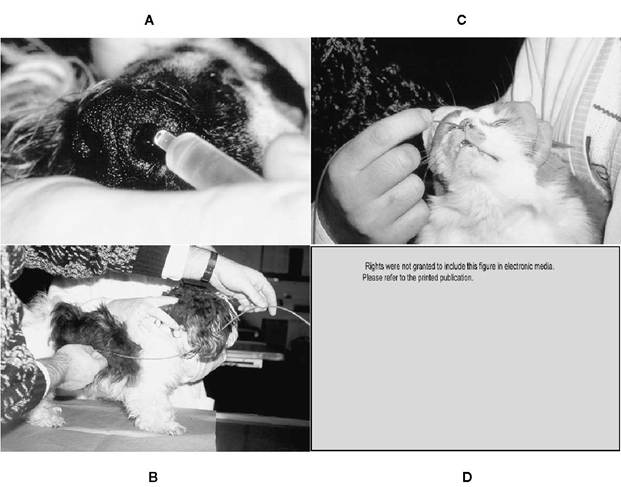
Figure 1 2-7 Nasoesophageal tube placement. A, Instillation of topical anesthetic into the nasal cavity.
B, Estimation of length of tube to be inserted in the patient. C, The feeding tube is inserted into the ventromedial aspect of the nares. D, The feeding tube is inserted through the ventral meatus and nasopharynx into the esophagus. NP, Nasopharynx: NV nasal vestibule; CS, cartilaginous septum; M, maxilla; DM, dorsal meatus; MM, middle meatus: EC, ethmoidal conchae; VNC, ventral nasal concha; DNC, dorsal nasal concha; AF, alar fold. (D from Crowe DT Jr: Clinical use of an indwelling nasogastric tube for enteral nutrition and fluid therapy in the dog and cat, JAmAnim Hosp Assoc 22:675,1986.)
requires general anesthesia, tube placement can be determined visually.
Securing the Tube to the Patient. Once the tube is properly inserted, the clinician should suture it to the nose and head to ensure that it will not be removed by the patient.The tube is secured to the lateral aspect of the nose with the preplaced butterfly tape and the zygomatic arch using 3-0 nylon suture (see Figure 12-6).An encircling suture and Chinese finger-trap friction suture (Figure 12-9, A and B) or cyanoacrylate glue may be used also. Although there may be concern about stimulating a feline’s whiskers using this placement, clinical experience has not found this to be a problem. An Elizabethan collar should be used until it is determined if the patient will tolerate the presence of the tube. Many cats tolerate a nasoesophageal tube without an Elizabethan collar.
Tube Management. The clinician should place a column of water in the tube and cap it with an infusion cap, three-way stopcock, or Christmas tree adapter when not in use; this prevents intake of air, reflux of esophageal contents, and occlusion of the tube by diet. Nasoesophageal tubes can be left in place for several weeks, are well tolerated, and are easily removed; the patient can drink and swallow around the tube; and repeated orogastric intubation is prevented.
Complications. Patients tolerate nasoesophageal feeding tubes fairly well; however, several complications may occur. Premature removal is a common occurrence, particularly if the tube is irritating. Other complications include rhinitis, dacryocystitis, esophageal reflux, vomiting, aspiration pneumonia, and obstruction of the tube. In addition, patients may vomit or regurgitate the tube and inhale the
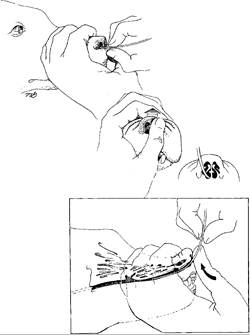
FIGURE 12-8 Nasoesophageal tube placement in dogs. The tip of the feeding tube is directed in a caudoventral- medial direction.The external nares are pushed dorsally to open the ventral meatus. (From Abood SK, Buffington A: Use of nasogastric tubes: indications, technique, and complications. In Kirk RW, Bonagura JD, eds: Current veterinary therapy XI, Philadelphia, 1992,WB Saunders.)
distal end, resulting in aspiration pneumonia if they are fed.
Pharyngostomy tube
Whenever it is necessary to provide nutritional supplementation to an anorexic patient (e.g., suffering protein-calorie malnutrition) or to patients that are unable or reluctant to ingest food orally (e.g., cleft palate, mandibular or maxillary fractures, oral neoplasia), a pharyngostomy tube can be considered (Figure 12-10). Pharyngostomy tubes should not be used for nutritional management of patients with esophageal disorders (e.g., esophagitis, esophageal stricture, recent esophageal surgery, following esophageal foreign body removal, esophageal neoplasia). The major advantage of a pharyngostomy tube over a nasoesophageal/naso- gastric tube is tube diameter; pharyngostomy tubes are generally 12 to 24 Fr, thus accommodating a wider variety of diets. Pharyngostomy tubes should terminate in the distal esophagus; they should never be placed through the lower esophageal sphincter. Generally, esophagostomy tubes are preferred over pharyngostomy because placement and use result in fewer complications.
Technique. Patients should be placed under general anesthesia and the trachea intubated. The patient is positioned in lateral recumbency with the side receiving the pharyngostomy incision uppermost. The clinician aseptically prepares a 4-cm-square area just caudal to the angle of the mandible. The mouth is held open with an oral speculum. The clinician premeasures and marks a 12 to 24 Fr polyvinyl chloride feeding tube from the exit point of the tube in the pharynx to the level of the seventh or eighth intercostal space, ensuring esophageal placement. The clinician places an index finger into the pharynx, near the base of the tongue, and palpates the epiglottis, arytenoid cartilages, and hyoid apparatus (Figure 12-11, A). The index finger is flexed toward the lateral aspect of the neck, and the junction of
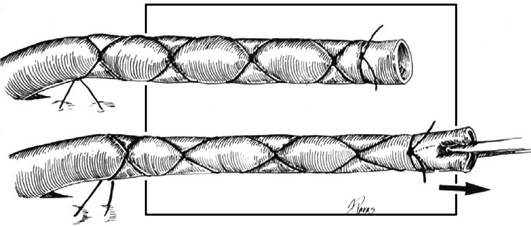
Figure 12-9 A, Schematic demonstrating placement of a Chinese finger-trap friction suture.
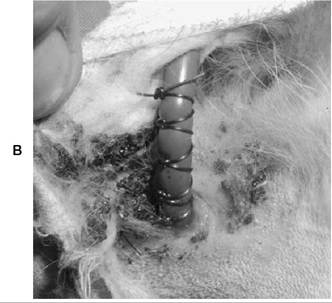
Figure 12-9, cont'd B, Chinese finger-trap friction suture used to secure a pharyngostomy feeding tube.

Figure 12-10 A pharyngostomy feeding tube in an adult male West Highland white terrier.
the intrapharyngeal ostium and laryngopharynx is identified; this is the proper location for the pharyngostomy tube exit (Figure 12-11, B). Enough pressure is gently applied to the lateral pharyngeal wall to create an externally visible bulge. An Eld device or large curved forceps (e.g., Carmalt or Doyen) should be used to maintain the bulge. A 1- to 2-cm skin incision is made over the bulge, and curved forceps are used to bluntly dissect subcutaneous tissue, pharyngeal muscle, and pharyngeal mucosa until the forceps become visible. If an Eld device is used, see esophagostomy tube placement for technique. The clinician uses forceps to grasp the tip of the pharyngostomy tube and pull it through the incision, into the oral cavity, and out of the mouth. The tip of the tube is reinserted into the mouth and passed into the midesophagus (i.e., premarked location on the feeding tube) (Figure 12-11, C).A stylet is generally not necessary for placement in the esophagus. The tube is secured to the patient’s neck at its exit point with a Chinese finger-trap friction suture technique (see Figure 12-9, A and B).The clinician places a column of water in the tube and caps it with a 3-ml syringe when not in use; this prevents intake of air, reflux of esophageal contents, and occlusion of the tube by diet.When the tube is no longer required, the clinician cuts the Chinese finger-trap friction suture, pulls the tube, and allows the pharyngeal wound to heal by contraction and epithelialization.
Complications. If the pharyngostomy tube is placed ventral and medial to the intrapharyngeal ostium and laryngopharynx, partial airway obstruction, coughing, and gagging may result. If the tube is improperly placed (i.e., through the lower esophageal sphincter), reflux esophagitis and stricture may occur.Vomiting the tube has also been reported. Because of the lower incidence of complications, esophagostomy tubes are preferred.
Esophagostomy Tube
Esophagostomy tube feeding is indicated in anorexic patients with disorders of the oral cavity or pharynx or anorexic patients with a functional GI tract distal to the esophagus (Figure 12-12). Esophagostomy tube placement is contraindicated in patients with a primary or secondary esophageal disorder (e.g., esophageal stricture, following esophageal foreign body removal or esophageal surgery, esophagitis, megaesophagus).
Tube Placement. Patients should be placed under general anesthesia and the trachea intubated. The patient is placed in right lateral recumbency with left side uppermost. The tube can be placed on either the right or left side of the mid- cervical region; however, the esophagus lies slightly left of midline, making left-sided placement more desirable. The clinician aseptically prepares a 4-cm-square area along the left lateral midcervical area. The neck is slightly extended and the mouth held open with a mouth speculum. The clinician premeasures and marks a 14 to 24 Fr polyvinyl chloride or Silastic feeding tube (i.e., 20 to 24 Fr for dogs and 14 to 18 Fr for cats) from the level of the midcervical region (i.e., exit point of
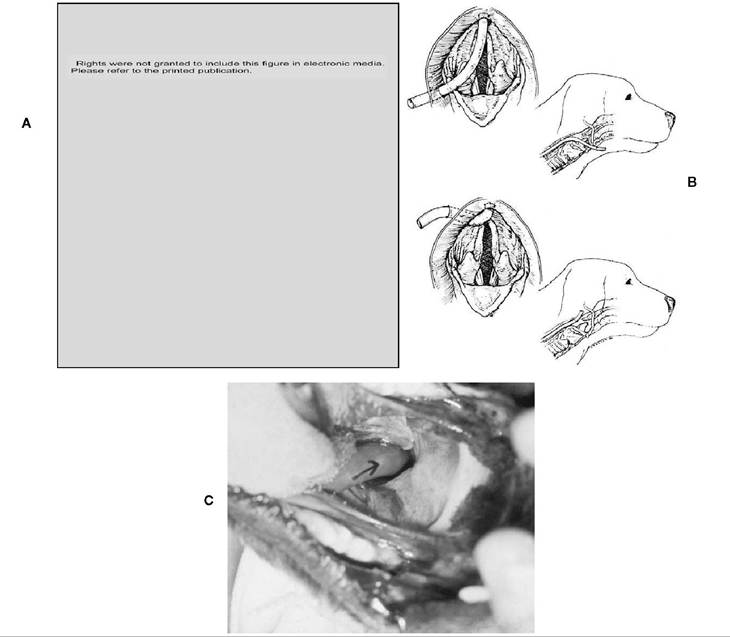
FIGURE 12-11 Pharyngostomy tube placement. A, Anatomic location for tube placement in the lateral pharyngeal wall.The white circle indicates the appropriate site for tube placement. (From Crowe DT Jr, Downs MO: Pharyngostomy complications in dogs and cats and recommended technical modifications: experimental and clinical investigations,JAAHA 22:493,1986.) B, Top: Improper placement of the tube exiting cranial to the epihyoid cartilage results in interference with function of the epiglottis and hyoid apparatus. Bottom: Proper placement of the tube exiting caudal to the hyoid apparatus. (From Crowe DT Jr: Nutrition in critical patients: administering the support therapies, Vet Med 84:162, February 1989.) C, The tip of the feeding tube exiting the oral cavity is grasped with forceps and directed into the esophagus.
feeding tube) to the level of the seventh or eighth intercostal space, ensuring thoracic esophageal placement. The clinician enlarges the two lateral openings of the feeding tube or cuts off the distal rounded end of the feeding tube to encourage smoother flow of blended diets. There are two techniques that can be used to place esophagos- tomy tubes: one method involves using an Eld percutaneous gastrostomy feeding tube placement device (Eld device), and the second involves using long curved forceps similar to pharyngostomy tube placement except caudal to the larynx.
Eld Gastrostomy Feeding Tube Placement Device Technique. An Eld device can be used to place an esophagostomy feeding tube.
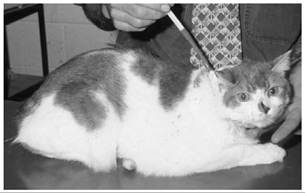
Figure 12-12 An esophagostomy feeding tube in an adult domestic shorthair cat.
The clinician places the oblique tip of the instrument shaft through the oral cavity and into the esophagus to the level of the midcervical region (i.e., equal distance between the angle of the mandible and thoracic inlet) and palpates the tip as it bulges the cervical skin. A small skin incision is made over the device tip (Figure 12-13, A1, A2, and A3). The clinician activates the spring-loaded instrument blade until it penetrates the esophageal wall, cervical musculature, and subcutaneous tissue and is visible through the skin incision. The clinician carefully enlarges the incision in the subcutaneous tissue, cervical musculature, and esophageal wall with the tip of a No. 15 scalpel blade to allow penetration of the instrument shaft (Figure 12-13, B1 and B2). A 2-0 nylon suture is placed through
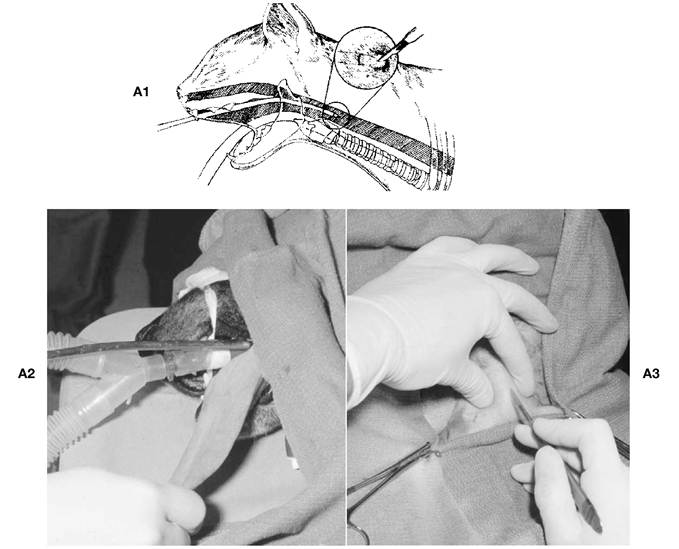
Figure 12-13 A, Esophagostomy tube placement: Eld PGFT applicator. 1,The applicator is passed through the oral cavity into the mid to proximal esophagus. A small skin incision is made in the lateral cervical region over the tip of the applicator. 2 and 3, Photographs illustrating these steps.
Continued
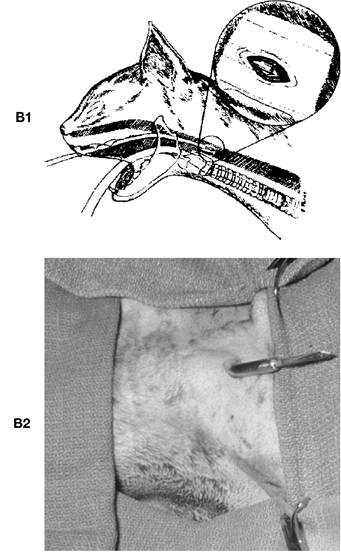
Figure 12-13, cont'd B, 1,The skin incision is enlarged in order to allow exteriorization of the applicator. 2, Photograph illustrating this step.
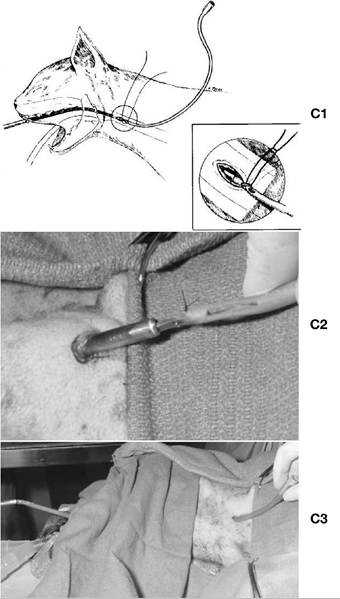
the side holes of the feeding tube and through the hole in the instrument blade. The suture is tightened until the tip of the instrument blade and feeding tube tip are in close apposition (Figure 12-13, C1, C2, and C3).The instrument blade is retracted into the instrument shaft so the feeding tube tip just enters the instrument shaft (i.e., deactivating the instrument blade). Sterile water-soluble lubricant is placed on the tube and instrument shaft.The clinician retracts the instrument and pulls the feeding tube into the oral cavity to its predetermined measurement.The 2-0 nylon suture is removed to free the feeding tube from the instrument.
Curved Forceps Technique. Placement of an esophagostomy tube using curved forceps is
FIGURE 12-13, cont'd C, 1,The feeding tube is attached to the applicator blade and retracted into the esophagus.The applicator with the feeding tube attached is then removed, pulling the feeding tube through the oral cavity. 2 and 3, Photographs illustrating these steps.
done in a manner similar to placement using the Eld device (Figure 12-14, A, B, and C).The patient is positioned in right lateral recumbency, and the curved end of the forceps is passed through the oral cavity into the midcervical esophagus. The ends of the forceps are palpated, and a skin incision is made over the end.The incision is continued through the subcutaneous tissue and esophagus, and the tips of the forceps are exteriorized. The distal end of the feeding tube is
FIGURE 12-14 Esophagostomy tube placement: curved forceps.
A, A long curved forceps is inserted through the oral cavity into the mid to proximal esophagus. The tip of the forceps is palpated, and a small skin incision is made over the tip.
B, The incision is extended through the underlying subcutaneous tissue and musculature into the lumen of the esophagus, and the curved forceps are exteriorized through the incision.The feeding tube is grasped by the curved forceps. C, The forceps and feeding tube are retracted into the esophagus and out of the oral cavity. (From Levine PB et al.: Esophagostomy tubes as a method of nutritional management in cats: a retrospective study,JAm Anim Hosp Assoc 33:405,1997.)
grasped with the forceps, and the forceps are retracted into the oral cavity.
Redirection of Tube. With either method, using the Eld device or using curved forceps, the distal end of the tube exits the oral cavity and the flared end of the feeding tube exits the midcervi- cal esophagus. The next step is to redirect the distal end of the feeding tube so that it terminates in the thoracic esophagus. There are two methods that the clinician can use to accomplish this: one involves using a stylet or hemostat to advance the distal tip of the catheter into the esophagus, and the second involves inserting a stylet down the shaft of the feeding tube. In the dog the clinician places a stylet through one of the side holes of the feeding tube and against its tip.The feeding tube is lubricated and advanced into the esophagus until the entire oral portion of the tube disappears. The clinician gently retracts the stylet from the oral cavity, being careful to ensure its release from the feeding tube (Figure 12-15, A and B). In the cat the
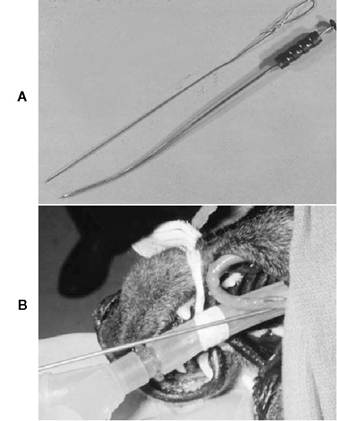
FIGURE 1 2-15 Esophagostomy tube placement: redirection of tube. A, Photograph of Eld PGFT applicator and stylet used to facilitate redirection of esophagostomy tube. B, The stylet is inserted through one of the side holes of the distal end of the esophagostomy tube and is used to redirect the feeding tube caudally in the esophagus.
distal end of the feeding tube is directed toward the stomach, the tube can be inserted to the premeasured mark (Figure 12-16, B3). The distal end of the feeding tube should terminate in the distal esophagus.
Securing the Tube. The clinician secures the tube to the cervical skin with a Chinese finger-trap friction suture of Novofil (see Figure 12-9, A and B).The exit point of the tube can be left exposed or loosely bandaged. A column of water is placed in the tube, and the exposed end capped with a 20- gauge hypodermic needle cap; this prevents intake of air, reflux of esophageal contents, and occlusion of the tube by diet. Most patients tolerate the tube without the need of an Elizabethan collar. Esophagostomy tubes can be removed immediately after placement or left in place for several weeks to months. The tube exit site should be periodically cleaned with an antiseptic solution. Tube removal is performed by cutting the Chinese finger-trap friction suture and gently pulling the tube. No further exit wound care is necessary; the hole seals in 1 to 2 days and heals in 3 to 5 days.
Advantages and Disadvantages. Advantages of esophagostomy tube feeding include the following: the tube is easily placed;
Righls wore not grunted to Includo Ihis Ilguro in electronic medln.
clinician should NOT use a stylet. The feeding tube is simply advanced into the esophagus with fingers or a mosquito hemostat until the entire portion of the tube disappears. The clinician must be sure that the tube is placed to the level of its premeasured mark. In the second technique an endotracheal tube stylet is passed into the proximal end of the feeding tube and is used to facilitate directing the distal end of the feeding tube in an aboral direction (Figure 12-16, A and Bl).The end of the stylet should not protrude beyond the end of the feeding tube.The clinician gently retracts the feeding tube with the stylet inserted from the mid- cervical hole while placing gentle upward pressure on the tube (Figure 12-16, B2). As the feeding tube is slowly retracted, the distal end of the tube will be redirected toward the distal esophagus by sliding the distal end of the tube along the opposite esophageal wall. Once the
Figure 12-16 A, Esophagostomy tube placement: alternate technique for redirection of tube. A stylet is inserted into the lumen of the feeding tube so that the tip of the stylet is near but not through the end of the tube.The tube and stylet are slowly retracted while upward pressure is applied.The end of the feeding tube is redirected in the esophagus so that it can be inserted into the distal esophagus. (From Rawlings CR: Percutaneous placement of a midcervical esophagostomy tube: new technique and representative cases,JAm Anim Hosp Assoc 29:526,1993.)
Continued
FIGURE 12-16, cont'd B, Photographs illustrating redirection of the esophagostomy feeding tube. 1,The stylet is inserted into the lumen of the feeding tube so that the stylet tip is near but not through the end of the tube. 2, The feeding tube and stylet are slowly withdrawn so that the tip of the feeding tube can be redirected toward the thoracic esophagus. 3,The feeding tube and stylet are inserted caudally in the esophagus so that the end of the feeding tube terminates in the thoracic esophagus.
tubes are well tolerated by the patient; large-bore feeding tubes (greater than 12 Fr) can be used, allowing use of blended diets; tube care and feeding is easily performed by the owner; patients can eat and drink around the tube; and tube removal can be performed anytime after placement. Esophageal tube placement eliminates coughing, laryngospasm, or aspiration occasionally associated with pharyngostomy tubes. The major disadvantage of an esophagostomy tube is the need for general anesthesia during placement.
Complications. Complications associated with esophagostomy tube placement include early removal by the patient or vomiting the tube. Two cases of esophageal perforation in cats have been reported. This was thought to be due to placement of the tube with a stylet. Esophageal perforation has not occurred since eliminating the stylet from placement protocol. Esophageal perforation has not been reported in the dog. No significant long-term complications have been reported (e.g., esophagitis, esophageal stricture, esophageal diverticulum, or subcutaneous cervical cellulitis). Reflux esophagitis can occur from improper tube placement (i.e., through the lower esophageal sphincter) or esophageal irritation from the tube itself (Figure 12-17). Midesophageal placement of silicone rubber tubes greatly reduces the incidence of esophageal injury and eliminates reflux esophagitis.
Gastrostomy Tube
Tube gastrostomy is indicated in anorexic patients with a functional GI tract distal to the esophagus or patients undergoing operations of the oral cavity, larynx, pharynx, or esophagus (Figure 12-18). Gastrostomy tube placement is contraindicated in patients with primary gastric disease (e.g., gastritis, gastric ulceration, gastric neoplasia) or disorders
Figure 12-17 Lateral cervical radiograph of an esophagostomy feeding tube in an adult dog.The end of the feeding tube terminates in the thoracic esophagus and does not traverse the lower esophageal sphincter. (From Rawlings CR: Percutaneous placement of a midcervical esophagostomy tube: new technique and representative cases.JAm Anim Hosp Assoc 29:526,1993.)

Figure 12-18 Percutaneous endoscopically placed gastrostomy feeding tube in an adult cat with idiopathic hepatic lipidosis.
causing uncontrolled vomiting and in comatose patients. Advantages of gastrostomy tube feeding include ease of tube placement, patient tolerance, use of large-bore feeding tubes, ease of tube care and feeding by the owner, and the fact that oral feeding can commence while the tube is in place. Disadvantages of gastrostomy tube feeding include the following: use of specialized equipment may be necessary (e.g., endoscope, special tube placement instruments), general anesthesia is required, feeding cannot be initiated the first 12 hours after tube placement, and, depending upon placement technique, tubes must remain in place for a minimum of 7 to 14 days before removal (in order to encourage adhesion formation between stomach and abdominal wall).
Tube Placement. Gastrostomy feeding tubes may be placed without visualization (using the stomach tube technique, Eld feeding tube placement device, or Cook feeding tube placement device) or with visualization (using endoscopy or surgery). Gastrostomy tubes placed surgically may be done with or without gastropexy. Gastrostomy tubes are usually placed under general anesthesia with the patient positioned in right lateral recumbency. For all techniques except placement through a midline laparotomy, the left paralumbar fossa is clipped and prepared aseptically. Drapes are not necessary unless a surgical approach is used. Gastrostomy feeding tubes should exit the left lateral abdominal wall approximately 1 to 2 cm caudal to the costochondral arch and approximately one third of the way dorsal from the ventral abdominal wall. This results in the tube being located along the gastric fundus cranial to the spleen and caudal to the liver.
Technique
Percutaneous Without Visualization
Placement of gastrostomy tubes with visualization is advised when possible because direct visualization is associated with potentially fewer complications; however, gastrostomy feeding tubes can be placed safely without visualization.
Stomach Tube Technique
A gastrostomy tube placement device can be prepared by purchasing a length of vinyl or stainless steel tubing from a hardware store (Figure 12-19, A). The length of the tubing is determined by measuring the distance from the nasal planum to the iliac crest and adding 15 cm.The outer diameter of the tube ranges from 1.2 cm (patients weighing less than 25 lb) to 2.5 cm for dogs weighing more than 55 lb.The distal tip of a stainless steel tube can be flared and deflected 45 degrees to the long axis of the tube to help displace the body wall laterally. The patient is anesthetized and positioned in right lateral recumbency. The lubricated tube is passed through the mouth and into the stomach. The tube is advanced until the end of the tube displaces the stomach laterally. Positioning the patient with its head over the edge of the table and lowering the proximal end of the tube will facilitate identifying the tube tip through the body wall (Figure 12-19, B).A stab skin incision is made over the distal end of the tube, and a 14- gauge hypodermic needle or an over-the-needle intravenous catheter is introduced percutaneously into the lumen of the tube while holding the distal tip of the tube between two fingers. Proper positioning of the catheter is confirmed by moving the hub from side to side and feeling the catheter tip strike the inside of the tube. A guide wire prepared from a monofilament banjo string or cerclage wire is threaded through the needle or catheter, into the tube, and out of the mouth of the patient (Figure 12-19, C and D).The tube and catheter are removed, and the wire is attached to a gastrostomy tube, which is secured (Figure 12-19, E). Securing the gastrostomy feeding tube to the wire is accomplished by cutting off the flared end of the mushroom-tipped catheter (Figure 12-19, F ).An intravenous catheter or 5-ml pipette tip is fed over the wire at the oral cavity. Two V-shaped notches are then cut opposite each other at the proximal end of the gastrostomy tube.The feeding tube is tied to the wire, and the notched end of the feeding tube is planted firmly in the flared end of the intravenous catheter or pipette tip.The feeding tube and catheter/pipette tip are lubricated. A long
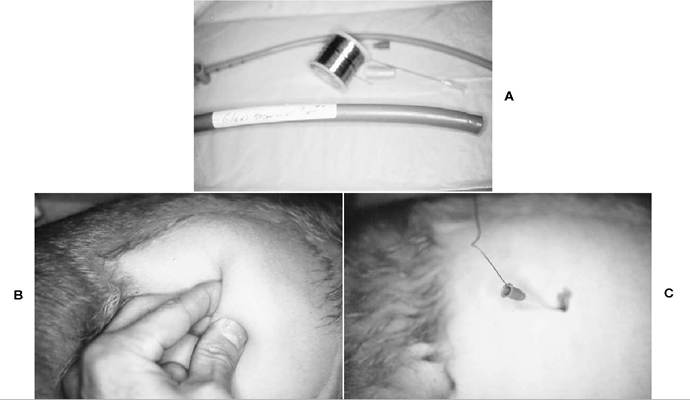
FIGURE 12-19 Gastrostomy tube placement without visualization: stomach tube. A, Equipment required to insert a gastrostomy feeding tube without visualization using a stomach tube.The stomach tube may be hard plastic or metal. A length of wire is also necessary for placement. B, The stomach tube is inserted through the oral cavity and esophagus into the stomach.The end of the tip in the stomach is palpated through the abdominal wall. C, An intravenous catheter has been inserted through a small skin incision into the lumen of the stomach tube, and a wire has been inserted into the catheter and lumen of the stomach tube. (A-C courtesy Dr.T. Glaus, Switzerland.)
Continued
piece of fishing line orVetafil is placed through the side holes of the mushroom end of the feeding tube; this suture should not be tied.This provides a means to recover the feeding tube should problems arise. The tube is then pulled through the esophagus, into the stomach, and through the abdominal wall by placing tension on the wire at the abdominal wall exit site (Figure 12-19, G and H). The skin incision may need to be enlarged to facilitate passage of the feeding tube through the body wall and skin (Figure 12-19, I).The mushroom tip should be palpable through the body wall. The mushroom tip should not be pulled through the body wall. Once the feeding tube is secured, the suture placed through the side holes of the mushroom tip is removed by pulling on one end of the suture.
Eld Feeding Tube Device
Gastrostomy feeding tubes may be placed nonvisu- ally using a device that facilitates placement. One device is the Eld percutaneous gastrostomy feeding tube applicator (Eld device) (Figure 12-20, A). Placement of a gastrostomy feeding tube using the Eld device is performed in a manner similar to using the device to place an esophagostomy tube. The patient is anesthetized and placed in right lateral recumbency; the tube will exit the left lateral abdominal wall in the paralumbar fossa. The Eld device is passed through the oral cavity, down the esophagus, and into the stomach. Gentle downward pressure is applied to the handle to facilitate identification of the distal end of the Eld device in the stomach (Figure 12-20, B).When the distal end of the Eld device is positioned properly in the left paralumbar fossa, a small stab skin incision is made over the distal end. Then the spring-loaded plunger is pushed (Figure 12-20, C), resulting in the sharp point being thrust through the gastric and abdominal wall. A piece of suture (such as Vetafil) or monofilament fishing line is inserted through the hole in the pointed tip of the distal end of the Eld device (Figure 12-20, D), and the distal end is retracted into the outer sheath. The entire device is removed, pulling the suture or
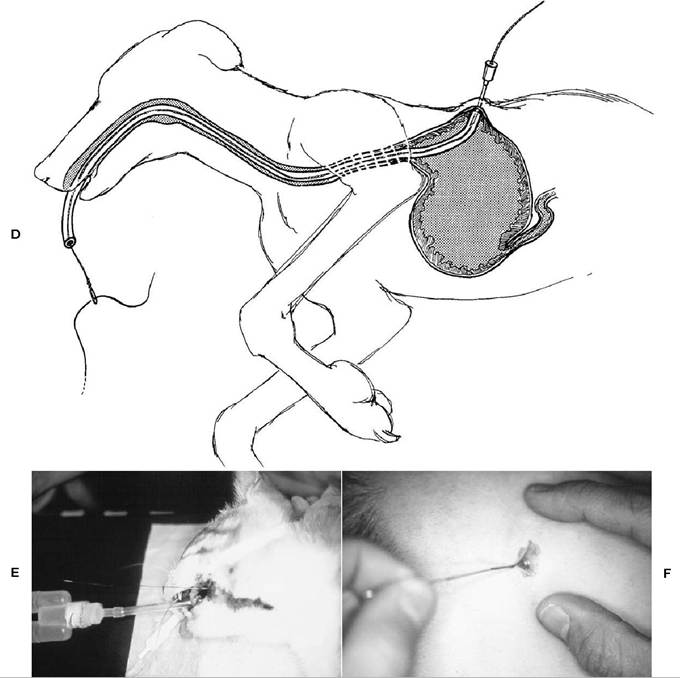
Figure 12-19, cont'd D, Schematic illustrating passage of the wire through the intravenous catheter and lumen of the stomach tube. E, The stomach tube is removed, but the wire is left in place.The wire now enters the lateral abdominal wall, passes through the stomach and esophagus, and exits the oral cavity. F, A tapered catheter is inserted on the end of the wire that exits the oral cavity, and the feeding tube is attached to the wire. (E and F courtesy Dr.T. Glaus, Switzerland.)
fishing line in an antegrade direction. This results in an end of the suture or fishing line exiting the oral cavity and the other end exiting the left abdominal wall. The gastrostomy tube is then secured to the suture exiting the oral cavity (Figure 12-20, E). Securing the gastrostomy feeding tube to the suture is accomplished by cutting off the flared end of the mushroom-tipped catheter. An intravenous catheter or 5-ml pipette tip is fed over the wire at the oral cavity. Two V- shaped notches are then cut opposite each other at the proximal end of the gastrostomy tube. The feeding tube is tied to the suture, and the notched end of the feeding tube is planted firmly in the flared end of the intravenous catheter or pipette tip. The feeding tube and catheter/pipette tip are lubricated. A long piece of fishing line or Vetafil is placed through the side holes of the mushroom
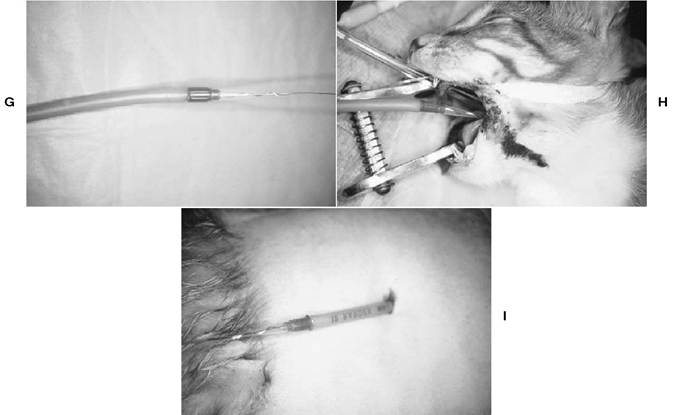
Figure 12-19, cont'd G, Tension is applied to the end of the wire that exits the lateral abdominal wall. H, The feeding tube is pulled into the oral cavity, esophagus, and stomach. I, The lateral abdominal wall skin incision is enlarged, and the feeding tube is exteriorized. (G-I courtesy Dr.T. Glaus, Switzerland.)
end of the feeding tube; this suture should not be tied.This provides a means to recover the feeding tube should problems arise.The tube is then pulled through the esophagus, into the stomach, and through the abdominal wall by placing tension on the suture at the abdominal wall exit site.The skin incision may need to be enlarged to facilitate passage of the feeding tube through the body wall and skin. The mushroom tip should be palpable through the body wall. The mushroom tip should not be pulled through the body wall. Once the feeding tube is secured, the suture placed through the side holes of the mushroom tip is removed by pulling on one end of the suture.
Cook Feeding Tube Placement Device
Use of a Cook feeding tube placement device (Cook device) is another technique for placing gastrostomy feeding tubes without visualization (Figure 12-21). The patient is anesthetized and placed in right lateral recumbency (Figure 12-22). The tube will exit in the left paralumbar fossa, and that area is aseptically prepared. The Cook device is passed through the oral cavity, down the esophagus, and into the stomach (Figure 12-23, A).The distal end of the Cook device is angled and flared, and this end is palpated in the left paralumbar fossa. A stab skin incision is made over the flared end of the Cook device (Figure 12-23, B), and the application needle is passed through the stab incision and body wall into the lumen of the Cook device (Figure 12-23, C). Correct insertion of the needle

Figure 12-20 A, Gastrostomy tube placement without visualization: Eld percutaneous gastrostomy feeding tube (PGFT) applicator.
Continued
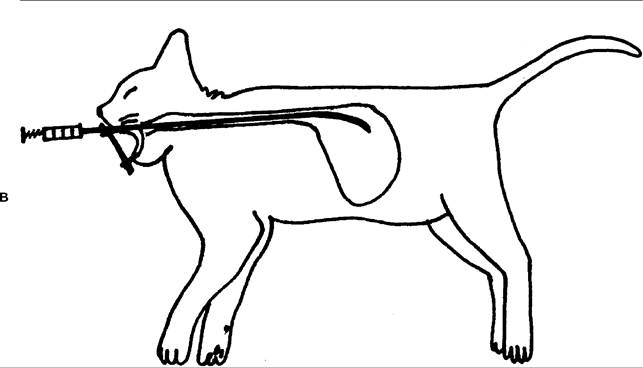

Figure 12-20, cont'd B, The applicator is inserted through the oral cavity and esophagus into the stomach. The tip of the tube is palpated through the lateral abdominal wall. C, When the spring-loaded plunger is depressed, a sharp, pointed end is exposed at the distal tip of the applicator. (B modified from JorVet Eld gastrostomy tube applicator manual, Jorgensen Laboratories, Loveland, Colo.)
is verified by tapping the needle against the inner wall of the lumen of the Cook device. If the flared end of the Cook device cannot be palpated in the gastric lumen or if the spleen appears to be overlying the end, a three-way stopcock can be attached to the proximal end of the Cook device and air can be injected to distend the stomach (Figure 1223, D). A threaded wire supplied with the Cook device is inserted through the needle so that it exits the proximal end of the Cook device where it exits the oral cavity (Figure 12-23, E).The wire is fed so that the threaded end is inserted and exits at the mouth (Figure 12-23, F).The Cook device is then removed. The flared end of a mushroomtipped feeding tube is cut off, and the remaining end of the feeding tube is inserted on the ribbed end of the tapered insertion device (Figure 12-23, G). The insertion device has a threaded end, which is attached to the threaded end of the wire exiting the mouth (Figure 12-23, H). A long piece of fishing line or Vetafil is placed through the side holes of the mushroom end of the feeding tube; this suture should not be tied. This provides a means to recover the feeding tube should problems arise.The insertion device and feeding tube are lubricated, and the tube is then pulled through the esophagus, into the stomach, and through the abdominal wall by placing tension on the wire at the abdominal wall exit site (Figure 12-23, I).The mushroom tip should not be pulled through the body wall (Figure
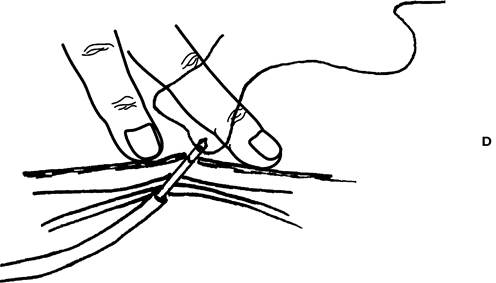
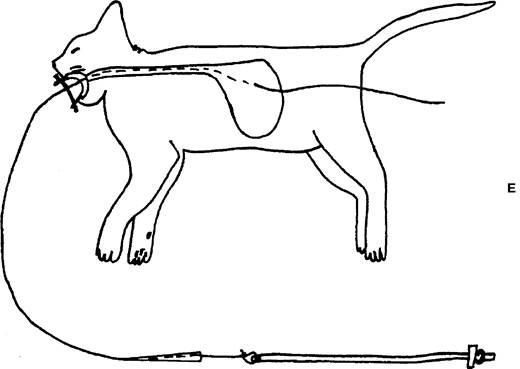
Figure 12-20, cont'd D, The sharp, pointed, distal tip of the applicator is thrust through the stomach and lateral abdominal wall. A piece of suture is threaded through the hole in the tip, and the tip is retracted into the body of the applicator. E, The applicator and attached suture are removed.The feeding tube is attached to the suture. (D modified from and E from JorVet Eld gastrostomy tube applicator manual, Jorgensen Laboratories, Loveland, Colo.)
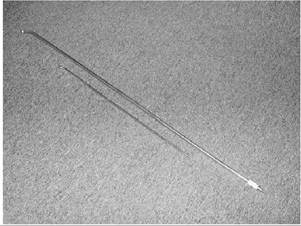
FIGURE 1 2-21 Gastrostomy tube placement without visualization: Cook feeding tube insertion device.
12-23, J). Once the feeding tube is secured, the suture placed through the side holes of the mushroom tip is removed by pulling on one end of the suture.
Advantages and Disadvantages. Advantages of gastrostomy feeding tube placement without visualization include ease of placement and low cost of placement. Disadvantages are the inability to perform surgical gastropexy to ensure an early and
FIGURE 1 2-22 Gastrostomy tube placement without visualization: Cook feeding tube insertion device. The device is passed through the oral cavity and esophagus into the stomach with the patient in right lateral recumbency. A, The device is rotated 90 degrees counterclockwise so that it can pass freely over the base of the heart. B, The catheter needle is inserted through the skin into the flared end of the device at a 45- degree angle to parallel the distal end of the device. (From Mauterer JV Jr et al.: New technique and management guidelines for percutaneous nonendoscopic tube gastrostomy,JAm Vet Med Assoc 205[4]:574,1994.)
permanent seal between the stomach wall and body wall and tube placement cannot be verified visually.
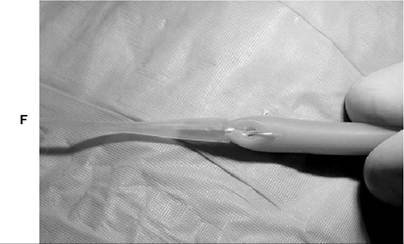
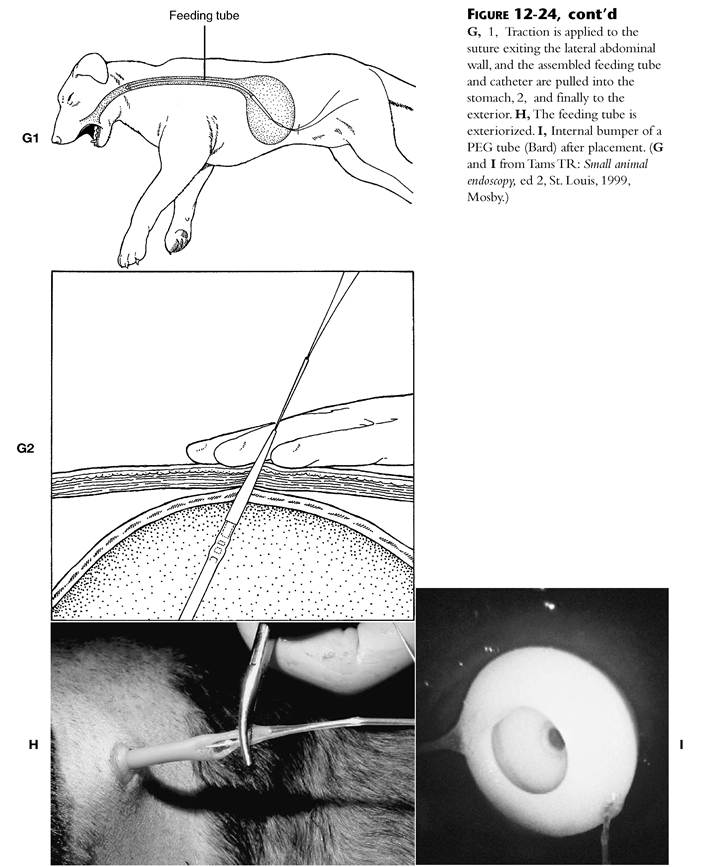
Percutaneous Endoscopic Placement Percutaneous endoscopic tube placement is performed as described for percutaneous surgical placement without gastropexy with the exception that the suture is placed from the left flank out through the oral cavity with the aid of an endoscope. The clinician passes the endoscope into the stomach and insufflates the lumen with air (Figure 12-24, A). A 1-mm skin incision is made in the left flank 1 to 2 cm caudal to the last rib and approximately one third of the distance dorsally from the ventral abdominal wall.An 18-gauge hypodermic needle or an over-the-needle intravenous catheter is passed through the skin incision and into the stomach lumen (Figure 12-24, B and C).The clinician passes a strand of Vetafil through the needle into the stomach, retrieves it endoscopically (Figure 12-24, D), and brings it out through the mouth. Once the strand of suture is entering the left flank and exiting the oral cavity, the feeding tube is placed as described for percutaneous placement without visualization (Figure 12-24, E-I).A retrieval suture is also placed through the side ports of the mushroom-tipped catheter.
Advantages and Disadvantages. The advantage of endoscopic placement is direct visualization of tube placement during the procedure. The disadvantage is inability to perform surgical gastropexy to ensure an early and permanent seal between the stomach wall and body wall.
Percutaneous Surgical Placement With Gastropexy
General anesthesia and standard skin preparation of the left paralumbar fossa is performed. The clinician should instruct an assistant to pass a large- bore stiff plastic stomach tube (e.g., as for decompressing patients with gastric dilatation volvulus) into the stomach. The left flank area is palpated until the bulging end of the stomach tube can be palpated. The tube should be moved to a point 1 to 2 cm caudal to the last rib and 3 to 4 cm ventral to the transverse processes of lumbar vertebrae 2, 3, and 4 and grasped with thumb and finger (Figure 12-25, A-C).The clinician holds the stomach tube in this position and makes a 2-cm skin incision over the end of the tube. Subcutaneous tissues are bluntly dissected to expose the external abdominal oblique muscle. The external abdominal oblique muscle is bluntly dissected in the direction of its fibers to expose the internal abdominal oblique muscle. This muscle is dissected in the direction of its fibers to expose the transversus abdominus muscle.The clinician dissects this muscle in the direction of its fibers and penetrates the peritoneum to expose the wall of the stomach over the tube, being careful not to enter the lumen of the stomach. One or two 3-0 Maxon stay sutures are placed in the exposed stomach wall to ensure that it will not fall back into the abdominal cavity. The orogastric tube can now be removed from the stomach. A purse-string suture is placed in the stomach wall around the proposed tube entry point using 3-0 Maxon. The clinician uses a No. 11 scalpel blade to enter the stomach, places a
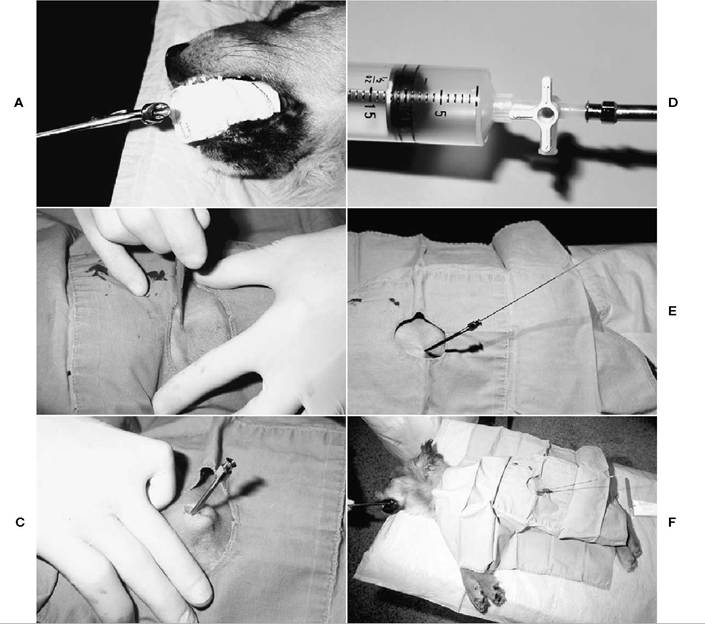
FIGURE 12-23 Gastrostomy tube placement without visualization: Cook feeding tube insertion device. A, The device is inserted through the oral cavity and esophagus into the stomach. B, A small skin incision is made over the left paralumbar fossa. C, The tip of the device located in the stomach is positioned under the skin incision, and the needle is inserted through the lateral abdominal wall and stomach wall into the lumen of the device.
D, A three-way stopcock can be attached to the end of the device for stomach insufflation. E, The threaded wire is inserted through the needle into the lumen of the device until it is visualized at the end of the device inserted into the oral cavity. F, The wire extends from the left lateral abdominal wall through the stomach and esophagus, and exits the oral cavity. (A-F courtesy Dr. R. Bright, Colorado.)
Continued

Figure 12-23, cont'd G, The flared end of the mushroom-tipped feeding tube is removed, and the remaining end of the feeding tube is attached to the ribbed end of the tapered insertion device. H, The tapered insertion device with the mushroom-tipped feeding tube is attached to the threaded end of the wire that exits the oral cavity. I, The wire is retracted through the abdominal wall, pulling the feeding tube through the oral cavity and esophagus into the stomach. J, The tapered insertion device aids in pulling the feeding tube through the stomach and lateral abdominal wall. (G courtesy Dr. R. Bright, Colorado.)
20 to 24 Fr Foley catheter 3 to 4 cm into its lumen, and inflates the bulb. The purse-string suture is secured around the Foley catheter to create an airtight and watertight seal. Gentle traction is placed on the Foley catheter to bring its bulb against the stomach wall and the stomach wall against the abdominal wall. Four or five simple interrupted sutures of 3-0 Maxon are placed from the stomach wall to the body wall to provide a firm gastropexy to the abdominal wall. The clinician closes subcutaneous tissues and skin around the exiting Foley catheter and secures the catheter to the skin with a Chinese finger-trap friction suture of No. 1 Novofil (Figure 12-26, A-C).
Advantages and Disadvantages. Advantages of the surgical technique include the following: the tube is easily placed, the stomach is easily found in an anoretic patient, tube placement is quick, no special equipment is needed to place the tube (i.e., endoscope or feeding tube placement device), surgical gastropexy ensures an immediate and long- lasting seal between the stomach wall and body wall, and confirmation of proper tube placement is performed during placement. Feeding tubes can be safely removed at any time after placement. A disadvantage of this technique is the difficulty of palpating the orogastric feeding tube in the flank of obese patients. Also it requires a surgical and thus more invasive approach to placing a feeding tube.
Surgical Placement Through a Midline Laparotomy
The patient is aseptically prepared for a midline celiotomy. From a ventral midline laparotomy approach, the distal end of a 20 Fr Foley or Pezzer catheter is brought into the abdominal cavity through a stab incision in the left body wall. The ventral surface of the stomach is exteriorized, a purse-string suture is placed in the body of the stomach equidistant between the lesser and greater curvature, and a stab incision is made in the center of the purse-string suture with a No. 11 scalpel blade. The distal end of the feeding catheter is
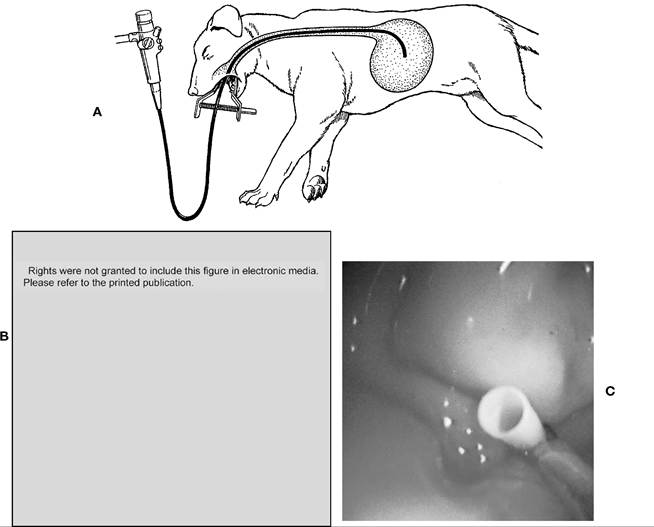
FIGURE 12-24 Gastrostomy tube placement: percutaneous endoscopic placement. A, With the dog in right lateral recumbency, the endoscope is inserted into the stomach and the stomach is distended with air. B, An over-the- needle catheter or hypodermic needle is placed transabdominally into the stomach lumen adjacent to the tip of the endoscope. C, Close-up of an endoscopic snare grasping a 2-inch catheter after the stylet has been removed. (A and C from Tams TR: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby. B from Bright RM, Burrows CF: Percutaneous endoscopic tube gastronomy in dogs, Am J Vet Res 49[5]: 629, 1988.) Continued
placed in the lumen of the stomach, and the pursestring suture is tightened around the catheter. The bulb (i.e., Foley) is inflated with saline, and gentle traction is placed on the catheter to bring the body of the stomach in close apposition to the left body wall. The stomach wall is sutured to the abdominal wall with four or five 3-0 Maxon sutures to provide an early permanent gastropexy. The feeding tube is secured to the skin with a Chinese finger-trap friction suture of No. 1 Novofil. The abdomen is closed routinely (Figure 12-27).
Advantages and Disadvantages. The advantage of gastrostomy tube placement via laparotomy is the ability to suture the stomach wall to the abdominal wall, creating an early permanent gas- tropexy. The major disadvantage is the need to perform a laparotomy to place the tube.This technique is generally performed when exploratory laparotomy is required for diagnosis or treatment of the patient’s primary disorder.
Complications of Gastrostomy Feeding Tubes
Potential complications of gastrostomy feeding tubes relate to mechanical, GI, and metabolic complications. The most severe complication of gastrostomy tube placement is early removal with leakage of gastric contents into the abdominal cavity and subsequent generalized peritonitis.
Figure 12-24, cont'd D, A strand of suture is inserted through the catheter into the stomach lumen and grasped with grasping forceps using endoscopic visualization. (From Bright RM, Burrows CF: Percutaneous endoscopic tube gastrostomy in dogs, Am J Vet Res 49[5]:629,1988.)
These feeding tubes are placed either surgically or percutaneously using a previously placed mushroom-tipped gastrostomy feeding tube. Surgical placement is through a midline celiotomy or through a left flank laparotomy. Placement can also be done using a previously placed gastrostomy feeding tube. A gastrostomy feeding tube is placed as described previously and left in place for 3 to 4 weeks to ensure adhesions between the stomach and body wall. The feeding tube is removed, and the depth of the fistula is measured (Figure 12-29, A).The appropriate LPGFT is chosen. The mushroom end of the LPGFT collapses with the aid of a stylet (Figure 12-29, B).The mushroom tip is collapsed and fed through the fistula into the gastric lumen. The stylet is removed, and the mushroom reexpands in the lumen. A cutaneous flange is inserted onto the LPGFT and used to secure the tube. LPGFTs have one or two internal valves to prevent reflux.
Advantages and Disadvantages. LPGFTs may be used for months to years in dogs and cats. Another advantage is that they lie flush with the skin; therefore bandage material is not required. Valves present in the LPGFTs prevent reflux of gastric contents. Disadvantages of LPGFTs include expense of the tubes, necessity for a previously placed gastrostomy tube or a surgical approach for placement, and the possibility of separating the adhesions while placing the LPGFT.
Ensuring firm placement of the feeding tube that results in an early and permanent gastropexy can prevent this complication. Peristomal infection can also occur if the tube is secured too tightly to the lateral abdominal wall or too loosely, resulting in rubbing of the tube in the gastrocutaneous fistula. GI complications include vomiting and diarrhea. Vomiting is often a result of preexisting disease or administration of food that is less than near body temperature or administering food too rapidly. Potential metabolic complications include intolerance to the diet, hyperglycemia due to stress- induced insulin resistance, and electrolyte imbalances. Protein intolerance may occur if too much protein is administered to a patient in renal or liver failure.
Low-Profile Gastrostomy Feeding Tubes. Low-profile gastrostomy feeding tubes (LPGFTs) can be used for long-term nutritional support (Figure 12-28, A and B). LPGFTs offer the advantage of exiting flush with the abdominal wall.
Percutaneous Castroduodenostomy Tube Percutaneous gastroduodenostomy is indicated in patients with severe gastroesophageal reflux, swallowing disorders, aspiration pneumonia, or persistent vomiting of gastric origin (Figure 12-30, A).
Technique. A percutaneous gastrostomy feeding tube is placed as described previously. A Pezzer catheter feeding tube is used, and the dome-shaped tip of the mushroom end is removed before placement. A strand of 2-0 silk suture is tied to the tip of an 8 to 10 Fr diameter, 60- to 110-cm, duodenal feeding tube with stylet. The duodenal tube is passed through the gastrostomy tube and into the stomach (Figure 12-30, B).The duodenal tube is visualized endoscopically, and the silk suture is grasped with biopsy forceps (Figure 12-30, C).The biopsy forceps are gently retracted into the endoscope port to pull the catheter tip against the endoscope. The clinician repositions the dog in left
Figure 12-24, cont'd e, 1, The end of the suture that exits the oral cavity is passed retrograde through the lumen of an intravenous catheter or pipette tip. 2,The end of the feeding tube opposite the mushroom tip end is modified by removing a V-shaped piece.An 18-gauge hypodermic needle is passed transversely through the tube just under the trimmed portion. The suture and needle are removed as a unit. 3, The suture is tied in a square knot, with the knot pulled deep into the notched end of the feeding tube. 4, The end of the feeding tube is placed into the flared end of the catheter or pipette tip and kept under tension with traction on the suture exiting the lateral abdominal wall. F, The feeding tube is attached to the suture exiting the oral cavity. (E from Bright RM, Burrows CF: Percutaneous endoscopic tube gastrostomy in dogs, Am J Vet Res 49[5]:629,1988.)
Continued
lateral recumbency, passes the endoscope through the pylorus and into the duodenum, advances the biopsy forceps to their full length, and releases the catheter (Figure 12-30, D).The biopsy forceps are replaced in the biopsy port, and the endoscope is slowly removed (Figure 12-30, E). The duodenal feeding tube is secured to the gastrostomy tube by seating the flanged end of the duodenal tube in the gastrostomy tube, and the duodenal tube stylet is slowly removed (Figure 12-30, F).
Advantages and Disadvantages. The advantage of this technique is placement of an enteral feeding tube without the need of laparotomy. Disadvantages include difficulty placing the tube in the duodenum, difficult placement in
patients weighing less than 40 lb, migration of the tube from the duodenum, mechanical obstruction of the tube (e.g., kinking), specialized instrumentation necessary for placement, and the necessity of radiographic assessment for tube placement con- firmation.This technique is technically demanding and is recommended only for veterinarians experienced in endoscopy.
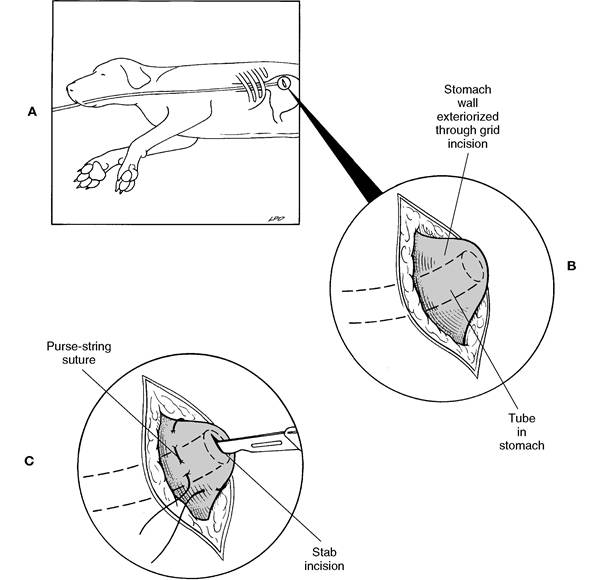
Figure 12-25 Percutaneous gastrostomy tube placement with gastropexy (cont’d in Figure 12-26). A, Pass a large- bore, stiff plastic stomach tube into the stomach. Palpate the end of the tube at the flank. B, Grasp the tube and move it to a point 2 to 3 cm caudal to the thirteenth rib and 2 to 3 cm distal to the transverse processes of the lumbar vertebrae. Secure the tube with thumb and finger, make an incision through the skin and subcutaneous tissue, and bluntly dissect the abdominal muscles to expose the gastric wall over the tube. C, Place a purse-string suture in the gastric wall around the tube and puncture the wall with a scalpel blade. (From Fossum et al.: Small animal surgery, ed 2, St. Louis, 2002, Mosby.)
Enterostomy (e.g., Duodenostomy or Jejunostomy) Feeding Tube
An enterostomy feeding tube is indicated in any patient undergoing oral, pharyngeal, esophageal, gastric, pancreatic, duodenal, or biliary tract surgery in which the intestinal tract distal to the surgical site is functional (Figure 12-31). Surgical patients with a neurologic status that may prevent postoperative feeding or patients with acute pancreatitis that are anticipated to be anorexic for more than 5 days may also be considered candidates for placement of an enterostomy feeding tube. Immediate feeding of a highly digestible, low-bulk diet in patients undergoing colonic surgery can be accomplished using an enterostomy tube. Patients with preexisting protein-calorie malnutrition that must undergo major abdominal surgery are considered candidates for early enteral hyperalimentation via enterostomy.
Technique. A celiotomy is required for placement of an enterostomy feeding tube. A 5 to 8 Fr diameter, 36-inch infant feeding tube in which
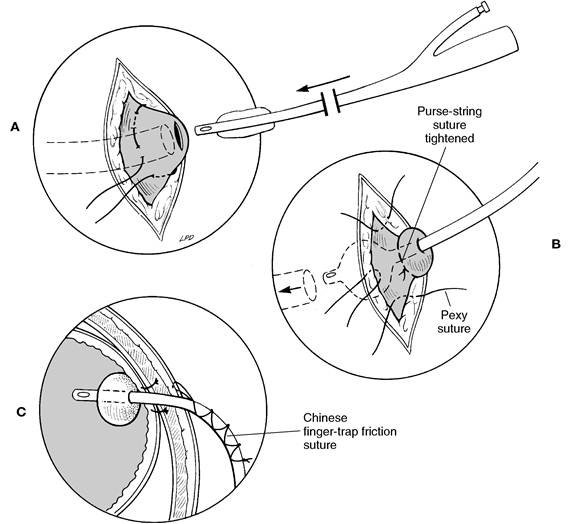
Figure 12-26 Percutaneous gastrostomy tube placement with gastropexy (cont’d from Figure 12-25). A, Place the Foley or Pezzer catheter into the lumen of the stomach and into the tube. B, Tighten the purse-string suture, remove the stomach tube, inflate the bulb of the Foley catheter, and suture the gastric wall to the abdominal wall. C, Note the proper tube placement of the inflated Foley catheter, the gastropexy, and the Chinese finger-trap friction suture to secure the tube in place. (From Fossum et al.: Small animal surgery, ed 2, St. Louis, 2002, Mosby.)
one end can be conveniently capped or a red rubber feeding tube is recommended.The distal tip of the feeding tube is brought into the abdominal cavity through a 2- to 3-mm stab incision on the right or left body wall using a No. 11 scalpel blade. The clinician selects a segment of small intestine, identifies the normal direction of flow of ingesta (i.e., oral to aboral), and ensures the selected segment can be easily mobilized to the feeding tube entrance location on the body wall.A 1- to 1.5-cm linear incision is made through the seromuscular layers of the antimesenteric border of the selected jejunal segment. A 10-gauge hypodermic needle or the point of a No. 11 scalpel blade is used, and the lumen of the jejunum is entered at the most aboral end of the incision. The distal end of the feeding tube is placed through the incision, and 10 to 12 inches of the tube is passed aborally in the lumen of the jejunum.The exiting portion of the tube is laid in the 1- to 1.5-cm seromuscular incision, and the tube is sutured in this “tunnel” by inverting the seromuscular layer over the tube with three or four interrupted Cushing sutures of 4-0 Maxon (Figure 12-32, A-C).The tube exit site of the jejunum is sutured to the exit site at the body wall with four to five simple interrupted sutures of 4-0 Maxon to provide a permanent enteropexy. The exiting feeding tube is secured to abdominal skin using a Chinese finger-trap friction suture of 2-0 Novofil.The clinician should be careful not to occlude the lumen of the tube when placing the finger-trap suture (Figure 12-33, A-C). The feeding tube exit site should be incorporated into a body bandage to prevent premature removal

FIGURE 12-27 Gastrostomy tube placement: surgical placement through a midline laparotomy—cross section of the abdomen showing the gastropexy and position of the gastrostomy feeding tube. (From Crowe DT Jr: Enteral nutrition for critically ill or injured patients— part II, Comp Cont Educ Pract Vet 8:719,1986.)
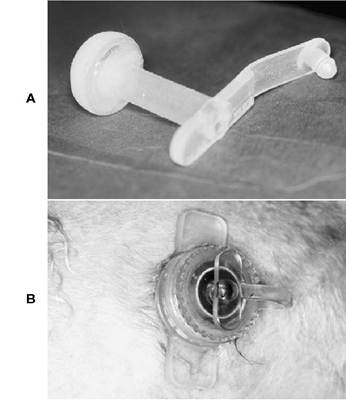
Figure 12-28 A, An example of a low-profile gastrostomy feeding tube. B, Low-profile gastrostomy feeding tube inserted in a male Collie with congenital megaesophagus.
by the patient, technical staff, or owner. Patients with an enterostomy feeding tube can be fed immediately postoperatively. A column of water should be kept in the tube between feedings to
help prevent tube occlusion or reflux of intestinal contents into the tube.
Advantages and Disadvantages. Advantages of enterostomy feeding tubes include bypassing the upper GI tract while providing enteral nutritional support, decreased stimulation of pancreatic enzyme secretion, providing nutrition for entero- cytes, and having fewer metabolic complications than parenteral nutrition has. Disadvantages of enterostomy feeding tube use include necessity of surgical placement, being limited to using liquid diets, necessity for more intensive monitoring because constant-rate infusion of diet is required, and potential for peritonitis with leakage or removal of the tube.
Complications. Complications include premature removal, tube-induced jejunal perforation, peritoneal leakage, and subcutaneous leakage. Tube- induced jejunal perforation is prevented by using soft rubber tubes designed for enterostomy feeding, not high-density polyethylene plastic tubes. Peritoneal leakage is prevented by paying close attention to include a 360-degree enteropexy. Passing 10 to 12 inches of tube into the jejunum and securely fixing the tube to skin with a Chinese finger-trap friction suture prevent subcutaneous leakage.
Gastrostomy-Enterostomy Tube Combination
Occasionally patients may require placement of gastrostomy and enterostomy feeding tubes (Figure 12-34).This combination of tubes is generally indicated for patients that present with vomiting as a major part of the history. These patients cannot initially be fed via a gastrostomy feeding tube immediately postoperatively. Therefore an enterostomy tube is placed and recommended for the initial feeding. A gastrostomy tube is also placed and used if the patient is still anorexic when the vomiting resolves.
Technique. Gastrostomy and enterostomy feeding tubes can be placed individually as described above. Alternatively, the enterostomy tube can be placed through the gastrostomy tube and into the jejunum. This technique is described below. The gastrostomy tube is placed as described above except for the following modifications. The distal end of the gastrostomy tube is cut off. A 5 Fr, 36-inch infant feeding tube (i.e., the tube used for
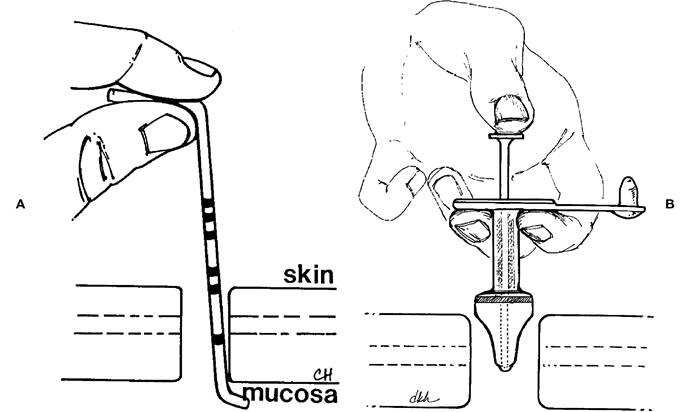
Figure 12-29 Low-profile gastrostomy tube placement. A, A stoma-measuring device placed into a gastrocutaneous fistula and withdrawn until the tip lies gently against the mucosa of the stomach. Circumferential lines indicate three depths (1.5,2.6, and 4.3 cm) that correspond with the shaft length of the feeding tube. B, An obturator being advanced inward until the disk back apposes the base of the low-profile gastrostomy feeding tube. This elongates the mushroom tip, facilitating placement into the stomach. (Modified from Bright RM et al.: Use of a low-profile gastrostomy device for administering nutrients in two dogs,JAm Vet Med Assoc 207[9]:1184,1995.)
enterostomy feeding) is passed through the gastrostomy tube so that it exits from its distal end. Before gastric placement of the gastrostomy tube, the exiting portion of the 5 Fr feeding tube is placed into the stomach lumen through the gastrotomy incision and manipulated into the duodenum and passed into the proximal jejunum. Once the enterostomy tube is placed 10 to 12 inches into the small intestine, the gastrostomy tube is placed into the gastrotomy incision and secured as described above in gastrostomy tube placement via laparotomy. The jejunostomy tube is secured to the gastrostomy tube to prevent tube migration.
Advantages and Disadvantages. The primary advantage of combination tube placement is the ability to feed a vomiting patient immediately postoperatively via an enterostomy feeding tube and to continue feeding the patient into the stomach if the vomiting resolves but the patient remains anorexic. The primary disadvantage of combination gastrostomy-enterostomy tube placement is the difficulty in passing the enterostomy tube in the small intestine. Care and patience is needed to encourage the small 5 Fr feeding tube to pass through the pylorus and into the small intestine.
Complications. The major complication associated with combination gastrostomy-enterostomy tube placement is gastrostomy tube occlusion with diet fed in the enterostomy tube. Occasionally diet placed in the enterostomy tube will occlude the gastrostomy tube. It is important to encourage careful management of the enterostomy tube so that diet does not enter the gastrostomy tube.