Sprains, Subluxations, and Luxations
WiH C. Jordan • Canaan Whitfield-Cargile
■ Definitions Sprains and luxations have been classified as type 2a traumatic arthritides.1 These injuries have been categorized in three forms: mild, moderate, and severe.
Mild sprains constitute injuries that involve the tearing or disruption of a minimal number of ligament fibers with no loss of integrity to the ligament. Hemorrhage and edema are typically present in the ligament. Injuries that involve a portion of the ligament, with loss of integrity, are considered moderate sprains. Laxity of the joint is often present with moderate injury, but complete separation of the ligament from the bone or complete separation of the body of the ligament is not seen. Significant hemorrhage and edema are present in the ligament. Injuries that involve tearing of the ligament, resulting in either complete separation from the bone or widening of the tendon fibers, are considered severe sprains. These injuries result in some form of joint instability, especially when the affected joint is manually stressed.Luxations and subluxations are usually the result of severe sprains of periarticular or articular ligaments. Luxations represent the complete dislocation of the articular surfaces, whereas subluxations have only partial and incomplete disarticulation (Fig. 38.19).
■ Etiology and Pathophysiology Sprains can be associated with acute injuries in which the ligaments are suddenly overloaded, resulting in acute failure or secondary to repetitive strains of submaximal loads resulting in less obvious breakdown but ultimately ligamentous injury. The latter results when maximal or near-maximal loads are repeatedly applied to the ligaments and associated structures, causing a degenerative type of lesion. Age can also be a contributing factor in these degenerative changes. Muscle fatigue can contribute to the weakening of adjacent structures, increasing the stresses applied to the supporting ligaments.
It is suspected that most sprains of ligaments are due to acute overload, whereas tendon injury most likely occurs as a result of repetitive low-grade trauma resulting in molecular degeneration.2 Luxations and subluxations are usually of traumatic origin, such as stepping in a hole or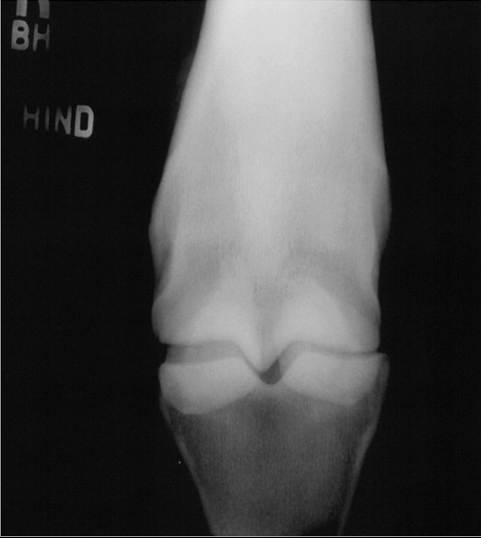
FIG. 38.19 Dorsopalmar radiograph of a subluxated metaphalangeal joint after the joint has been manually stressed.
entrapment of a limb in a gate or fence, or subsequent to traumatic complete ligamentous disruption.1
Typically, hemorrhage and edema form within the ligaments surrounding the joint capsule, or in severe lesions the hemorrhage can be periligamentous or intraarticular. Inflammation ensues, and the ligamentous or capsular lesion heals through fibrosis, forming a scar, with the predominant production of type III collagen. Type III collagen contains smaller-diameter fibrils and has fewer crosslinks than type I collagen, which is the predominant collagen type in normal tendons and ligaments. As the lesion matures, both fibril diameter and number of crosslinks increase, in addition to the proportion of type I collagen. This increases the strength of the injury, which can take weeks to months to heal but will ultimately be weaker than normal tissue.3 Often the affected joint capsule and surrounding ligaments become fibrotic as healing occurs, resulting in decreased range of motion (ROM) in the affected joint. Secondary dystrophic mineralization of the affected soft tissue structures may occur and also adversely affect the joint's mobility.
Luxations of the coxofemoral joint in calves may be associated with calving injuries during dystocia or in cows being ridden while in estrus, or with a traumatic fall in the immediate postpartum period.3 Shoulder joint luxations are usually the result of trauma.4
■ Clinical Signs and Differential Diagnosis Clinical signs vary depending on the severity of the sprain, location of injury, and time since the initial injury.
The animal may have a history of mild lameness or decreased performance, as well as a history of a positive response to NSAIDs or stall rest. Patients with moderate to severe sprains will typically have a more pronounced, acute lameness or may be non-weight bearing on the affected limb. There may also be localized swelling, heat, increased joint effusion, or pain elicited on palpation or manipulation of the affected joint. Other signs may include abnormal limb positioning, decreased ROM, crepitus, and joint laxity. Injuries may present after an acute or traumatic insult as chronic lameness, or a chronic mild injury can present acutely with severe lameness if the collateral ligament completely ruptures. Chronic injuries are characterized by joint capsule thickening or enthesophyte formation at the origin and insertion of the affected collateral ligament.Subluxations and luxations result in loss of joint function, loss of structural integrity of the limb, and potentially an acute varus or valgus deformity. Complete luxations in the horse are most common in the pastern, fetlock, and hock joints.5-8 Luxations can occur in the shoulder,19 carpus, and coxofemoral joint, but these luxations are less common in horses.9,10 Coxofemoral luxations are the second most common type of luxation in cattle.3
Differential diagnoses vary depending on the region affected and duration of injury but may include soft tissue contusion, synovitis and capsulitis, osteoarthritis, bursitis, musculotendinous injuries, fractures, physeal fractures, septic arthritis, tenosynovitis, and flexural or angular limb deformities.
■ Diagnostic Tests A thorough history and physical examination should be performed at presentation. The examination should include assessment of pain, swelling, heat, joint effusion, and joint instability. Patients presenting with only mild lameness should have a thorough lameness examination. Caution should be exercised in regard to perineural anesthesia, especially if there is evidence of joint laxity or instability or severe lameness, as perineural anesthesia could exacerbate the extent of joint damage or result in complete luxation once the affected area is desensitized, resulting in increased weight bearing.
Confirmatory diagnostics include diagnostic imaging to confirm sprain, luxation, or subluxation. The imaging modality of choice will vary greatly depending on species affected, size of animal, location of injury, and physical exam findings. Radiographs should be obtained to assess the joint's bony structures because concurrent fractures are common, with traumatic insults resulting in luxation. Stress views can be performed to assess the level of joint instability (see Fig. 38.19). One study reported on 17 horses with luxation or subluxation of the metacarpophalangeal (MCP) or metatarsophalangeal (MTP) joints.5 All had rupture of at least one collateral ligament (CL) of the joint. In those horses, radiographs showed that 8 of 17 horses sustained fractures, 6 of which were avulsion fractures located at the origin of the CL. Other types of fractures identified in that study were splint bone fractures and small articular chip fractures. Fractures of the proximal or middle pastern bones can cause luxation or subluxation of the proximal or distal interpastern joint. Nuclear scintigraphy can also be used to evaluate insertional desmopathies that may not be radiographically apparent.
Ultrasonography is very useful in localizing and depicting the severity of ligamentous lesions and for confirming the association of fracture fragments identified radiographically. In acute cases, ultrasound evaluation often shows hemorrhage within the joint capsule (Fig. 38.20). Ultrasonography is often a useful imaging modality to assess the integrity of joints that may not be amenable to radiographs such as the coxofemoral joint, where this modality can be an important component of the diagnosis.11 Cross-sectional imaging including CT or MRI is useful in the diagnosis of joint integrity, and MRI is the gold standard for imaging and diagnosing ligamentous injuries in large animals.12,13
■ Treatment Treatment varies widely based on the severity of the injury, location, and associated structures involved.
Mild sprains can be treated conservatively with support bandages, NSAIDs, polysulfated GAGs, and rest for 3 to 4 weeks, followed by a controlled exercise program before returning to normal activity. Adjunctive physiotherapies such as hydrotherapy or shock wave treatment may also be considered. Moderate sprains involving significant ligament damage may necessitate use of a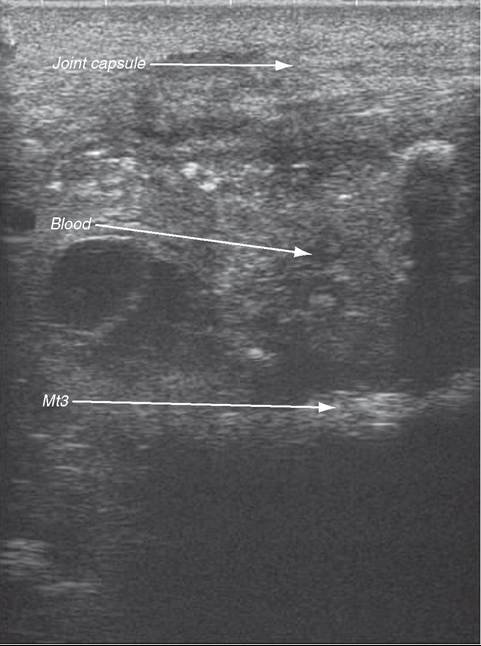
FIG. 38.20 Ultrasound image of a metacarpophalangeal joint from a horse with an acute sprain. Note the hemorrhage accumulation within the joint capsule. Mt3, Third metatarsal bone of fetlock joint.
cast or splint to provide joint stability during the initial healing process. Distal limb immobilization with a fiberglass cast and stall confinement was the initial treatment for 10 of 17 horses with MCP or MTP luxation and CL rupture. Duration of cast immobilization ranged from 14 to 132 days (mean = 71 days).5
In acute cases, hemorrhage is often present within the affected joint. This hemorrhage usually resolves after 7 to 10 days, but it can also subsequently form a fibrinous clot within the joint capsule, resulting in a chronic, mild synovitis that may necessitate treatment with intraarticular antiinflammatory agents, including sodium hyaluronic acid and triamcinolone.14,15 Diagnostic arthroscopic surgery should be considered to evaluate articular cartilage integrity and remove persistent fibrin accumulation. If arthroscopic surgery is performed, a cast or splint should be applied to the affected limb during recovery from anesthesia to prevent luxation of the affected joint and further injury. Severe sprains may require some form of internal coaptation (surgical implants) or arthrodesis of the joint, depending on the degree of joint instability. Support of the contralateral limb should be considered for non-weightbearing injuries.
Luxations of the coxofemoral joint in cattle can be repaired by open or closed techniques, and success depends on duration of the luxation, concurrent fractures or soft tissue injury, and age.
Open reduction was reported as being more successful than closed reduction, although closed reduction should be attempted immediately after the injury if possible.3 In select cases, femoral head otectomy can also be considered.9,16 Shoulder joint luxations can also be reduced by closed and open techniques, with degree of injury, clinician preference, success of closed approach, and damage to other structures dictating which approach is chosen.,■ Prognosis Prognosis depends on the severity of damage to the intraarticular cartilage and surrounding soft tissue structures. Horses that sustain mild joint or ligamentous strains have a good prognosis for returning to previous athletic use. Horses that sustain moderate or severe sprains or joint luxations usually develop secondary DJD in the affected joint, which may require intraarticular medications and NSAIDs or, in some cases, surgical arthrodesis of the affected joint. The prognosis for survival and returning to athleticism varies widely based on many of these factors. The long-term prognosis for returning to athletic performance may be poor. Eight of 17 horses with MCP or MTP joint trauma resulting in joint instability and rupture of the CL returned to riding, and one returned to jumping activity after limb immobilization and stall confinement.5