Therapeutics
Unfortunately, there is no rapidly acting treatment to improve clinical signs, nor is there any treatment that can reverse or even halt this process. However, management of anxiety can make a significant impact on the quality of life of both the patient and the family.
There are multiple options for managing anxiety in dogs. Alprazolam is my first choice as it is very safe and does not interfere with most concurrent diseases. It can be administered at 0.01-0.1 mg/kg once to twice daily or as needed an hour before bed to aid in sleep. It is a benzodiazepine, so there is the potential for a paradoxical reaction. Trazodone can also be used as an anxiolytic at 2-5 mg/kg two to three times daily. Trazodone and tramadol can be administered together with care - dose adjustments must be made as higher doses of both in combination can induce serotonin syndrome. Oral aceproma- zine is another option, but oral absorption is erratic and unreliable in the dog, so you must carefully titrate the dose to effect; overdoses of acepromazine can also cause significant hypotension. I never recommend using phenobarbital for sedation as it can have significant side effects including hepatopathies and blood dyscrasias.Chronic therapeutic options include pharmaceuticals and neutraceuticals. Selegiline (Anipryl), is a monoamine oxidase B inhibitor that should be administered at 0.5-1 mg/ kg once daily in the morning. Selegiline should not be combined with tricyclic antidepressants or selective serotonin reuptake inhibitors, and should be used cautiously with other drugs that can enhance serotonin function (like tramadol and trazodone) due to the potential for serotonin syndrome. S- adenosylmethionine (SAMe) has also been shown to reduce age-related mental decline in dogs; it should be administered at 18mg/ kg for at least 2 months. L-Carnitine and omega-3 fatty acids have also been used in dogs with CCD.
There is also some evidence for vitamins E and C and antioxidants in the diet. None of these therapies can halt the progression of disease nor can they make clinical signs go away completely. These treatments also are slow to act. They all need to be administered for at least one month, ideally two, before any clinical effect is seen.There is no one therapy that has significant benefits over another, though multiple therapies can be initiated at once.
Rescue or relapse therapies for CCD mainly focus on preventing or treating anxiety. This can be done preemptively, when a known stressful scenario is coming and the owners can pre-treat. A good example of this would be houseguests visiting and disrupting the normal schedule of the household. This kind of aberration often induces marked anxiety in CCD patients, so a short-acting anxiolytic drug like alprazolam or trazodone can be used to effect. The same drugs can be used if there is an unforeseen event that causes a crisis. In this scenario, a benzodiazepine is more
Table 6.2 Canine cognitive dysfunction rating scale with example data for a dog over the threshold (P50) for query diagnosis.
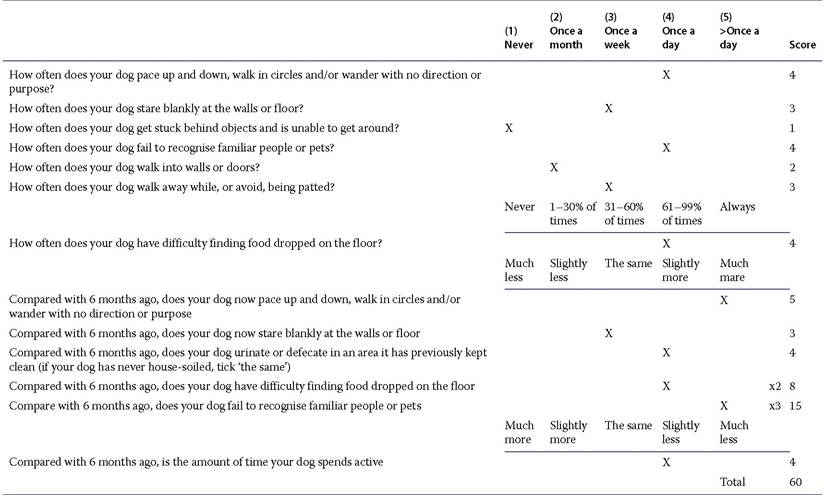
Source: Salvin et al. 2011, p. 334. Reproduced with permission of Elsevier.
effective as it is more rapid-acting. Unfortunately, there is no true rescue therapy as there is nothing that has been shown to reverse the disease process.
All of the above-listed drug therapies have been shown to have some effect, but they do not all work in every case! Generally, any one therapy will work in about 50% of dogs, but they will take at least a month to show any effect. If no intervention is performed, the condition will simply progress in its natural course.
Any of the therapies listed will have a greater effect if started earlier in the clinical disease process. The later in the disease, and the more severely affected the animal, the less likely you are to get a great clinical effect from any medication.
As a clinician, it is important to have objective measurements for the patient. Here, you can use serial neurological examinations and behavioral assessments to monitor progression of the disease. The CADES or CCDR scales are also very useful as monitoring tools as they will give you a number and not just an opinion. Because quality of life means different things to different people, the objectivity of validated scales can be very helpful. Pain is not typically a component of CCD, but geriatric dogs often suffer from degenerative joint disease or chronic spinal cord disease and may show discomfort as a result of that; if there is any question of pain, it should be treated. The inappropriate vocalizations often exhibited by patients affected with CCD may represent disorientation, anxiety, or pain. These patients exhibit progressive loss of mental function and will eventually end up totally unaware of their surroundings. This progression can occur over months to years, depending on how early signs are noted. As the disease progresses, there will be loss of function manifested in deterioration
Box 6.2
A pet's chronic progressive loss of function and ability to perform normal activities can be devastating to clients.
of mental abilities, less and less recognition of the owner and familiars, loss of house training, and decreased interaction.
A caregiver's expectations, ability, and quality of life are also considerations with regards to the care of a pet with CCD. Client ability to provide care or accept patient's status must be taken into account. Considerations such as medication regime, emotional, financial, and physical ability of a client to care for the patient should be discussed. To make the unknown less intimidating, it is important to inform the owners that this is a progressive and incurable condition. Whatever treatments are chosen are meant to be palliative and will only help slow the progression; they will not cure the disease. In some circumstances, hospice care (see chapter 36) could be helpful to the client.