Therapy
The choice of treatment depends on the underlying cause of HAC. Therefore, it is important to differentiate between PDH and ADH, after excluding the iatrogenic form.
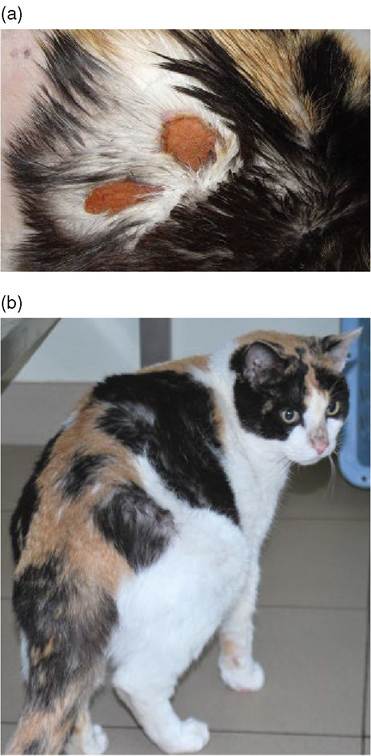
Figure 12.1 Cat (11 years old, spayed female, domestic shorthair) with pituitary-dependent hyperadrenocorticism.
Skin tears are observed on the dorsal aspect of the thorax due to increased cutaneous fragility (Figure 12.1a). Trilostane treatment allowed healing of lesions (Figure 12.1b). At diagnosis the cat was not diabetic. Diabetes mellitus developed after approximately 1 year of trilostane administration, despite improvement of hyperadrenocorticism.Medical and surgical options are available to treat both PDH and ADH. Treatment of HAC quickly improves polyuria and polydipsia, as well as polyphagia, whereas a few months may be necessary for improvement of dermatologic and muscular signs. Reduction of cortisol, however, can unveil clinical signs related to arthropathy or an allergic disorder. Regarding biochemical parameters, these can take weeks to improve and resolve; persistence of alterations may indicate that the treatment is not sufficient or that there is concurrent disease.
Medical Therapy for Pituitary Dependent Hyperadrenocorticism
Trilostane
This is an inhibitor of β-3 hydoxysteroid dehydrogenase in adrenal glands and is currently the drug most frequently used and recommended in dogs and cats due to the high rate of improvement of clinical signs and few side effects. In dogs, the dosages administered orally are 0.2-1.1 mg/kg, twice daily, with larger breeds requiring lesser quantity; some dogs require daily administration (with higher dosages) (Feldman and Kass 2012; Arenas, Melian, and Perez-Alenza 2013). In the cat, dosages vary from 1 mg/kg 3 times a day, up to 13 mg/kg once daily (Mellett, Bruyette, and Stanley 2013).
It is worth noting that trilos- tane is absorbed better when given with food (Figure 12.2).The correct dosage of trilostane is initially checked after 10-15 days and the goal, in dogs, is to reach a cortisol post-ACTH stimulation ranging between 1.5 and 5μg∕dL. Recent studies have reassessed the utility of basal cortisol only: values ≥1.3 μg∕dL exclude excessive suppression, while values < 2.9 μg∕ dL exclude inadequate control. Because clinical benefits can be observed only after about 30 days, at first control the dosage should not be increased, but rather reduced if cortisol is low. Later, modifications of the dosages in dogs are based both on clinical response and cortisol concentrations post-ACTH stimulation:
• If 1year and 29% >3 years (Clemente et al. 2007). The number of cats treated is still too limited to provide accurate information on maintenance therapy and survival.
Mitotane
Mitotane (o, p'-DDD) has cytotoxic action primarily on the area fasciculata and reticularis of the adrenal cortex. For years it was the main drug used for HAC treatment in dogs, while in cats it is not recommended due to its low efficacy. Mitotane in dogs provides good improvement of clinical signs, but can cause serious side effects (hypoadrenocorticism in 6-10%, often irreversible) and relapses are common (50-60% in the first year) (Kintzer and Peterson 1991).
Therapy with mitotane includes two phases:
Initiation phase: 30-50 mg/kg of oral mito- tane, preferably divided in two daily administrations, with food. Dogs undergoing treatment should have a good appetite. The initiation phase is interrupted if the owner observes a major decrease in appetite, thirst, vomiting, or diarrhea. After 8-10 days, or at any time before if a dog shows these clinical signs, the ACTH stimulation test should be repeated. Cortisol post-ACTH should be 1-4 μg∕dL to start maintenance therapy; if >4 μg∕dL, a second course of therapy can be repeated.
In case of severe clinical signs of hypoadrenocorticism or if cortisol decreases to 4μg∕dL, it is recommended to restart the loading phase. Median survival of dogs treated with mitotane is approximately 2 years; according to one study, treatment with trilostane is associated with longer survival than mitotane (Clemente et al. 2007).Ketoconazole
This is an inhibitor of the 11 β-hydroxylase in the adrenal glands but is not frequently used in dogs. The initial dosage is 5 mg/kg twice daily, which may be gradually increased to 20-30 mg/kg, according to clinical signs. The efficacy of treatment is assessed using the ACTH stimulation test. On occasion, the treatment is not effective or may cause liver damage. Median survival of treated dogs is 25 months (Lien & Huang 2008). Ketoconazole is not recommended in cats to treat HAC.
Other Drugs
Bromocriptine, cyproheptadine, selegiline, retinoic acid, metyrapone, and aminoglutethimide are not currently recommended in dogs and cats.
Surgical Therapy for Pituitary Dependent Hyperadrenocorticism
Transsphenoidal hypophysectomy is a good therapeutic option in dogs, especially for tumors of limited size. The most frequent postoperative complications are central diabetes insipidus and hypernatremia, especially if the tumor is large, as well as secondary hypothyroidism and keratoconjunctivitis sicca. Dogs undergoing surgery may experience recurrence in 28% of cases, with a median disease-free period of 896 days (Hanson et al. 2005). The number of cats treated by transsphenoidal hypophysec- tomy is still limited.
Radiation Therapy for Pituitary Dependent Hyperadrenocorticism
This may be considered for pituitary tumors that cause neurological signs. In dogs, radiation therapy can significantly reduce tumor size. However, despite the benefit, in the case of tumors of considerable size neurological signs may persist. Medical treatment of HAC is not discontinued, despite radiation therapy.
The number of cats treated with radiation therapy is still limited.Surgical Therapy for Adrenal Dependent Hyperadrenocorticism
Adrenalectomy is the treatment of choice for dogs with ADH, after careful assessment of risks and benefits. Vascular infiltration, the presence of tumors >5cm and metastases are adverse prognostic factors. Metastases are observed in 6-18% of cases by radiography, ultrasound, or CT. Intraoperative and perioperative mortality is variable, but can exceed 25%; animals that survive, however, have excellent life expectancy, from 1 to over 4 years. To stabilize the dog before surgery, it is important to administer medical therapy (preferably trilostane) for 3-4weeks. Intraoperative and postoperative complications are intraperitoneal bleeding, hypoadrenocorticism, pancreatitis, and acute renal failure (Massari et al. 2011). In cats, experience is still limited.
Medical Therapy for Adrenal Dependent Hyperadrenocorticism
Trilostane is also effective to treat dogs with ADH, although sometimes with a slightly lower dosage than that used for PDH. Median life expectancy ranges from 12-14 months. Mitotane can be used for medical therapy of dogs with ADH, although the effective dosages are 50-100% higher compared to those used for PDH, for both the initiation phase and maintenance therapy. Median survival of dogs with ADH treated with trilostane or mitotane is comparable (Helm et al. 2011).
Other Therapies
Because HAC can lead to hypertension, it is necessary to assess whether this is present and treat it with anti-hypertensive drugs. Furthermore, HAC in dogs often causes glomerulopathy and proteinuria, which may require anti-proteinuric treatment. Dogs, and especially cats, can have concurrent diabetes mellitus. Treatment for HAC improves glycemic control in many cats, but not always in the dog. Finally, since HAC in dogs may promote a hypercoagulable state and thromboembolism, antiplatelet agents may be necessary (Park et al. 2013).