Treatment
Treatment of CP is largely symptomatic as in most cases there is no specific treatment, with the possible exception of the ECS. However, supportive treatment remains very important because it can make a real difference to the quality of life of the affected dog and can be life-saving in acute exacerbations of underlying chronic disease.
The most challenging aspect of long-term management is dealing with the chronic pain, but addressing functional loss is also important. In addition, acute exacerbations of disease should be addressed with intensive management in the same way as truly acute pancreatitis cases.Treatment of Ongoing Chronic Pancreatitis
CP in dogs and cats is usually a low grade, progressive, on-going disease that slowly destroys the pancreatic parenchyma, like a smoldering fire. It is important that the pain, progressive loss of endocrine and exocrine function, and concurrent signs are managed.
In some cases of CP, the disease will eventually ‘burn itself out' when the entire pancreas has been destroyed. These cases will have functional loss (diabetes mellitus and EPI) but will no longer suffer from bouts of pain and acute exacerbations of disease. This is in many ways the “ideal” because the exocrine and endocrine insufficiencies can be treated whereas the pain of on-going CP can be very difficult to control. It is impossible to predict in animals, as in humans, which cases of end-stage CP will “burn themselves out” in the animal's life time and which cases will continue to suffer from recurrent bouts of acute flare-ups of disease in spite of functional loss.
Pain can be particularly marked postpran- dially is often under-recognized by owners and clinicians, particularly in cats. Because of this, all animals with CP should be assumed to be suffering from pain until proven otherwise. Use of effective analgesics often results in behavior changes such as increased activity and playfulness.
In most cases, the pain can be controlled long term but in a small number of dogs and cats, it may prove impossible to provide effective long-term analgesia and this may lead to end-of-life decisions based on quality of life.The pain of CP is similar to other chronic pain conditions in that it appears to cause up-regulation of central pain pathways with resultant hyperesthesia. There are many studies on the mechanisms and treatment of chronic pain in human CP but very little information in dogs and cats. The author has observed lymphocytic infiltrates within nerve sheathes on histology of the pancreas of affected dogs strongly suggesting that neurogenic pain is also important in small animals with CP. Treatment recommendations are thus currently extrapolated from humans. The use of a ‘Pain Ladder' is the most helpful, starting with non-steroidals and then adding additional drugs until pain is effectively controlled (Figure 14.1). Traditional non-steroidals are often avoided because of the risk of GI ulceration and the frequency with which animals with CP have concurrent renal compromise, particularly during acute exacerbations of disease. Consideration could be give to their use longer term when the animal is stabilized, with careful monitoring of renal
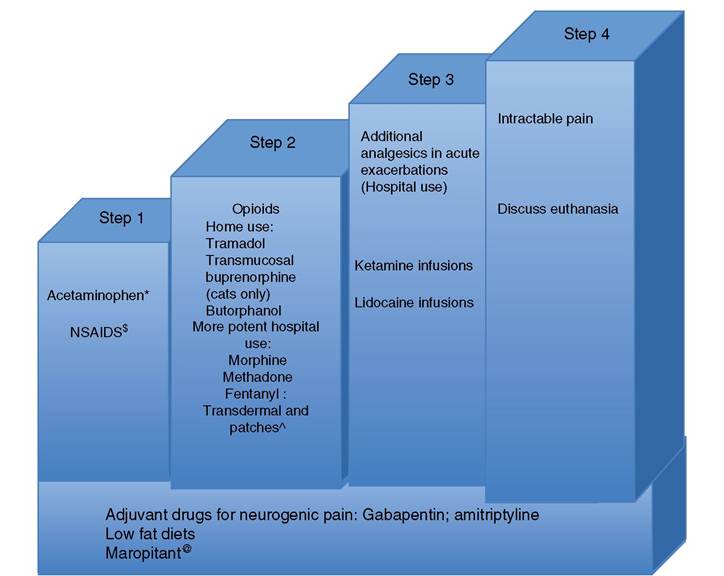
Figure 14.1 Analgesic ladder for dogs and cats with chronic pancreatitis, based on the human analgesic ladder in Sebastiano et al. (2005), which is based on the World Health Organization analgesic ladder for cancer pain. Note each step in the ladder can be added to the previous step for multimodal analgesia. *Preferred non-opioid drug in dogs, provided liver function is normal. Not to be used in cats. sNon-steroidal anti-inflammatories - higher risk of GI side effects in pancreatitis and only to be used when renal function is normal. ^Animals can be sent home with Fentanyl patches but great care must be taken about human contact particularly with children.
@ Substance P has been implicated in the neuropathic pain of chronic pancreatitis so maropitant has a role in multimodal analgesia.function. Acetaminophen is a useful first line drug in dogs, as in humans, but should never be used in dogs with decreased liver function or in cats. Feeding a low-fat diet is likely also to contribute to effective analgesia in dogs and cats with CP. In humans, high-fat diets increase postprandial pain and anecdotally the same is true in small animals.
The loss of exocrine function, together with recurrent bouts of anorexia, means that many affected dogs and cats can suffer from mild or more severe protein-calorie malnutrition, which should be recognized and addressed. Clinicians should be proactive in supplementing pancreatic enzymes in these cases. In addition, it may be necessary to supplement cobalamin in dogs and particularly cats with EPI. This is traditionally given parenterally, but a recent study suggests oral supplementation may also be efficacious.
Comorbidities are common in canine and feline CP. Affected animals are often elderly, so some may be etiologically unrelated additional diseases of ageing dogs and cats, which may impact on control of the CP. For example, hyperadrenocorticism in dogs appears to increase the risk of acute bouts of pancreatitis. In cats, cholangitis and inflammatory bowel disease are common co-morbidities and their etiological relationship to CP is unclear. Clinicians should treat all co-morbidities as effectively as possible, while considering the potential for any treatments or dietary interventions to worsen the pancreatitis.
CP in ECS may respond to immunosuppression with corticosteroids or systemic cyclosporine. Ideally, diagnosis should be confirmed histologically in either pancreas or kidney prior to medication, but their use could be considered in an animal with convincing diagnostic imaging and clinic- pathological changes. Monitoring efficacy of treatment is currently challenging, as there are no validated blood tests for serial measurement, so animals should be monitored by clinical response.
Corticosteroids may also be indicated in cats with CP, predominantly to treat concurrent inflammatory bowel disease and/or lymphocytic cholangitis. The underlying cause of these diseases in cats remains an area of active research and bacteria have also been implicated, so the concurrent use of antibiotics is logical in cats until the diseases are better understood. A more complete discussion of the potential etiologies of CP and cholangitis in cats can be found in Simpson (2015)
Treatment of Low-Grade Recurrent Flare-ups
Dogs and cats with CP commonly present with stable ongoing chronic disease punctuated by episodes of acute exacerbation (like a smoldering fire which recurrently flares up). Severe acute episodes will require hospitalization and treatment. The owner at home can manage milder episodes, as long as the animal is not dehydrated or anorexic for a prolonged period of time. Mild acute episodes should be managed with an increase in analgesic use and a day or two of fasting. Early enteral feeding is very important in the context of severe acute pancreatitis but in mild disease, a few days fasting is not injurious and will reduce the pain associated with the episode. The author has also observed that some dogs respond to a course of metronidazole (10mg∕kg BID) after an acute bout of disease, particularly CKCS. This is likely to be due to development of secondary antibiotic responsive diarrhea due to secondary small intestinal ileus and malabsorption.
Treatment of Acute Flare-ups
Acute exacerbations of disease may also be very severe. Cases presenting clinically as severe acute pancreatitis should be treated in the same way as truly acute pancreatitis with intensive supportive care. The pillars of treatment of acute pancreatitis, and acute flare-ups of chronic disease, are: fluid therapy, analgesia, anti-emetics, and early enteral feeding.
More on the topic Treatment:
- Fluid Therapy for Renal Failure in Horses (Box 44.4)
- Eosinophilic enteritis (EE)
- Physitis (Epiphysitis)
- Control
- Acquired Torticollis
- Triaryl Phosphate Poisoning (Chronic Organophosphate Poisoning; Dying-Back Axonopathy)
- TUBERCULOUS MYCOBACTERIOSIS IN TERRESTRIAL AUSTRALIAN MAMMALS
- Compartment, Downer, and Muscle Crush Syndromes of Cattle
- Abstract
- The Superfamily Macropodoidea includes kangaroos, wallabies, potoroos, bettongs and the musky rat-kangaroo (Hypsiprymnodon moschatus), collectively referred to here as ‘macropods’.