Treatment of Undifferentiated Ruminant Respiratory Disease
Amelia R. Woolums
ANTIMICROBIAL THERAPY. The basic principles of antimicrobial therapy for bacterial bronchopneumonia are to treat early enough, treat long enough, and treat with the appropriate antimicrobial agent.
Because there are currently many effective antimicrobials marketed for the treatment of important bacterial respiratory pathogens in cattle (see Table 31.15), failure to treat early enough is more likely an important cause of treatment failure than failure to choose the correct antibiotic. If lung lesions becomes too advanced before treatment is initiated, it may not be possible to reverse lung pathology with a practicable course of any antimicrobial.Treating early enough requires timely identification of animals with clinical signs of respiratory disease. Because individual ruminants in production agriculture settings often receive their first treatment for undifferentiated respiratory disease from a layperson caretaker and not from a veterinarian, it is appropriate for caretakers to be taught by the supervising veterinarian to recognize signs of respiratory disease. Caretakers should be trained to watch for these signs whenever they are in contact with ruminants in their care; clinical scoring systems have been developed for identification of respiratory disease in dairy calves.2,3 Similarly, in cattle feedlots clinical signs are assessed by lay caretakers, including the pen riders who evaluate cattle in the feedlot pens and the “hospital crew” who examine individual cattle “pulled” or removed from feedlot pens by the pen riders and sent to a treatment area for individual assessment and treatment by the hospital crew. It is imperative that lay caretakers evaluating animals for clinical signs of disease receive training from the supervising veterinarian and that training be reviewed regularly so disease identification and treatment is as accurate and timely as possible.
In addition, treatment of affected animals by lay caretakers should be based on written protocols established by the supervising veterinarian and maintained for easy review on the farm or feedlot.Ruminants with undifferentiated bronchopneumonia are often identified and treated presumptively based on clinical signs, without diagnostic testing to identify specific viral or bacterial etiologic agents. However, if animals fail to respond as expected to nonspecific therapy, diagnotic tests are warranted, as they may reveal an unexpected pathogen, a bacterial pathogen with unexpected antimicrobial resistance pattern, or another underlying disease that must be addressed.
Since bacteria often contribute to bronchopneumonia in ruminants, appropriate presumptive treatment includes an antimicrobial effective against the most common causes of bacterial bronchopneumonia. Selection of the appropriate antimicrobial tends to be what most veterinarians focus on when treating respiratory disease because this is the aspect of therapy over which they have the greatest control. Factors such as cost, route of administration, treatment interval, drug label restrictions, necessity of extralabel doses, and withholding times may exclude a number of antimicrobials, leaving a short list of suitable alternatives for use as a first-line antimicrobial agent. Only antimicrobials that are licensed and effective at label doses should be considered for routine use in food animals. Table 31.15 lists antimicrobials currently approved in the United States for the treatment of respiratory disease in cattle, sheep, and goats. If data regarding the MIC of bacteria isolated from untreated animals are available, the dose or duration of therapy can be rationally modified, but it is imperative that proper withdrawal times be observed when antimicrobials are used in an extralabel fashion. At the time of this writing, the Food Animal Residue Avoidance Databank (FARAD; www.farad.org or 1-888-USFARAD) is an invaluable resource for veterinarians who need to identify withdrawal times for drugs administered to food animals in an extralabel manner.
The use of MIC data requires some understanding of the pharmacokinetics and pharmacodynamics of the drugs to be considered; published information is available regarding interpretation of MIC data, or veterinarians can contact FARAD, the diagnostic bacteriologist at their local diagnostic laboratory, or a veterinary clinical pharmacologist for assistance.A decision regarding which antimicrobial to use to treat bronchopneumonia may be based on the results of antimicrobial susceptibility testing or MIC data for bacteria isolated antemortem or postmortem from animals in the group. However, such results must be interpreted carefully. The most relevant information is gained from testing samples collected from diseased lung at postmortem from animals that have not yet received any antimicrobial therapy. However, because animals are often treated presumptively before they die or are euthanized, it may be difficult to test animals that have not already been treated. Once an animal has been treated, bacteria isolated may be resistant to multiple antimicrobials.19,20 However, bacteria isolated from the lungs of cattle that have been treated with antimicrobials are not always resistant to these drugs.21 Currently, evidence-based guidelines for management of cattle with bronchopneumonia attributed to MDR bacteria are lacking; anecdotally it has been reported that cattle can recover despite the presence of M. haemolytica resistant to the antimicrobial with which they are treated. This may indicate that the host response can resolve infection and repair pathology in at least some cases of MDR infection. Management of cattle with respiratory disease associated with MDR bacteria is an active area of research.
The choice of which antimicrobial to use can also be based on records of efficacy for animals treated in the past. Producers who keep accurate records of drugs used, with results of treatment responses, relapses, and the proportion of treated animals that become chronic cases, may select first-line antimicrobials based on historical performance of a drug.
This may be the best approach to antimicrobial selection. Guidelines for response to antimicrobial therapy for feedlot cattle with respiratory disease have been suggested: 70% to 80% of animals should respond to the first treatment they are given, the case fatality rate should be between 4% and 7%, and the ratio of chronic cases to cases that die should be 0.5 to 1.0.22A final method of choosing a first-line antimicrobial drug is reliance on published treatment trials. Published trials give comparisons between responses for various antibiotics in cattle with naturally occurring bacterial bronchopneumonia. The outcomes of these trials are often expressed as both health and production values. When evaluating published treatment trials that use cases of naturally occurring bacterial bronchopneumonia, it is important to realize that the results may not be applicable to cattle and pathogens outside the operation where the trial was carried out. The highest-quality information comes from meta-analyses or systematic reviews, which incorporate information from multiple trials. Recent meta-analyses provide estimates of the relative efficacy of many of the antimicrobials currently labeled for treatment or control of bovine respiratory disease.23-25
Mass medication of an entire group of cattle during an outbreak can curtail the daily number of new cases and improve outcomes. In the acute stages of an outbreak, whatever drug is chosen should be given by injection; therapeutic levels are not likely to be reliably maintained by administering drugs in feed or water because of suppressed feed intake by sick cattle. It is important to base a decision to mass-medicate on measurable criteria. Some feedlot veterinarians implement mass medication when the pull rate of sick animals is 10% on each of 3 consecutive days or 25% on a single day.26
Although little research has been undertaken to determine optimal duration of therapy for undifferentiated respiratory diease of ruminants, a general recommendation is that therapy should be continued for at least 48 hours after clinical signs of fever, dyspnea, and systemic inflammatory response have abated.
Many of the antimicrobial drugs labeled for use in the treatment of pneumonia in cattle provide multiple days of therapeutic drug concentrations in lung tissue after only a single injection. These products decrease the time and stress associated with daily treatment; in feedlots, they also make it easier for caretakers to return animals to home pens rather than keeping them in hospital pens, which may be associated with poorer responses by treated animals. Although a 3-day course of antimicrobial therapy for undifferentiated bronchopneumonia was in the past considered adequate, the view is increasingly held that treatment for a longer duration may be more appropriate. This is particularly true for pneumonia caused by M. bovis in dairy calves or feedlot cattle, which may respond better to treatment for at least 7 to 10 days.27,28 Although treatment for 7 to 10 days would be extralabel for some antibiotics, multiple drugs currently marketed have been shown to provide therapeutic drug levels for at least 7 days when used at dosages recommended on the label (see Table 31.15).In some cases clinical signs of bronchopneumonia do not resolve following treatment with the first-line antimicrobial. In such cases, veterinarians must decide when to give a new drug and which drug to choose for second-line therapy. In the past, a standard recommendation was to administer a second antimicrobial if the animal was still febrile 72 hours after treatment with the first-line antimicrobial. However, recent research has suggested that, for cattle given a long-acting antibiotic as a first-line treatment, it may be acceptable to wait longer than 72 hours before administering a second antibiotic. For example, it has been recommended that cattle not responding to treatment with long-acting (200 mg/mL) oxytetracycline should be treated with a second drug after 2 to 3 days, whereas cattle treated with ceftiofur crystalline free acid (Excede® [Pfizer Animal Health, Parsippany, N.J.]) should be treated with a second drug if not responding after 5 to 7 days, and cattle treated with tulathromycin (Draxxin® [Pfizer Animal Health, Parsippany, N.J.]) should be treated with a second drug if not responding after 7 to 14 days.29 It can be difficult for a veterinarian to withhold treatment with a second or even third drug if cattle are not improving quickly, but administering a different long-acting product every 3 days may not improve outcomes, although the practice will increase the cost of treatment and may also increase opportunities for the development of bacteria resistant to the antimicrobials.
More research is needed to provide evidence-based guidelines regarding when a second or third drug should be given to nonresponding cattle. At this time, veterinarians often make recommendations based on past experience. A typical decision tree for treating feedlot cattle with antibiotics is shown in Fig. 31.67, but protocols such as these may be modified as more information about the use of long-acting antimicrobials is obtained from field research.The same principles of therapy described previously apply to the treatment of sheep and goats. Unfortunately, fewer drugs are labeled for the treatment of sheep and goats as compared with products used for cattle. Drugs labeled for use in sheep and goats are listed in Table 31.15. Note that whereas tilmicosin (Micotil 300 [Elanco Animal Health, Greenfield, Ind.]) is labeled for use in sheep, fatal reactions have occurred in goats treated with this drug. Goats should not be treated with tilmicosin. It is imperative to ensure that producers are given an appropriate meat and milk withdrawal time when antimicrobials are administered to sheep and goats at extralabel dosages; this is a particular concern in feedlot lambs or goats and in lactating dairy sheep or goats, from which products may enter the food chain in a relatively short time after treatment.
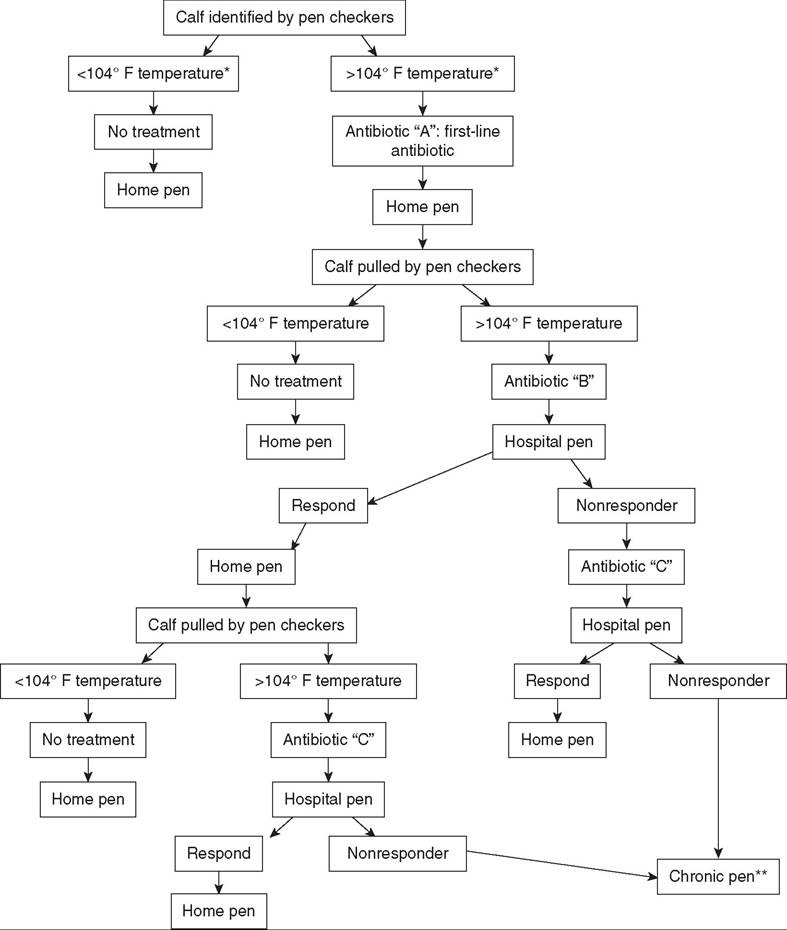
‘Temperature at which cattle are treated can vary from 103.5° to 104.5°F ; cutoff is selected at discretion of supervising veterinarian. **Calves in chronic pen should be monitored for weight gain, suffering, and withholding times, so that appropriate action can be taken (i.e., euthanize, sell, continue feeding).
FIG. 31.67 Decision tree for antibiotic treatment of feedlot cattle. (Input contributed by Dr. Robert A. Smith.)
ANTIINFLAMMATORY THERAPY. Viral or bacterial infection that leads to bronchopneumonia can cause significant tissue injury and inflammation. Moreover, many of the bacteria that cause bronchopneumonia are gram-negative bacteria that produce endotoxin, which can cause a systemic inflammatory response that can be harmful and even fatal. Treatment with NSAIDs could mitigate these effects; treatment should also decrease fever and discomfort, which should lead to improved feed intake and improved growth or milk production. A review of the published evidence for the use of NSAIDs in treatment of BRD is available.30 Although NSAIDs often decrease fever and improve clinical appearance in cattle with BRD in the first few days after administration, a positive impact of NSAID treatment on other outcomes has not been as consistent. For example, average daily gain was improved for cattle with BRD given an NSAID as well as an antimicrobial in one study31 but not in another.32 Mortality was not decreased by NSAID treatment,32,33 but lung consolidation at slaughter or necropsy was decreased in cattle receiving certain NSAIDs.31,33 Therapy with NSAIDs might be justified on the grounds that they should improve animal comfort and therefore animal welfare, but the degree to which they actually improve comfort and welfare has not been quantified. It has also not been well established that NSAIDs are cost-effective; this will likely vary in different settings depending on the number of animals to be treated and the cost of the drug administered. If NSAIDs are to be used for treatment of BRD, in the United States and Canada flunixin meglumine (Banamine® [Merck Animal Health, Madison, N.J.]) is approved for control of pyrexia associated with BRD (1.1 to 2.2 mg/kg IV either as a single dose or divided into two doses at 12-hour intervals for up to 3 days). It is important to remember that flunixin meglumine is labeled only for IV use; administration via the IM or SC route can result in violative residues in tissues if longer withdrawal times are not observed. Phenylbutazone, which has been used in the past for antiinflammatory effect in ruminants, is now illegal to use in lactating dairy cattle in the United States, and because of prolonged tissue levels found in treated cattle its use is discouraged in all food animals. Recently meloxicam has received significant attention in North America for the control of pain and inflammation in cattle (1 mg/kg PO34 or 0.5 mg/kg IM35). At the time of this writing, meloxicam is not specifically approved for the treatment of BRD in the United States or Canada; it is approved in Canada for treatment of calves with diarrhea or for pain control associated with disbudding. At the time of this writing, no NSAID is labeled in the United States or Canada for the treatment of respiratory disease in sheep or goats.
Because NSAIDs can be nephrotoxic and because nephrotoxicity is exacerbated by dehydration, dehydrated animals should be rehydrated before administration of these drugs. Care should also be taken not to overdose NSAIDs or use them for prolonged periods because they may also result in abomasal ulceration.
While corticosteroids have potent antiinflammatory effect and are sometimes used for treatment of severe inflammation associated with an infectious disease, they should not be used indiscriminately in the treatment of respiratory disease because of the potential for immunosuppression. Corticosteroids may have a place in treatment of respiratory diseases such as necrotic laryngitis or tracheal edema syndrome of feedlot cattle because edema of the larynx or trachea can cause life-threatening airway narrowing. The dose for dexamethasone in cattle is 0.05 to 0.2 mg/kg IM or IV, and the dose for isoflupredone acetate is 10 to 20 mg IM. Treatment with corticosteroids may cause recrudescence of BHV-1 infections.
There has been little research to support the use of antihistamines as an ancillary treatment for bovine respiratory disease. Tripelennamine HCl is labeled for cattle at a dose of 1.1 mg/kg, which can be repeated in 6 to 12 hours.
ANTIVIRAL AND IMMUNOMODULATING THERAPY. Although antiviral drugs could be of theoretical benefit for treating ruminants with undifferentiated bronchopneumonia, they are not routinely used. Levamisole and isoprinosine have been used in attempts to stimulate the bovine immune system with equivocal success.36 It is important to recognize that the immunostimulatory benefits of levamisole occur at doses in the 2 to 3 mg/kg range, compared with the anthelmintic dose of 6 mg/kg. A decreased immune response has been observed after an 8 mg/kg dose of levamisole. A DNA immunostimulant (Zelnate [Bayer Healthcare LLC, Pittsburgh, Pa.]) is available for use to aid in the treatment of BRD associated with M. haemolytica infection. Treatment with this immunostimulant decreased the percent of abnormal lung in calves experimentally exposed to M. haemolytica3 and decreased mortality due to BRD in high-risk cattle.38
SUPPORTIVE THERAPY. Supportive treatment may foster recovery of patients with respiratory disease. Sick animals should be provided with shelter that protects them from rain, cold, wind, and hot sun. They should not be crowded or housed in areas with excess mud and manure, and good-quality feed and clean water should be easily accessible. Mineral and vitamin deficiencies should be corrected with the use of injections or oral preparations if necessary.