Tubular Necrosis
Meredyth L. Jones
Tubular necrosis (TN) is a term referring to intrinsic acute renal failure (ARF) caused by hemodynamic, nephrotoxic, glomerular, or interstitial disorders. Tubular damage may be a primary clinical entity or a secondary effect of another systemic illness.
The kidneys receive a large proportion of circulating blood volume, resulting in a high rate of toxin exposure, as well as increased vulnerability to ischemia and reperfusion injury with diseases causing changes in nutrient blood flow. Acute renal failure, characterized by a sudden decrease in glomerular filtration rate, nitrogenous waste accumulation, and loss of the ability to manage sodium, electrolytes, protein, acid-base and water balance, develops over hours to days. Depending on the nature and duration of the primary insult, widespread dysfunction or necrosis of tubular epithelial cells may produce reversible renal injury, ARF, or chronic renal failure (CRF).Potential causes of TN and ARF are included in Table 34.2.
Clinical Signs
The clinical signs of ARF in ruminants are nonspecific and usually not indicative of overt urinary tract dysfunction. Depending on the inciting cause, anuria, oliguria, or polyuria may exist. Cattle with ARF frequently are presented for evaluation of poor appetite, diarrhea, or epistaxis.1 Depression, nasal discharge, ileus, melena, and mild free-gas bloat may also be present. If a concurrent septic condition exists, fever, tachycardia, and scleral injection may be present. The saliva may have a strong ammonia smell. Muscular weakness, even recumbency, may result from the acid-base and electrolyte imbalances and intravascular volume depletion that occur with severe, acute TN. Rectal palpation findings are usually unremarkable, although renal enlargement and perirenal edema may be found in occasional cases. If untreated, CRF may ensue, usually producing weight loss in addition to the signs listed.
In such cases, a reduction in size of the left kidney may be appreciated on rectal palpation.Renal (uremic) encephalopathy is a syndrome of brain dysfunction associated with renal disease. It is characterized by signs of intracranial disease, such as altered behavior or sensorium, weakness, motor dysfunction, and convulsions, which may resolve on restoration of normal renal function or improvement of clinical parameters of renal disease. The pathogenesis of renal encephalopathy is complex and incompletely understood, but neurologic function appears to be impaired by alterations in the extracellular fluid content of acids, phosphorus, amino acids, or certain hormones. Alteration in neurotransmitter balance or release within the central nervous system (CNS) may also be involved. Renal encephalopathy appears to be a rare complication of renal failure in ruminants, as reported in two cows and a goat, where the lesions included myelin vacuolation.2-4
Differential Diagnosis
Formulation of a differential diagnosis list for a ruminant with TN may be difficult because of the nonspecific nature of clinical signs and variety of primary disease conditions that may predispose an animal to TN. Generic systemic illness differential diagnoses are similar to those of renal origin. Diseases causing signs of acute, severe illness in ruminants include pneumonia, pleuritis, mastitis, metritis, peritonitis, endocarditis, and metabolic derangements.
■ TABLE 34.2
Differential Diagnoses for Acute Renal Failure in Ruminants
| Inorganic Compounds | Organic Compounds | Therapeutics | Endogenous Compounds | Hemodynamic Causes | Infectious Agents | Plants |
| Arsenic | Cantharidin | Aminoglycosides | Calcium oxalate | Blood loss | Malignant catarrhal fever | Castor bean (Ricin) |
| Bismuth | Carbamate fungicides | Gentamicin, neomycin, amikacin | Hemoglobin | Endotoxic shock | Coxiella burnetii | Beets (Beta) |
| Boric acid | Carbon tetrachloride | Amphotericin B | Myoglobin | Disseminated intravascular coagulation | Leptospira spp. | Bristle grass (Setaria) |
| Cadmium | Cholecalciferol- based rodenticides | Bacitracin | Renal vein thrombosis | Mycobacterium spp. | Cocklebur Xanthium) | |
| Calcium Chromium Copper Lead Mercury Molybdenum Phosphorus Sodium fluoride Uranium Zinc | Diquat Ethylene glycol Mycotoxins Natural gas condensate Ochratoxin, citrinin, fumonisin Oxalic acid Pentachlorophenol Phenolics Stillage liquid from ethanol production | Cephalosporins Doxycycline Ionophores NSAIDs Oxytetracycline Polymyxin B Sulfonamides Vitamin C Vitamin D, particularly D3 Vitamin K3 | Heat-related injury | Rift Valley fever Septicemia -Mycoplasma agalactiae -Salmonella enterica -Others | Crocus (Colchicum) Curlydock (Rumex) Daisy (Nolletia) Greasewood (Sarcobatus) Halogeton (Halogeton) Hybrid sudan or Sudan grass (Sorghum) Inkweed (Phytolacca) Jessamine (Cestrum) Kleingrass (Panicum) Kochia scoparia |
NSAIDs, Nonsteroidal antiinflammatory drugs.
Pathologic Studies
The complete blood count and serum biochemistry can provide important evidence for the presence of renal disease and clues as to its etiology.
Inflammatory diseases are common in ruminants, and the leukogram may reflect those primarily affecting the upper urinary tract. Acute inflammation affecting renal tubules may result in neutropenia or a left shift to immature (band) neutrophils. Renal enzymes and electrolytes evaluated in the serum biochemistry are useful indicators of renal function. Blood or serum urea nitrogen (BUN) is interpreted as a measure of glomerular filtration rate (GFR), reflecting function and perfusion of the kidneys. BUN is influenced by the protein level in the diet and the ability of the rumen to recycle urea. Creatinine is produced and eliminated in constant amounts in the body and is not influenced by rumen physiology, making it superior for evaluation of renal perfusion and function in ruminants, although it may be elevated above reference ranges in heavily muscled bulls with adequate renal function. Azotemia may result from prerenal, renal, or postrenal causes, with renal causes indicated by persistent isosthenuria or hyposthenuria in the absence of iatrogenic causes. Overinterpretation of a single, dilute urine sample should be avoided.Fractional excretion of (FE) electrolytes can further delineate the nature of renal azotemia. Fractional clearance of sodium has been used to help document renal failure in cattle, with values of 0% to 4% described in normal cattle.5 Age, ration, and metabolic status may affect FE values.5 When applying this test, it is prudent to compare the patient's FE value for sodium to that of an age-matched herdmate in a similar physiologic state and on a similar ration. The normal values for several urinary diagnostic indices in healthy calves have been reported.6
Hyponatremia, hypochloremia, and metabolic alkalosis may also be present with ARF, with variable potassium levels.1,7 Because the kidney is the primary organ controlling magnesium excretion in ruminants, hypermagnesemia may occur in TN, particularly under conditions of high magnesium intake.1,8 Hyperphosphatemia results from reduced phosphorus excretion in saliva during anorexia, reduced urinary phosphorus excretion, and tissue hypoxia.9,10 Hypocalcemia is also common in TN in ruminants because of reduced calcium intake, gastrointestinal stasis, urinary losses, and the competitive effect of hyperphos- phatemia.1 Metabolic acidosis may develop in juvenile ruminants with TN and concurrent diarrhea.5,10
A urinalysis should be performed on all animals with suspected renal disease. Proteinuria, hematuria, and granular casts may be found in cases of tubular necrosis.
Table 34.3 lists additional clinical and clinicopathologic criteria that may facilitate diagnosis of TN caused by nephrotoxins.
Pathophysiology
The mechanisms of TN include hemodynamic changes within the kidney, as well as ischemic and toxic damage to tubular cells. Reduced blood flow to the kidneys most often occurs during generalized loss of vascular volume, as seen with marked
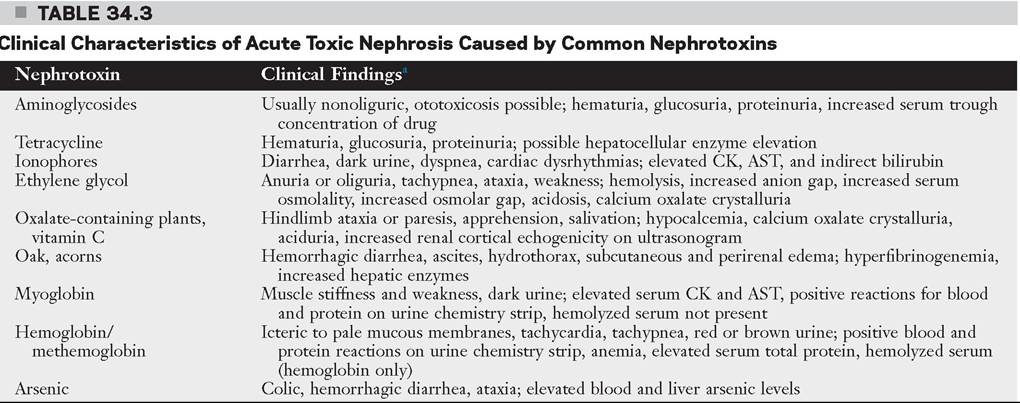
aMany general clinical characteristics of acute tubular necrosis are also present. See Clinical Signs and Clinical Pathology. AST, Aspartate aminotransferase; CK, creatine kinase.
blood loss, septicemia, endotoxemia, or severe dehydration. In ruminants, the most common primary conditions resulting in these changes include mastitis, metritis, enteritis, rumen acidosis, and intestinal accidents. These conditions may also cause infarction of the renal cortex and renal vein thrombosis. * * 4 * * * Acute, severe renal tubular necrosis has been reported in lambs as heat stress-related injury, similar to ischemic, heat-induced injury in humans.11 Prolonged, severe ischemia may destroy the tubular basement membrane, thereby preventing tubular epithelial cell regeneration.12 Rumen acidosis or other conditions resulting in severe rumen distension may additionally result in mechanical obstruction of renal vasculature, impairing renal perfusion.1
Bilateral bacterial infection of the kidneys may result in ARF or CRF as a result of destruction of nephrons by bacterial toxins and host inflammatory response. Renal infection may be established by ascending urinary tract infection or via hematogenous infection of the kidneys.
Pigment nephrosis is an endogenous toxicity from the presentation of large amounts of hemoglobin or myoglobin to the kidneys as a result of hemolytic disease or myopathies. These pigments result in renal vasoconstriction and tubular obstruction from protein coagulation.
A variety of toxins may result in significant damage to the kidneys by a variety of mechanisms that result in ARF. The high metabolic demands of renal tubular epithelial cells render them susceptible to toxins that disrupt cellular enzymes. The injury caused by most nephrotoxins is compounded by dehydration, which concentrates the toxin in the tubular filtrate, slows toxin clearance, and if severe, reduces renal perfusion. Because some nephrotoxins are therapeutic agents, it is vital that the veterinarian monitor appetite, body weight, water intake, urine output, routine urine chemistry, serum drug concentration, and serum creatinine concentration during administration of these agents. Young or elderly patients, patients with preexisting renal insufficiency or sepsis, those receiving other potentially nephrotoxic drugs, and patients on prolonged or high-dose therapy with these agents warrant the closest attention.13 Nonsteroidal antiinflammatory drugs block the effects of prostaglandins, which are important for maintenance of renal blood flow, and may cause medullary crest necrosis when used in pediatric, geriatric, and inadequately hydrated patients or for a prolonged dosing regimen.14 Some sulfonamide antimicrobials have been associated with deposition of insoluble precipitates in the renal tubules and blocking excretion of creatinine.15 Aminoglycoside antimicrobials, particularly gentamicin, have cumulative effects on the renal tubules and may cause cell death through mitochondrial oxidation and other mechanisms.13,16
Ethylene glycol, the primary ingredient in many antifreeze products, is converted by the liver into nephrotoxic metabolites, mainly glycolic acid. Additionally, calcium oxalate crystals form and are deposited in the renal tubules, causing further compromise.17 Lethal doses for ethylene glycol are 5 to 10 mL/kg in mature cattle and 2 mL/kg in preruminating calves.18,19 Insoluble oxalate crystal deposition in the renal tubules is also a common pathologic mechanism for some nephrotoxic plant poisonings including halogeton, greaseweed, pigweed, sorrel, dock, and Russian thistle.
Several nephrotoxic plants also exhibit effects on other body systems including the respiratory, gastrointestinal, cardiac, and hepatic systems, with additional symptoms observed. Many of the nephrotoxic plants, particularly those causing oxalate toxicity, are also nitrate accumulators.Treatment and Prognosis effectively achieved through IV administration of isotonic, sodium-containing fluids, with calcium and potassium supplementation as indicated. Normal (0.9%) saline or 0.45% saline + 2.5% dextrose serve as reasonable base fluids. Additional IV potassium can be substituted if indicated after initial therapy, being cautious to remain below the generally recommended toxicity rate of 0.5 mEq/kg/h. Diuresis should continue until the patient is producing sufficient volumes of urine. If cost or facilities make IV fluid therapy impractical, repeated administration of water and electrolytes by orogastric or nasogastric tube is an option. A small-bore tube can be passed through the nasal cavity into the rumen and secured to the animal's halter to allow one person to administer fluids repeatedly without the need for repeated tube passage. Placement of a small rumenostomy also would allow one person to administer fluids repeatedly with relative ease. Administration of IV or oral fluids at 1.5 to 2 times the adult maintenance level of 60 mL/kg/day may be adequate to induce diuresis. The patient should be monitored for chemosis, ventral or peripheral edema, or labored or rapid respiration, which may be indicative of overhydration. Fluid therapy should be continued until azotemia resolves, at which time the patient's voluntary fluid intake can be assessed. Oral supplementation of potassium and calcium salts may be necessary in some cases because it is often not possible to include adequate yet safe levels of these salts to IV fluids in cases of refractory hypokalemia and hypocalcemia, respectively.
Restoration of urine production is necessary in anuric or oliguric animals. If fluid therapy does not promote diuresis, furosemide (1 mg/kg IV or IM) may be administered. Repeated administration (every 1 to 2 hours) may be necessary to induce urine production. With repeated use of furosemide, the patient's serum sodium and potassium concentrations must be monitored. Mannitol (0.25 to 1 g/kg IV bolus) can be used to provide osmotic diuresis.
Vasopressors and inotropes may assist with renal perfusion but must be administered using fluid pumps as constant rate infusions. These have wide and controversial ranges of therapeutic efficacy. Drugs and dosages used anecdotally in ruminants include intravenous dopamine (2 to 5 μg/kg/min), dobutamine (5 to 10 μg/kg/min), and combination norepinephrine (0.4 μg/kg/min) + dobutamine (5 μg/kg/min) based on available information.20 It should be noted that the use of dopamine alone in cases of ARF may not be as beneficial as once thought and adverse effects have been discovered.21
Additional supportive therapy may include broad-spectrum antimicrobials against susceptible infectious agents, plasma transfusion to treat hypoproteinemia, and nutritional support through parenteral nutrition or rumen transfaunation. Antiinflammatory agents may prove useful but should be used cautiously where renal damage exists and only when the kidneys are being therapeutically well perfused. Urinalysis and FE of electrolytes can be measured in conjunction with serum monitoring parameters during intensively managed cases.
Lesions that occlude tubular blood flow (renal vein thrombosis, DIC) warrant a poor prognosis, whereas renal failure resulting from toxic causes carries a more favorable prognosis with early diagnosis and aggressive therapy. Return of appetite and progressive reduction in BUN and serum creatinine levels are positive prognostic indicators.7 Prolonged supportive treatment (2 to 3 weeks) may be necessary to allow for regeneration of tubular epithelium in cases of acute TN.