VOMITING
Most small animal practitioners agree that vomiting is one of the most common reasons that dogs and cats are presented for diagnosis and treatment. Vomiting refers to a forceful ejection of gastric and often proximal small intestinal contents through the mouth.
The vomiting act involves three stages: nausea, retching, and vomiting. It is emphasized that vomiting is simply a clinical sign of any of a number of disorders that can involve any organ system in the body. Vomiting does not constitute a diagnosis in itself.Clinical Features
Because a wide variety of disorders and stimuli can cause vomiting (Box 1-4),it may present the clinician with a major diagnostic challenge. Although
| ■BOXUd Causes of Vomiting | |
| Dietary Problems | Disorders of the Gastroesophageal Junction |
| 1. Sudden diet change | Hiatal hernia (axial, paraesophageal, diaphragmatic |
| 2. Ingestion of foreign material (e.g., garbage, grass, plant leaves) | herniation, gastroesophageal intussusception) |
| 3. Eating too rapidly | Disorders of the Small Intestine |
| 4. Intolerance to specific foods | 1. Parasitism |
| 5. Food allergy | 2. Enteritis 3. Intraluminal obstruction (foreign body, intus- |
| Drugs | susception, neoplasia) |
| 1. Intolerance (e.g., antineoplastic drugs, cardiac | 4. Inflammatory bowel disease—idiopathic |
| glycosides, antimicrobial drugs [e.g., erythromycin, | 5. Diffuse intramural neoplasia (lymphosarcoma) |
| tetracycline], arsenical compounds) | 6. Fungal disease |
| 2. Blockage of prostaglandin biosynthesis (non- | 7. Intestinal volvulus |
| steroidal antiinflammatory drugs) 3. Injudicious use of anticholinergics | 8. Paralytic ileus |
| 4. Accidental overdosage | Disorders of the Large Intestine 1. Colitis |
| Toxins | 2. Obstipation |
| 1. Lead 2. Ethylene glycol | 3. Irritable bowel syndrome |
| 3. Zinc | Abdominal Disorders |
| 4. Others | 1. Pancreatitis 2. Zollinger-Ellison syndrome (gastrinoma of |
| Metabolic Disorders | pancreas) |
| 1. Diabetes mellitus | 3. Peritonitis (any cause, including feline infectious |
| 2. Hypoadrenocorticism | peritonitis) |
| 3. Renal disease | 4. Inflammatory liver disease |
| 4. Hepatic disease | 5. Bile duct obstruction |
| 5. Sepsis | 6. Steatitis |
| 6. Acidosis | 7. Prostatitis |
| 7. Hyperkalemia | 8. Pyelonephritis |
| 8. Hypokalemia | 9. Pyometra |
| 9. Hypercalcemia | 10. Urinary obstruction |
| 10. Hypocalcemia | 11. Diaphragmatic hernia |
| 11. Hypomagnesemia 12. Heatstroke | 12. Neoplasia Neurologic Disorders |
| Disorders of the Stomach | 1. Psychogenic (pain, fear, excitement) |
| 1. Obstruction (e.g., foreign body, pyloric mucosal | 2. Motion sickness (rotation or unequal input from |
| hypertrophy, external compression) | the labyrinths) |
| 2. Chronic gastritis (superficial, atrophic, hypertrophic) | 3. Inflammatory lesions (e.g., vestibular) |
| 3. Parasites (Physaloptera spp.—dog and cat; Ollulanus | 4. Edema (head trauma) |
| tricuspis—cat) | 5. Autonomic or visceral epilepsy |
| 4. Gastric hypomotility 5. Bilious vomiting syndrome | 6. Neoplasia |
| 6. Gastric ulcers | Miscellaneous Causes of Vomiting |
| 7. Gastric polyps | 1. Heartworm disease (feline) |
| 8. Gastric neoplasia 9. Gastric dilatation 10. Gastric dilatation-volvulus | 2. Hyperthyroidism (feline) |
Modified from Tams TR:Vomiting,regurgitation, and dysphagia. In Ettinger SJ, ed: Textbook of veterinary internal medicine, ed 4, vol 1, Philadelphia, 1995,WB Saunders.
vomiting does not always signify the presence of a serious disorder, it may be the first indication of intestinal obstruction, renal failure, pancreatitis, parvovirus enteritis, addisonian crisis, drug toxicity, neoplasia, and others. A complete historical review with emphasis on all body systems is essential for determining a realistic and effective initial work-up plan and treatment protocol.
All too often, early concentration on only the GI tract leads to a misdiagnosis and inappropriate treatment for the cause of the vomiting.As previously discussed, it is essential that the clinician make a clear differentiation between regurgitation and vomiting at the outset. If there is uncertainty about whether or not regurgitation is occurring after the history is reviewed, survey thoracic radiographs should be made to evaluate for possible esophageal dilation. Contrast studies may occasionally be necessary to identify the presence of esophageal dilation.
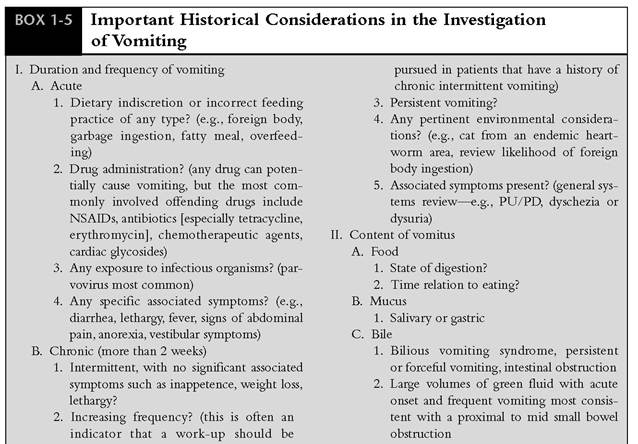
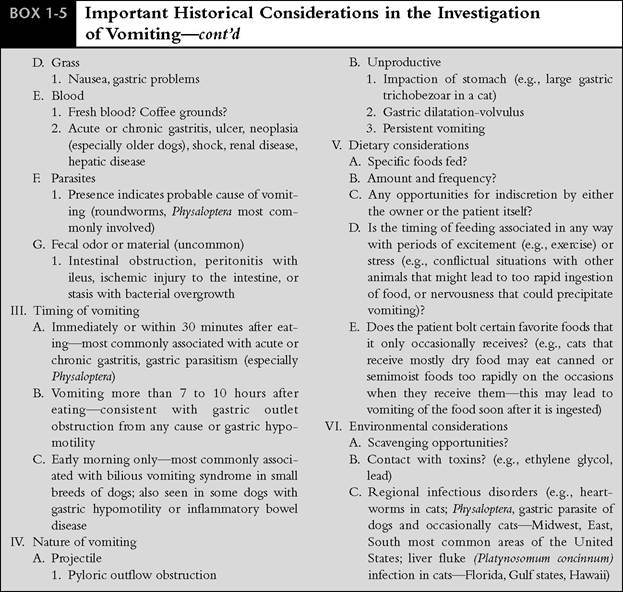
Consideration of the following historical features is often useful in assessing and diagnosing disorders that cause vomiting (Box 1-5):
• Duration of signs and systems review
• Content of the vomitus
• Time relation to eating
• Nature (e.g., type, frequency) of vomiting
• Dietary and environmental history
The line of questioning should begin with determining if the vomiting is an acute problem or is chronic (longer than 2 weeks in duration) and whether there has been any blood in the vomitus. The signalment, immediate signs, past pertinent history, and beneficial or deleterious effects of any drugs that may have been administered (either for the immediate symptoms or as treatment for another disorder) should be reviewed. In particular it should be determined whether any nonsteroidal antiinflammatory drugs (e.g., aspirin, carprofen, etodolac, flunixin meglumine [Banamine], phenylbutazone, ibuprofen [Motrin, Nuprin], piroxicam [Feldene]) have been used. Gastric and intestinal erosions and potentially serious ulceration may develop in conjunction with their use. Nephrotoxicity may also
NSAIDs, Nonsteroidal antiinflammatory drugs; PU/PD, polyuria/polydypsia.
occur. Inhibition of renal prostaglandins can be associated with renal ischemia and acute renal failure.
Fortunately this syndrome is uncommon. However, patients with hypovolemia, congestive heart failure, or preexisting renal insufficiency may be at increased risk.Acute pancreatitis may be a component of a drug reaction; agents that have been implicated include azathioprine (Imuran), thiazide diuretics, furosemide, sulfonamides, tetracycline, L-asparaginase, and others.Occasionally a chronic asymptomatic disorder is first manifested by an acute onset of vomiting, which may then persist as either a frequent or a sporadic problem until definitive treatment is instituted. Inflammatory bowel disease is an example of a common disorder that may present in this way. Specific information regarding diet (type of food, number and timing of feedings each day, amount fed per meal, any recent changes); vaccinations (consider systemic disorders such as distemper, parvovirus, feline infectious peritonitis); travel history; and environment (e.g., exposure to toxins, ingestion of spoiled food or foreign bodies, likelihood of GI parasites or infectious problem such as parvovirus enteritis, feline patient from an endemic heartworm area) is obtained in all cases. A thorough systems review with questions investigating any significant occurrence of potentially important signs such as PU/PD, coughing and sneezing, dysuria, or dyschezia should also be addressed. This routine systematic approach will help to alleviate diagnostic “tunnel vision” on the part of the clinician. For example, a history of PU/PD and acute vomiting in an older intact female dog immediately suggests the possibility of pyometra (also rule out primary renal disease), and the presence of dyschezia in conjunction with vomiting may be consistent with vomiting secondary to colitis (approximately 30% to 35% of dogs with colitis also have vomiting, which may occur before or in conjunction with the onset of large bowel signs).
A description of the vomiting episodes, including any association with eating or drinking, yields important information in some cases.
Normally all food should be evacuated from the stomach by 7 to 10 hours after ingestion. The presence of food and its state of digestion will depend on dietary composition (with high-fat diets the stomach empties more slowly), gastric secretions and motility, presence of any gastric outflow obstruction, and time elapsed since ingestion. Vomiting shortly after eating most commonly suggests dietary indiscretion or food intolerance, overeating, stress or excitement, gastritis, or a hiatal disorder. Vomiting of undigested or partially digested food more than 7 to 10 hours after eating is an important clinical sign that usually indicates a gastric motility disorder or gastric outflow obstruction. Dogs with hypomotility may vomit undigested food several hours to 10 to 18 hours or more after eating and often exhibit a cyclic pattern of clinical signs. This disorder has been recognized much more frequently in recent years. Misconceptions commonly lead to misdiagnosis and mismanagement of affected patients. It is often incorrectly assumed that gastric retention means gastric outflow obstruction, and unnecessary surgery such as pyloromyotomy may be performed. It is now well recognized that pyloromyotomy procedures are not commonly indicated in dogs or cats with chronic vomiting.Causes of gastric outflow obstruction include foreign bodies, antral and/or pyloric mucosal hypertrophy, gastric and duodenal ulcers, antral or pyloric neoplasia or polyps, and external compression on the antrum and pylorus (e.g., abscess, mass). Foreign bodies are identified much more commonly than the other disorders listed in Box 1-4. All are characterized by vomiting, which may occur shortly or a number of hours after eating, and occasionally projectile vomiting occurs.
Significant information can often be obtained from a complete description of the color and consistency of the vomitus, especially when interpretation is made in conjunction with a review of clinical signs. As previously discussed, if food is present, the degree of digestion and time since the most recent meal should be determined. Presence of bile in the vomitus is not unusual because vomiting begins with jejunal retroperistalsis and intestinal contents are swept into the stomach before the actual act of vomiting. Bile may appear as a yellow or green coloration. Bile is often present when vomiting is due to inflammatory bowel disease, idiopathic or secondary gastric hypomotility (bile alone or bile with food), intestinal foreign bodies, and pancreatitis. Chronic intermittent bilious vomiting in small breeds of dogs, especially when it occurs mostly in the early morning hours, is most suggestive of reflux gastritis. The presence of bile helps to rule out a complete pyloric obstruction.
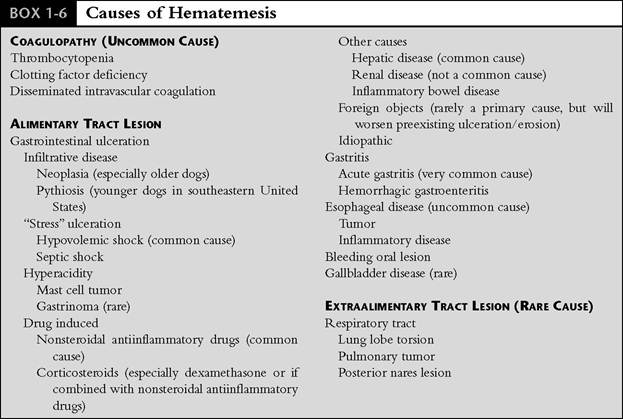
Expulsion of large amounts of predominantly greenish-colored fluid from a patient with acute vomiting is most consistent with a proximal to mid small bowel obstruction. Lethargy, dehydration, and abdominal pain are generally present in affected patients. In general, the more proximal a bowel obstruction is located, the more fulminant the clinical signs will be. Small amounts of blood may be present in any case of gastric or duodenal mucosal compromise with erosions or ulceration (e.g., hypovolemia with resultant loss of integrity of the gastric mucosal barrier, drug-induced damage, acute or chronic gastritis or inflammatory bowel disease, gastric or duodenal ulceration, or neoplasia). Hematemesis may also be caused by a coagulopathy or ingestion of blood from another site (e.g., mouth, nasal sinuses, lungs). Large clots of blood or “coffee grounds” (blood altered by and mixed with gastric juice) usually indicate a more significant degree of erosions or ulceration. Fresh blood is usually altered in the stomach to the dark brown or black color known as “coffee grounds” in a matter of minutes. Presence of bright-red blood in the vomitus thus indicates very recent or active hemorrhage.
Clinicians should be aware that not all patients with gastric ulcers have hematemesis or even vomit. This fact highlights the importance of obtaining a thorough history to determine if any “ulcerogenic factors” could be present. Recent onset of hematemesis in a patient with chronic vomiting is often a sign that a potentially serious and worsening disorder is present. Such conditions as neoplasia with ulceration, uremic gastritis, or chronic severe gastritis with erosive changes should be considered, and diagnostic evaluation to determine the cause should be expedited. Potential causes of hematemesis are listed in Box 1-6.
A fecal odor suggests intestinal obstruction, peritonitis with ileus, ischemic injury to the intestine, or stasis with bacterial overgrowth. Projectile vomiting is an imprecise term that is used to describe forceful ejection of vomitus from the mouth, which is expelled a considerable distance. Its occurrence suggests a significant degree of gastric or proximal small bowel obstruction (foreign body, large antral or pyloric polyps, neoplasia, pyloric hypertrophy). In my experience this clinical sign occurs infrequently.
Chronic intermittent vomiting is a common presenting complaint in veterinary medicine. Often there is no specific time relation to eating, the content of the vomitus varies, and the occurrence of vomiting may be very cyclic in nature. Depending on the disorder, other signs, such as diarrhea, lethargy, inappetence, weight loss, and salivation (nausea), may occur as well. When presented with this pattern of clinical signs in patients in which metabolic disorders, GI parasitism, and adverse food reactions have been ruled out, the clinician should strongly consider chronic gastritis, inflammatory bowel disease, irritable bowel syndrome, and gastric motility disorders as leading differential diagnoses. A detailed work-up, including gastric and intestinal biopsies, is often required for definitive diagnosis in these cases. It is important to note that chronic intermittent vomiting is a common clinical sign of inflammatory bowel disease in both dogs and cats. Diarrhea may or may not be a concurrent problem in patients with inflammatory bowel disease. Vomiting from systemic or metabolic causes may be an acute or chronic sign, and generally there is no direct correlation with eating and no predictable vomitus content.
The concomitant presence of diarrhea with vomiting often provides important diagnostic clues. Vomiting preceding diarrhea suggests toxic ingestion, a progressively severe disease of the small intestine such as viral enteritis (e.g., due to parvovirus or rotavirus), pancreatitis, or acute colitis. Also, infections with parasites, including Giardia and roundworms, can cause vomiting that precedes the
From Willard M: Clinical manifestations of gastrointestinal disorders. In Nelson RW, Couto CG, eds: Essentials of small animal internal medicine, St.Louis, 1992, Mosby-Year Book.
onset of diarrhea. Occasionally Giardia may cause chronic intermittent vomiting without diarrhea or with only sporadic bouts of abnormal stools. Diarrhea preceding vomiting usually suggests primary but progressive intestinal damage, and vomiting is generally a secondary event in these patients. This includes patients that have gastric hypomotility secondary to inflammatory bowel disease.
Physical Examination
It is important to stress the enormous significance of a complete history and physical examination in evaluation of a vomiting patient. An all too frequent error in clinical practice is to make a diagnosis based on an incomplete history and cursory examination. This may lead to use of unnecessary diagnostic tests and inappropriate treatment. Essential early diagnosis of a serious disorder may be missed. A systematic approach can be both thorough and time efficient. Areas to receive emphasis in a vomiting patient are listed here.
The first step in physical examination is to assess the patient's overall attitude, posture, and energy level (i.e., active versus lethargic). This will often assist the clinician in determining to some degree the seriousness of the patient's condition and its degree of discomfort, if any exists. Observe the patient! Will any pain relief or antiemetic medication to control nausea be needed? It is often very reassuring to the owner when the clinician begins the examination by showing interest in how the patient has been acting and feeling. Patients that are experiencing a significant degree of nausea often have a forlorn expression, swallow frequently, and salivate (Figure 1-2). Patients with intestinal foreign body obstruction, pancreatitis, gastric neoplasia, and other serious conditions are often quite subdued at the time of presentation. These types of observations can often be made as the history is being discussed and recorded. Careful observation should be continued throughout any subsequent period of hospitalization.
The mucous membranes are evaluated for evidence of blood loss, dehydration, sepsis, shock, and jaundice. Salivation suggests the presence of nausea (common causes of salivation are listed in Box 1-7). An oral examination may reveal a part of an oral or pharyngeal foreign body that may extend to the stomach or intestine. The best example of this is a linear foreign body in a cat in which a portion of the foreign material loops around the tongue at the frenulum, with the free

Figure 1-2 Typical appearance of a puppy quite ill from parvovirus enteritis. This puppy was depressed, reluctant to move, and nauseated. Watery diarrhea was present in the cage.
ends subsequently advancing along the intestinal lumen as a result of progressive peristalsis. Intestinal plication with potential for perforation results. It is extremely important that an oral examination with careful evaluation of the frenulum area be done in all vomiting cats. In some cases, mild tranquiliza- tion (e.g., ketamine 5 to 8 mg intravenously) is required so that a definitive examination can be done (Figure 1-3). Dogs occasionally have similar foreign body positioning, so a careful oral examination is important in this species as well. The cervical soft tissues of vomiting cats should be palpated for an enlarged thyroid nodule or nodules (hyperthyroidism commonly causes vomiting). Hyperthyroidism should be considered in any cat 5 years of age and older. Cardiac auscultation may reveal rate and rhythm abnormalities that can
BOX 1-7
Causes of Salivation
Nausea
Stomatitis (including chronic feline gingivitis/ stomatitis/pharyngitis)
Direct oral stimulation (e.g., ingestion of caustic materials, foreign body, electric cord injury, oral neoplasia)
Chemical poisoning (organophosphates, carbamates, metaldehyde)
Esophagitis
Esophageal foreign body
Portosystemic shunt (especially in cats)
Medications (especially in cats; e.g., trimethoprim/ sulfadiazine)
Rabies
Conditioned reflex (Pavlovian response)

Figure 1-3 Linear foreign body (dental floss) under the tongue of a cat that was tranquilized in order to facilitate a thorough oral examination. The cat was presented because of acute vomiting, anorexia, and lethargy.
occur with metabolic disturbances such as hypoadrenocorticism (bradycardia,weak femoral pulses), infectious enteritis with septic shock (tachycardia, weak pulses), or gastric dilatation-volvulus (tachycardia, weak pulses, pulse deficits).
A careful assessment is made for either generalized or localized abdominal pain (e.g., pancreatitis, foreign body, pyelonephritis, hepatic disease, regional inflammation in inflammatory bowel disease). Other abdominal factors to evaluate include abnormal organ size (e.g., hepatomegaly, small or large kidneys), presence of a mass (foreign body, intussusception, lymphadenopathy, neoplasia), degree of gastric distention (increased with gastric dilatation, gastric dilatation-volvulus, gastric retention due to hypomotility or outflow obstruction), and altered bowel sounds.
Auscultation of the abdomen may occasionally be useful. Bowel sounds are often absent in peritonitis and increased in acute inflammatory disorders. An increased pitch suggests distention of intestinal loops. Serial palpation may be required to detect problems in some patients, including those with tensing of the abdominal wall due to pain or nervousness and when a foreign body, mass, or intussusception (especially sliding or ileocolic intussusceptions) is located in the craniodor- sal abdomen, where the ribs prevent careful manipulation. It is often helpful to have someone hold the patient with the front end elevated so that the anterior abdominal organs shift caudally a little, into a more palpable position. It is also recommended that a two-hand palpation technique be used, starting with gentle extension of one had under each side of the rib cage. Finally, if history or radiographs strongly suggest the possibility of a foreign body or intussusception that has eluded initial palpation efforts, it may be useful to sedate the patient so that further gentle palpation can be done. Difficult-to-find foreign bodies can often be readily palpated with the assistance of sedation or general anesthesia. Clinicians need to exercise great care when palpating patients that may have sharp intestinal linear foreign bodies or a large turgid uterus due to pyometra——forceful palpation could cause perforation of the intestine or uterus in these situations!
A rectal examination is always done in dogs to evaluate stool characteristics for fresh blood or mucus, melena, or presence of foreign material; to obtain a fresh stool sample for parasite and possibly cytologic examination; and to evaluate the mucosa for sensitivity and abnormal texture. Serial rectal examinations are most important when GI bleeding is either suspected or has been identified. Because patient size precludes rectal examination in many small cats, careful assessment of stool characteristics is done instead in such patients.
Diagnostic Plan
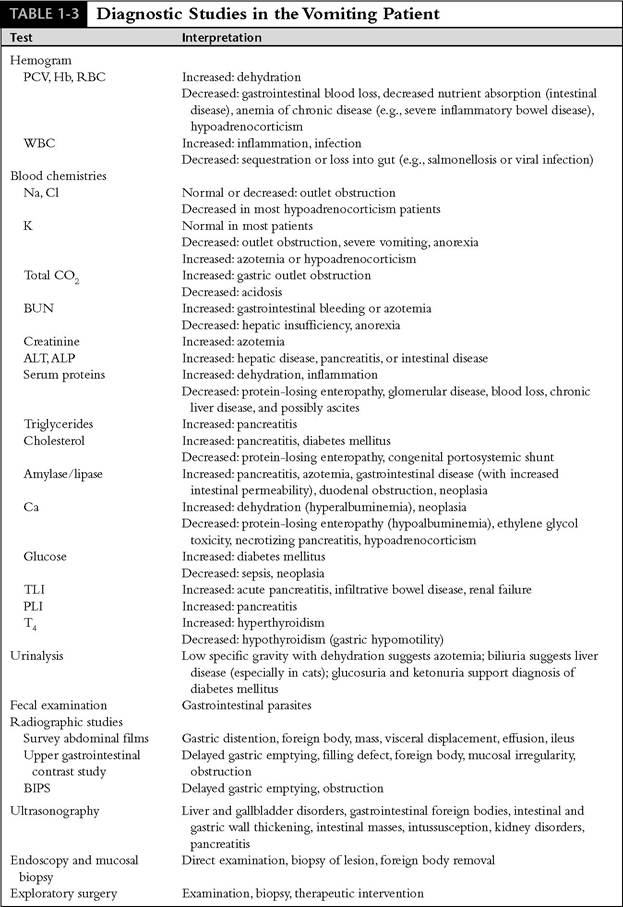
Vomiting patients in some cases require an extensive work-up, but an organized approach will help to minimize the tests necessary for an early diagnosis. The most important initial considerations in determining what tests to perform are (1) signalment, (2) duration (acute [less than 7 to 14 days] versus chronic), (3) frequency of vomiting, (4) degree of symptoms (mild versus moderate to severe illness, i.e., life-threatening), (5) other clinical signs (e.g., shock, melena, abdominal pain), and (6) physical examination findings. Diagnostic studies and their possible results are summarized in Table 1-3.
If reasonable concern is established, a minimum database, including CBC, biochemical profile (or specific tests for evaluation of liver, kidneys, pancreas,electrolytes),complete urinalysis (determination of pretreatment urine specific gravity is extremely important for accurate differentiation of prerenal azotemia and primary renal disease), and fecal examination, is essential. Intestinal parasites, including Giardia, can cause vomiting and diarrhea. Survey abdominal radiographs are indicated if historical information suggests that they should be done or if thorough abdominal palpation is not possible or suggests an abnormality
Modified from Burrows CFrVomiting and regurgitation in the dog: a clinical perspective. In Viewpoints in veterinary medicine, ed 2, LehighValley, Pa, 1993,Alpo Pet Foods.
PCV, Packed cell volume; Hb, hemoglobin; RBC, red blood cell count; WBC, white blood cell count; Na, sodium;
Cl, chloride; K, potassium; CO2, carbon dioxide; BUN, blood urea nitrogen; ALT, alanine aminotransferase; ALP, alkaline phosphatase; Ca, calcium; TLI, trypsin-like immunoreactivity; PLI, canine pancreatic lipase immunoreactivity; T4, thyroxine; BIPS, barium-impregnated polyethylene spheres.
(e.g., foreign body, pancreatitis, pyometra). Unfortunately these tests are often not done early enough. Even if baseline results are unremarkable, such studies are more than justified because they help to rule out serious problems at the outset (e.g., vomiting due to renal failure, diabetes melli- tus, liver disease). Alternatively, any abnormalities provide direction for initial treatment and further diagnostics.
A recently developed test, canine and feline pancreatic lipase immunoreactivity (cPLI, fPLI), is now available for diagnosis of pancreatitis in dogs and cats. This assay specifically measures the concentration of lipase originating from the exocrine pancreas. Because there are many lipases from different cellular origins, running total serum lipase levels is not specific enough for diagnosing pancreatitis. The assay for pancreatic lipase immunoreactivity uses specific antibodies directed against pancreatic lipase and therefore directly measures pancreatic lipase. Preliminary studies have shown that serum PLI concentration is both very specific and sensitive for diagnosis of pancreatic inflammation. The test is available at The GI Laboratory at Texas A&M University in College Station,Texas.
The decision to perform more in-depth diagnostic tests is based on ongoing clinical signs, response to therapy, and initial test results. These tests may include an ACTH stimulation test to confirm hypoadrenocorticism in a patient with an abnormal sodium-potassium ratio (Na:K) or suggestive CBC changes (anemia, lymphocytosis, and eosinophilia in a stressed patient) or to investigate for this disorder if electrolytes are normal (approximately 10% of dogs with hypoadrenocorticism do not present with abnormal electrolyte levels). Hypoadrenocorticism is more common in young to middle-age female dogs. A complete barium series is useful for identification of a gastric or intestinal foreign body, gastric hypomotility, gastric outflow obstruction, and partial or complete intestinal obstruction. Liquid barium contrast studies may be normal in patients with gastric hypomotility disorders. Measuring the emptying of barium mixed with food is a better test for evaluating gastric motility. Solids empty by a different mechanism from that for liquids, and it is not uncommon for patients with a known gastric emptying disorder to empty a liquid meal in a timely manner.
Medical ID Systems, Inc, Grand Rapids, MI 49512-3942.
Alternatively, small, nondigestible radiopaque markers (e.g., BIPS*) can be mixed with food for a radiographic series to study motility.
BIPS are inert, white, radiopaque, barium- impregnated polyethylene spheres (BIPS). They have a density similar to food but are sufficiently radiodense to show clearly on abdominal radiographs (Figure 1-4). All animals receive exactly the same dose of BIPS. They can be administered with or without food, depending on the clinical situation. BIPS are dispensed in capsule form. There are two sphere sizes contained in each dose application. There are 10 larger spheres (5 mm in diameter) and 30 smaller spheres (1.5 mm in diameter). The primary function of the large BIPS is the detection of GI tract obstructions. The small BIPS mimic the passage of food, and their transit through the GI tract provides an accurate estimate of the gastric emptying rate and intestinal transit time of food. Instructions on the use of BIPS are available from the distributor. Also, references are listed at the end of this chapter.
An air contrast gastrogram is often very useful for identifying gastric foreign bodies in cases in which survey films alone are not diagnostic (Figure 1-5). Confirmation of presence of a gastric foreign body may not be made in some
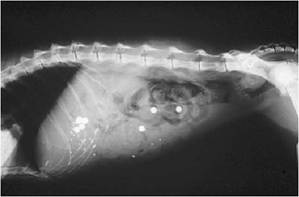
Figure 1-4 Lateral abdominal radiograph of a 15-year-old cat taken 24 hours after the start of a BIPS study to evaluate GI motility. This cat had presenting symptoms of intermittent vomiting and diarrhea. Many BIPS spheres remain in the stomach many hours after they would have exited the stomach of a cat with normal motility. The stomach should be completely empty after a meal by 7 to 10 hours. Small bowel transit time was also prolonged. This scattered pattern of BIPS is consistent with ileus. Endoscopy was subsequently performed, and moderate to severe inflammatory bowel disease was diagnosed. It was thought that the delayed motility resulted from the infiltrative bowel disease. Initial treatment included corticosteroids, cisapride (for GI promotility effect), and a diet featuring a protein source that was novel to this cat.
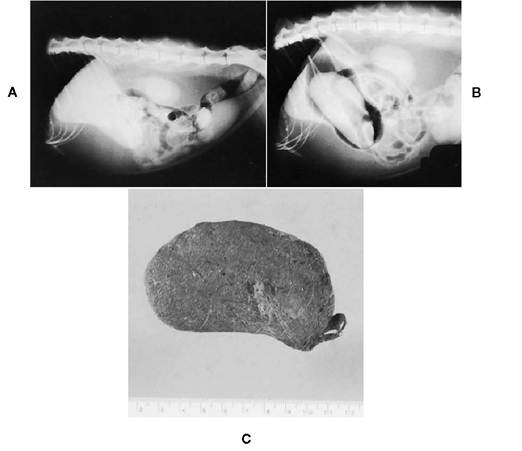
Figure 1-5 A, Lateral abdominal radiograph from a 10-year-old feline immunodeficiency virus (FIV)-positive cat with intestinal lymphoma. The cat had a gradually decreasing appetite, recent onset of intermittent vomiting, and occasional episodes of nonproductive retching.Abdominal palpation revealed a doughy mass in the region of the stomach. This radiograph shows that the stomach is distended and has a soft tissue/fluid opacity. The small intestine and colon are normal. B, Air gastrogram (40 ml of air was injected through a small feeding tube into the stomach while the cat was lightly tranquilized). A large mass density within the lumen of the stomach is consistent with a gastric trichobezoar. This simple procedure allowed rapid confirmation that a foreign body was present in the stomach. C, Trichobezoar that was surgically removed from the cat. The trichobezoar was 9 cm in length, and its configuration was similar to the inside of the stomach.
cases in which a barium series is done until most of the barium has left the stomach because a large barium pool often obscures foreign objects. Barium swallow with fluoroscopy is often necessary for diagnosis of hiatal hernia disorders and gastroesophageal reflux disease. Endoscopy is also useful for identifying these disorders.
Serum bile acids assay is used to assess for significant hepatic disease, including portosystemic shunts and chronic severe liver disease, when the liver enzymes are normal or only mildly elevated. Because vomiting is a frequent presenting sign in cats with heartworm disease, a feline heartworm antibody test should be done to investigate this possibility. In endemic areas testing cats for heartworm disease should be considered part of the minimum database. Because most cats with heartworm disease are amicrofilaremic, tests for microfilaria are usually negative. Antigen tests are also frequently negative. Thoracic radiographs may provide important clues in a cat with heartworm disease. Suggestive findings include right ventricular enlargement, pulmonary lobar artery enlargement, and pulmonary parenchymal disease. The caudal lobar arteries usually show the earliest radiographic changes, with the left and the right being equally affected. These changes are best recognized on the ventrodorsal or dorsoventral views. Some cats also have hyperglobulinemia. The presence of both peripheral eosinophilia and basophilia is also suggestive of heartworm disease in cats.
Thyroid testing should also be done on vomiting cats 5 years of age and older to evaluate for hyperthyroidism. It is important to remember that cats with hyperthyroidism may have thyroid hormone levels that fluctuate into the normal range for several days at a time early in the course of the disease. If hyperthyroidism is still suspected after an initial serum thyroxine (T4) level is shown to be normal, either the test should be repeated in 1 to 3 weeks or, alternatively, other tests can be run. Alternative tests include the triiodothyronine (T3) suppression test, free T4 by equilibrium dialysis (fT4ED), TRH stimulation test, or performance of a technetium scan. In cats with a total T4 (TT4) in the upper 50% of the basal resting range, an elevated fT4ED in the face of clinical signs is highly predictive of hyperthyroidism. Due to the simplicity of running an fT4ED versus performing a T3 suppression test or TRH response test, fT4ED should be the first test run for diagnosis of cats with hormonally occult (normal TT4) hyperthyroidism.
Chronic vomiting in cats is occasionally due to infection with the gastric parasite Ollulanus tricus- pis. Young, free-roaming cats are most often affected. Diagnosis is made by evaluation of gastric contents via the Baermann technique or by examination of filtered vomitus using a ?40 or dissecting microscope for detection of the nematode (Figure 1-6). Xylazine (Rompun) can be administered at 1 mg/lb intramuscularly to stimulate vomiting in order to collect the gastric secretions.
Serum gastrin levels are run if a gastrinoma (Zollinger-Ellison syndrome) is suspected. Gastrinoma, a gastrin-secreting tumor usually found in the pancreas, is infrequently seen in clinical practice. Clinical signs include chronic vomiting and/or diarrhea, weight loss, and anorexia. Middle-age to older dogs are most commonly affected (gastrinomas are quite rare in cats). The clinician should consider running a serum gastrin level in patients with chronic vomiting and wasting disease that are not readily explained by more routine diagnostic testing (i.e., baseline blood tests, urinalysis, radiography, and endoscopy).
One of the most reliable and cost-efficient diagnostic tools currently available for evaluation of vomiting is flexible endoscopy. Endoscopy allows for direct gastric and duodenal examination, mucosal biopsy from these areas, and in many cases gastric foreign body retrieval. Endoscopy is considerably more reliable than barium series for diagnosis of gastric erosions, ulceration, chronic gastritis, gastric neoplasia, and inflammatory bowel disease.Vomiting due to presence in the upper GI tract of the parasite Physaloptera is best diagnosed via direct visualization at endoscopy. The nema-
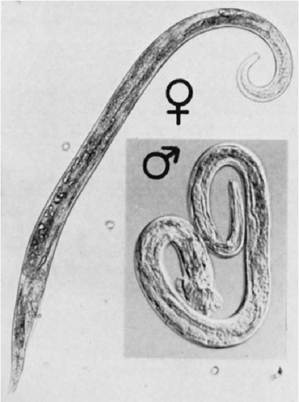
Figure 1-6 Ollulanus tricuspis from a leopard (?140). Diagnosis is usually based on finding adult specimens of this viviparous species in vomitus. (From Georgi JR: Helminths. In Georgi JR, Georgi ME, eds: Parasitology for veterinarians, ed 5,Philadelphia, 1990,WB Saunders.)
tode parasites can be readily seen on the surface of the gastric mucosa and retrieved through the endoscope working channel for definitive identification (Figure 1-7). It is stressed that biopsy samples should always be obtained from the stomach and, whenever possible, the small intestine during endoscopic procedures regardless of gross mucosal appearance. Normal gastric biopsy results may support gastric motility abnormalities, psychogenic vomiting, or irritable bowel syndrome or may be noncontributory (i.e., look elsewhere for diagnosis). Many dogs and cats with vomiting due to inflammatory bowel disease have no abnormalities on gastric examination or biopsy. If only gastric biopsies are performed, the diagnosis may be missed. As previously mentioned, some patients with colitis both vomit and have diarrhea. If large bowel symptoms are present in conjunction with vomiting, the colon should be examined and biopsies performed as well. Flexible endoscopy equipment should be used whenever possible so that the entire colon, including ascending colon, cecum, and terminal ileum, can be examined. Diagnosis of the rare ileocolic or cecocolic intussusception case that may

Figure 1-7 Multiple Physaloptera nematodes (arrows) lying on the gastric mucosa in a dog. These nematodes may cause the chronic vomiting and histologic lesions of lymphocytic-plasmacytic gastritis. (From Jergens AE, Moore FM: Endoscopic biopsy specimen collection and histopathologic considerations. In Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.)
have eluded diagnosis up to this point can be readily made on direct visualization of these areas. Examination or biopsy may also reveal typhlitis.
Ultrasonography can be useful in the diagnostic work-up of a number of disorders that can cause vomiting (see Chapter 2).Among the problems that may be detected with ultrasonography are certain disorders of the liver (e.g., inflammatory diseases, abscessation, cirrhosis, neoplasia, vascular problems) and gallbladder and bile ducts (cholecystitis, choleliths, bile duct obstruction), GI foreign bodies, intestinal and gastric wall thickening, intestinal masses, intussusception, kidney disorders, pancreatitis, and others. Needle aspirations and/or biopsies can be done at many sites under ultrasound guidance.
Abdominal exploratory is indicated for a variety of problems, including foreign body removal, intussusception, gastric mucosal hypertrophy syndromes, procurement of biopsy samples, and resection of neoplasia. If the diagnosis is unclear on examination, gastric and small intestinal (two to three samples total) biopsies must be performed. In a majority of dogs and cats with gastritis and inflammatory bowel disease, no gross abnormalities are detected at exploratory. Samples should also be obtained from liver and any enlarged lymph nodes. Also, any visible abnormalities in the pancreas warrant biopsy of this organ. Pancreas biopsy is a safe procedure when done properly.
Timing of Work-up
The frequency and duration of vomiting can vary from weeks to years. In animals with chronic, slowly progressive disorders, vomiting may be only a sporadic event with or without occasional periods of increased frequency or severity possibly associated with flare-ups of the disease process. Clinicians often ask when a patient with a disorder characterized by intermittent vomiting should undergo a detailed diagnostic work-up. Indeed, it is not unusual for some cats, several of my own included, to vomit once or twice every 1 to 2 weeks or so for many months or years without any apparent untoward effect. A variety of factors are usually involved in the decision-making process regarding when diagnostic evaluation should be undertaken. The foremost factors include development of any concurrent worrisome signs, such as inappetence, weight loss, signs of abdominal discomfort such as cramping, presence of leukocytosis and/or hypoproteinemia, any signs of hyperthyroidism in cats to suggest advancing inflammatory bowel disease, and, very importantly, the degree of the owner's concern and level of interest in finding answers regarding his or her pet's problem.
In general, I recommend that a work-up be started if the frequency of vomiting or degree of any signs associated with the vomiting (e.g., lethargy, discomfort, inappetence) begins to increase. Always keep in mind that as disease processes worsen they are frequently more difficult to bring under control. With the availability of endoscopy and our ability to utilize it for examination and biopsy of the stomach and small intestine, in a significantly noninvasive manner when compared with surgery, it is definitely reasonable to recommend its use even in patients with mild clinical signs. A countless number of my patients from over the years come to mind during this discussion, but two in particular should help make a lasting point here. Both demonstrated only mild clinical signs, which included intermittent vomiting and mild occasional lethargy. Each, however, had a serious life-threatening problem that was fortunately diagnosed early enough for the patient to undergo meaningful treatment. A brief account of their histories follows.
In early 1988 I examined a 10-year-old neutered male domestic short hair (DSH) cat with a history of intermittent vomiting of 7 weeks' duration. There was a gradual increase in frequency over the last 2 weeks, no weight loss, and a normal appetite.Although the owner did not have a great deal of money to spend, he expressed concern about his cat's well-being and requested that we try to find out what was wrong while keeping his cost-containment concerns in mind. The cat weighed 12 lb, and physical examination was unremarkable other than signs of vague anterior abdominal discomfort. A CBC, biochemical profile, serum T4, feline leukemia virus (FeLV), feline immunodeficiency virus (FIV) test, and a urinalysis were run. Radiography was bypassed in favor of endoscopy (greater sensitivity and likelihood of definitive diagnosis). Endoscopy revealed a large mass in the fundus of the stomach, which was found to be lymphoma (Figure 1-8). Intestinal biopsy specimens revealed moderate lymphocytic- plasmacytic enteritis. After 5 months of chemotherapy (no surgery was done), the mass was no longer detectable at endoscopy (Figure 1-9). After 1 year of chemotherapy there was no histologic evidence of lymphoma and chemotherapy was discontinued. Subsequent yearly endoscopic examination and biopsy of the stomach and duodenum revealed no evidence of recurrence of the lymphoma. Interestingly, the cat still had a
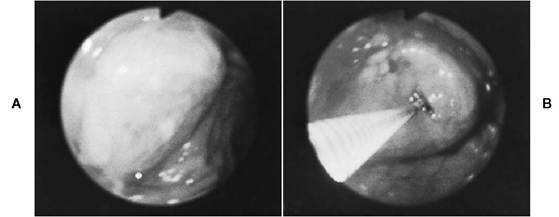
Figure 1-8 A, Close-up endoscopic view of a large mass in the gastric fundus of a 10-year-old cat with a 7-week history of intermittent vomiting. B, Biopsy forceps are advanced into the mass under endoscopic guidance. The histologic diagnosis was lymphoma. (From Tams TR: Gastroscopy. In Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.)
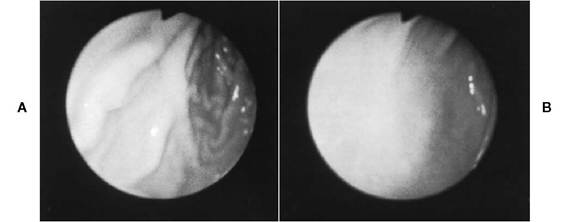
Figure 1-9 Five-month follow-up endoscopic examination of the cat described in Figure 1-8. Treatment involved chemotherapy (prednisone, cyclophosphamide, vincristine) alone. No surgery was done. A, Forward view of proximal stomach at mild distention. The mass is no longer visible, and the rugal folds are smooth. B, Same site as A with moderate distention. The mucosa at the original site of the mass appears whiter than the surrounding mucosa. (From Tams TR: Gastroscopy. In Tams TR, ed: Small animal endoscopy, ed 2, St. Louis, 1999, Mosby.)
moderate degree of inflammatory bowel disease, and antiinflammatory therapy (prednisone) was maintained. If the dose was decreased too much, vomiting began to recur. The cat lived to the age of 17 years, 7 years beyond the diagnosis of gastric lymphoma.
In 1992 I evaluated a 9-year-old neutered male Bouvier with a history of intermittent vomiting of 5 months' duration (only one to two episodes per week and with no worrisome associated signs). The owners became concerned because they felt the dog was sleeping a little more than normal, and they requested that their regular veterinarian begin investigating the problem. A CBC, biochemical profile, serum T4, urinalysis, fecal examination for parasites, and survey radiographs of the thorax and abdomen were unremarkable. The dog was then referred for endoscopy, which revealed a large proliferative mass involving the entire pyloric canal and the proximal duodenum just aboral to the pylorus (Figure 1-10). The pyloric canal was occluded an estimated 300 degrees. The remainder of the stomach and duodenum were grossly and histologically normal. Histologic examination of the mass revealed it to be an adenocarcinoma. The distal antrum, pylorus, and proximal duodenum were resected, and the dog recovered uneventfully. This patient experienced an excellent quality of life. Upper GI endoscopy was performed at 6-month intervals to examine the stomach and proximal small intestine, and there were no gross or histologic abnormalities detected (Figure 1-11). There was also an exploratory laparotomy done at one point for removal of a cloth linear foreign body. This allowed a thorough examination of the abdominal cavity, and there was no evidence of recurrence of neoplasia. The dog lived 30 months beyond the diagnosis of gastric neoplasia, and there was never any recurrence of adenocarcinoma in the stomach region. Unfortunately, euthanasia was
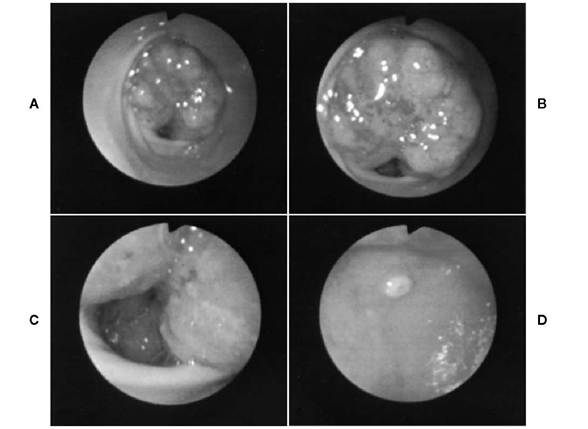
FIGURE 1-10 Endoscopic views of the stomach and proximal duodenum of a 9-year-old male Bouvier with a history of intermittent vomiting of 5 months' duration. A, The antral walls are normal.A proliferative mass is visualized in the pyloric orifice. B, Close-up view of the pyloric mass. The mass is occluding a majority of the pyloric orifice. The remaining orifice space is visualized at the six o'clock position. C, Pyloric canal near the pyloroduodenal junction. The mass extended into the proximal duodenum. The histologic diagnosis was adenocarcinoma. D, The major duodenal papilla is visualized in the upper center in the field of view.
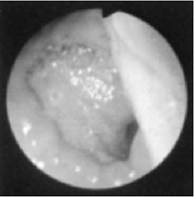
Figure 1-11 Six-month follow-up endoscopic view from the dog described in Figure 1-10. The anastomosis site between the proximal gastric antrum and the duodenum is in the field of view (note ridged area extending from five o’clock to twelve o’clock position). There was no gross or histologic evidence of tumor recurrence.
performed at 30 months because of prostatic adenocarcinoma.
These two case histories clearly demonstrate the value of timely diagnosis of potentially lifethreatening problems. Frequently dogs and cats with intermittent vomiting have much more minor problems; however, it is difficult to anticipate which are the patients that will have the more severe problems. One of the clinician’s most important roles is to advise and educate owners in a responsible manner. Shouldn’t we as clinicians at the very least make owners aware of the diagnostic capabilities that we have at our disposal today? There is no question that a majority of our canine and feline patients with GI symptoms have treatable disorders. The important point is that we diagnose the chronic and potentially serious disorders early enough to make a difference.
Summary
The cause of chronic vomiting can be determined in most dogs and cats, and early diagnosis is facilitated when a systematic diagnostic approach is followed. In my experience, once adverse food reactions, GI parasites, drug reactions, and metabolic causes have been ruled out, the most common causes of chronic vomiting encountered in practice are inflammatory disorders (gastritis, inflammatory b owel disease), gastric hyp omotility, obstructive disorders (foreign bodies, hypertrophy syndromes), and neoplasia. The most clinically useful (i.e., high yield of important information while being cost-effective) diagnostic procedures include hemogram and biochemical profile evaluation, thyroid and feline heartworm testing in cats, urinalysis, fecal examination, survey abdominal radiography, ultrasonography, and endoscopy.