Blood
Most of the functions of blood are included in the following list:
1. Distribution of nutrients absorbed from the digestive tract
2. Transport of oxygen from the lungs to cells throughout the body
3.
Transport of carbon dioxide from metabolizing cells to the lungs4. Transport of waste products from metabolizing cells to the kidneys for excretion
5. Transport of hormones from endocrine glands to target cells
6. Assistance in body temperature control by transporting heat from deeper structures to the surface of the body
7. Assistance in maintaining a constant pH of body fluids by providing chemical buffers
| Table 15-1. Representative Values for Selected Constituents of Typical Mammalian Plasma | ||
| Constituents | Units of Measurement | Typical Range |
| Sodium | mEq/L | 135-155 |
| Potassium | mEq/L | 3.0-5.5 |
| Chloride | mEq/L | 95-110 |
| Bicarbonate | mEq/L | 22-26 |
| Total protein | g/dL | 6-8 |
| Albumin | g/dL | 3-4 |
| Blood urea nitrogen | mg/dL | 10-25 |
| Creatinine | mg/dL | 1.0-1.5 |
| Glucose | mg/dL | 70-100 |
8. Assistance with the prevention of excessive loss of blood from injuries by providing proteins and other factors necessary for blood coagulation
9.
Assistance with the defense of the body against disease by providing antibodies, cells, and other factors of body defense (see Chapter 16)Blood consists of cells and other cell-like formed elements suspended in a fluid called plasma. Some of its functions are specific to individual cells; for example, erythrocytes are primarily responsible for the transport of oxygen. other functions, such as assisting with body defense, involve a variety of blood cells and other plasma components. Blood volume is the total amount of blood in an animal’s body, including formed elements and plasma. Typical values given as a percentage of body weight are 7-9%. Lean, muscular, athletic animals tend to have higher percentages than animals with more body fat. (Specific gravity is an index, or ratio, of the weight of a substance to the weight of an equal volume of water. A specific gravity greater than 1 means that an equal volume of the substance weighs more than water, at 1 gImL. Blood and plasma have slightly higher specific gravities than water, primarily because of the blood cells and proteins, but the slight difference is usually disregarded when estimating blood or plasma volumes based on body weight.)
A large number of plasma proteins are suspended in the plasma, and electrolytes (e.g., Na+, K+, and Cl-) and other substances (e.g., glucose and urea) are dissolved in the plasma. While there are some minor species differences (e.g., adult ruminants typically have slightly lower values for blood glucose than other mammals), the values in Table 15-1 are typical normal ranges for the major chemical constituents of mammalian plasma.
Plasma is a subdivision of a larger body fluid compartment known as extracellular fluid, or ECF (see Chapter 2). Interstitial fluid, fluid outside of cells but not within vessels, is the other subdivision of the ECF compartment. The primary difference between interstitial fluid and plasma is that plasma contains a much higher concentration of proteins that cannot easily diffuse through the walls of capillaries.
Formed Elements of Blood and Hematopoiesis
The formed elements of the blood include erythrocytes (red blood cells), leukocytes (white blood cells), and platelets. Because erythrocytes and platelets both lack nuclei, they are not typical cells (see Plate II).
Hematopoiesis is the formation and development of all formed elements of blood (erythrocytes, leukocytes, and platelets), and all of these have a common ancestor, pluripotent
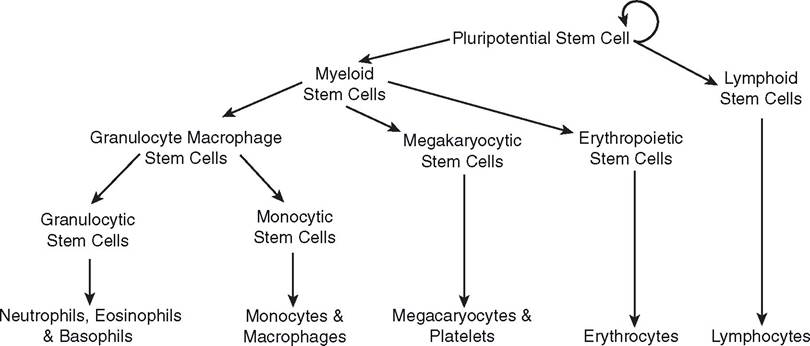
Figure 15-1. Summarized pathways to illustrate origin of blood cells and platelets.
stem cells (see Chapter 3 and Fig. 15-1). Pluripotent stem cells can replicate to provide more pluripotent stem cells or give rise to more differentiated stem cells that are committed to develop along one of two specific paths, myeloid and lymphoid. Figure 15-1 is an abbreviated family tree for blood cells and platelets, with the mature cells and platelets listed at the bottom of the maturation pathways. it is abbreviated in that several immature forms between the stem cells and the mature forms have been omitted. in theory, with enough time for an adequate number of cell divisions, a single pluripotent stem cell could repopulate a depleted bone marrow with additional pluripotent stem cells and give rise to mature erythrocytes, leukocytes, and platelets.
During early experimental studies on hematopoiesis, individual immature cells were isolated from bone marrow and maintained in cell culture. These studies demonstrated that in the right conditions, certain individual cells would form in vitro colonies that contained immature and mature cells of a specific cell line. The most undifferentiated cells that could form the cells of a specific lineage were termed colony-forming units (CFUs). More current literature uses the stem cell terminology; for example, a myeloid stem cell is equivalent to a colony-forming unit-granulocytic, erythrocytic, monocytic, and megakaryocytic (CFU-GEMM).
obviously, the proliferation and differentiation of bone marrow stem cells must be highly regulated. For example, the generation of erythrocytes should increase in response to blood loss after hemorrhage, while the generation of leukocytes should increase in response to an infection. A large variety of circulating chemical messengers have been found to regulate the proliferation and differentiation of bone marrow stem cells. The general term for such agents is hematopoietin. An individual hematopoietin may stimulate committed cells within development pathways to give rise to specific blood cells or may have a more general effect by stimulating less committed stem cells. For example, erythropoietin is the hematopoietin that stimulates a specific increase in erythrocyte production, and interleukin-2 stimulates increases in the production of several leukocytes. More information on individual hematopoietins is provided in later sections of this chapter and in Chapter 16. Based on the CFU terminology, hematopoietins have also been described as colony-stimulating factors.
Erythrocytes
Erythrocytes (from the Greek erythro-, red; -cyte, cell) range from about 5 to 7 μm in diameter. They are biconcave disks with a thick circular margin and a thin center (Fig. 15-2). The biconcave shape provides a relatively large surface area for gas exchange across the cell membrane. Erythrocytes have no nuclei and few organelles (Plate ii, Chapter 1). Total erythrocyte counts are expressed as number of cells per microliter of whole blood, and most domestic animals have about 7 million per microliter (Table 15-2). (Total leukocyte and platelet counts are also expressed per microliter of blood.)
The protein hemoglobin is the major intracellular constituent of erythrocytes. Hemoglobin is a complex molecule containing four
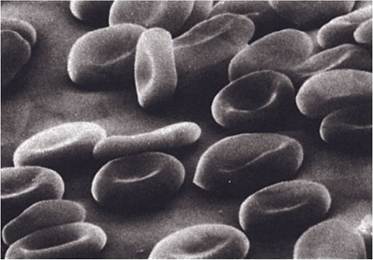
Figure 15-2. Red blood cells as seen by scanning electron microscopy.
(Reprinted with permission from Cohen B.J. and Wood D.L. MemmlerS The Human Body in Health and Disease. 9th ed. Philadelphia: Lippincott Williams & Wilkins, 2000.)amino acid chains (globin portion) held together by noncovalent interactions. Each amino acid chain contains a heme group (red porphyrin pigment), and each heme group contains an atom of iron. Hemoglobin concentration is measured in grams per 100 mL of blood, and typical values for normal hemoglobin concentrations range from about 11 to 13 gI100 mL in domestic mammals.
Hemoglobin functions in the transport of both oxygen and carbon dioxide. Oxygen binds to the ferrous iron in the heme group to form oxyhemoglobin (HbO2); this process is termed oxygenation (not oxidation). The amount of oxygen that can be bound is proportional to the amount of iron present, with one molecule of oxygen combining with each atom of iron. Because of the binding to hemoglobin, blood can contain about 60 times as much oxygen as would be dissolved in a similar quantity of water in the same conditions. Carbon dioxide also binds to hemoglobin at a different site on the molecule. Carbon dioxide binds to α-amino groups of peptide chains to form carbaminohemoglobin.
Binding of oxygen and carbon dioxide to hemoglobin is readily reversible. Blood arriving at the lungs from the peripheral circulation contains carbaminohemoglobin and is exposed to air with a relatively high concentration of oxygen and a relatively low concentration of carbon dioxide. in the lungs, carbon dioxide dissociates from carbaminohemoglobin, resulting in the formation of hemoglobin, which can bind oxygen to become oxyhemoglobin. When the blood containing oxyhemoglobin returns to the peripheral tissues that are relatively deficient in oxygen, the bound oxygen is released to the tissues. Carbon dioxide can then bind to hemoglobin to continue the cycle.
| Table 15-2. Representative Values for Blood Cell and Platelet Numbers per Microliter of Blood in Selected Domestic Animals | ||||
| Blood Element | Horse | Cow | Dog | Chicken |
| Erythrocytes | 8-11a | 6-8a | 6-8a | 2.5-3a |
| Total leukocytes | 8-11b | 7-10b | 9-12.5b | 20-30b |
| Neutrophils | 4-7b | 2-3.5b | bgcolor=white>6-8.5b5-10b | |
| Lymphocytes | 2.5-4b | 4.5-6.5b | 2-3.5b | 11-18b |
| Monocytes | 400-500 | 350-500 | 450-600 | 2-3b |
| Eosinophils | 200-500 | 150-500 | 200-500 | 600-2,000 |
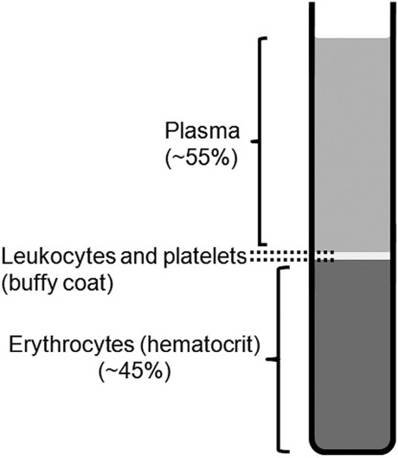
| Basophils | blood) results if either the number of functional erythrocytes or the quantity of hemoglobin per unit of blood is below normal. Anemia may be due to deficient blood formation, as with diseases of the bone marrow, kidney disease with inadequate production of erythropoietin, or poor nutrition, including dietary deficiency of iron, copper, vitamins, or amino acids. Anemia may also be caused by accelerated loss or destruction of erythrocytes, such as with hemorrhage or parasites. The hematocrit (packed cell volume) is the percentage by volume of whole blood that is erythrocytes. Routine hematocrit determinations require a glass tube treated to inhibit blood clotting (hematocrit tubes). Hematocrit tubes containing blood are centrifuged until the blood cells are packed in the lower end of the tube (Fig. 15-3). Hematocrits typically range from 35 to 45 for most mammalian species and are generally considered to be an indicator of the total erythrocyte count. Hemoconcentration is a decrease in the fluid component of blood with a resulting increase in the ratio of cells to fluid. it is indicated by an excessively high erythrocyte count (polycy-
Figure 15-3. Layering of blood components in an anticoagulated and centrifuged blood sample. themia) or a high hematocrit. Reductions in plasma volume may result from inadequate water intake or excessive loss of fluids from the body, such as with vomiting or diarrhea. Platelets Blood platelets, also called thrombocytes, are fragments of megakaryocytes, large cells formed and residing in the bone marrow. Thrombocytes are the smallest of the formed elements in the blood at 2-4 μm. They are surrounded by a plasma membrane and contain some organelles, but not nuclei. Thrombocytes range from 150,000 to 500,000 per microliter of blood in most mammalian species (Table 15-2). The appearance of platelets in a stained smear may be considerably different from their actual appearance in circulating blood, where they are oval disks. in smears they may appear as circular disks, star-shaped fragments, or clumps of irregular shape (Plate II, Chapter 1). Platelets reduce loss of blood from injured vessels. By adhering to vessel walls and to each other in the area of the injury, platelets may form a plug upon which a thrombus (clot) forms to occlude the opening in the vessel and prevent further blood loss. substances released by platelets and lodged on their surface membranes stimulate clotting and help cause local constriction of the injured blood vessel (described in more detail later in this chapter). Leukocytes Leukocytes (Plate II, Chapter 1) or white blood cells (from the Greek word leuco, white) differ considerably from erythrocytes in that they are nucleated and are capable of independent movement to exit blood vessels. Leukocytes may be classified as either granulocytes or agranulo- cytes based on the presence or absence of cytoplasmic granules that stain with common blood stains, such as Wright’s stain. These stains contain an acid dye, eosin, which is red, and a basic dye, methylene blue, which is bluish. Granulocytes are named according to the color of the stained granules (i.e., neutrophils, which have granules that stain indifferently; eosinophils; and basophils). The nuclei of granulocytes appear in many shapes and forms, leading to the name polymorphonuclear leukocytes (from the Greek poly, many; morpho, form). However, the term is commonly used to indicate neutrophils, because they are normally the most prevalent granulocyte. Monocytes and lymphocytes are the two types of agranulocytes. Neutrophils. Neutrophils, a first line of defense against infection, constitute a large percentage of the total leukocyte number (Table 15-2). upon tissue injury or microbial invasion, neutrophils rapidly accumulate within the interstitial fluids of the injured or invaded area. The active movement of neutrophils and other leukocytes out of intact blood vessels and into the interstitial fluid is diapedesis. Chemical messengers known as chemotactic factors attract neutrophils to these sites. Chemotactic factor is a general term for a variety of compounds that are capable of attracting neutrophils and in some cases other leukocytes. These factors may be produced by invading microorganisms, by leukocytes after interacting with microorganisms, or by damaged tissue. Neutrophils are phagocytes; they engulf invading bacteria to destroy them. The destruction involves the action of enzymes in the intracellular granules of the neutrophils and cell membrane-bound enzymes that are activated when phagocytic vesicles are completely formed. During phagocytosis, neutrophils may also release enzymes that contribute to the local inflammation. In the process of responding to the potential infection, many of the attracted neutrophils are destroyed. Pus, the semiliquid material that results from the collective responses to a microbial invasion, may contain neutrophils and cellular debris. An abscess is an accumulation of pus that has been isolated by the formation of surrounding connective tissue. Neutrophilia is an increase in the number of circulating neutrophils in the blood that occurs with bacterial infections. Circulating neutrophils can increase as a result of an immediate release of existing neutrophils from the bone marrow and an increase in neutrophil production. Neutropenia refers to an abnormally low number of circulating neutrophils. The word endings -philia and -penia can be combined with the root names of the other leukocytes to indicate similar conditions (e.g., eosinophilia is an increase in eosinophils). Eosinophils. Eosinophils contain red-staining cytoplasmic granules. Normally, eosinophils are less than 10% of total leukocytes (Table 15-2), but they may increase in number with allergic conditions and parasitism. Eosinophils are ameboid and somewhat phagocytic. Their primary function seems to be the regulation of allergic responses and tissue responses to parasites. They act by removing antigen-antibody complexes, which stimulate allergic responses, and by inhibiting some of the mediators of allergic responses, such as histamine. Basophils. Basophils contain blue-staining granules and are rarely seen in normal blood. The granules of basophils contain multiple compounds, including heparin, which prevents blood clotting, and histamine, which relaxes smooth muscle of blood vessels and constricts smooth muscle in airways. Cells that are very similar but distinct, mast cells, are found in many sites throughout the body but are especially prevalent in connective tissue below an epithelial lining exposed to the external environment (e.g., dermis, wall of airways, and wall of gastrointestinal tract). Basophils and mast cells release the contents of their granules during allergic responses, and these chemicals contribute to the characteristic tissue responses. The release of the granules is mediated in part by the binding of specific antibodies and the associated allergen (antigen). Monocytes. Monocytes are the largest of the circulating leukocytes. They are phagocytic and develop into even larger macrophages when they exit vessels and enter the tissues. Like neutrophils, monocytes are attracted by chemotactic factors to areas of tissue injury and microbial invasion. in addition to phagocytosis of tissue debris and microbes, macrophages have a major role in the overall initiation and regulation of inflammatory and immune responses. During their response to tissue injury or microbial invasion, macrophages release numerous chemical messengers that coordinate the function of other cells responding to injury or invasion. Macrophages also function in the processing of antigens, a necessary step in the initiation of an immune response. These functions are discussed in more detail in Chapter 16. Lymphocytes. In most species, lymphocytes are the second most prevalent circulating leukocyte after neutrophils, but they are more prevalent than neutrophils in ruminants (Table 15-2). Based on their functions, three general types or groups of lymphocytes have been identified (B lymphocytes, T lymphocytes, and NK, or natural killer cells), but these types cannot be identified by differences in appearance. In blood smears, lymphocytes vary in size, with a relatively large nucleus surrounded by a small amount of cytoplasm (Plate II, Chapter 1). Lymphocytes function in specific immune responses and immune surveillance, and these functions are discussed in Chapter 16. Differential White Blood Cell Counts. Differential counts indicate the percentage of each type of white cell in the blood sample (Table 15-2). The various types of leukocytes have different functions and respond differently to various types of infections or diseases, so differential counts can be useful for diagnosis. Differential counts taken over time can also be used to evaluate the response of an animal to infection or disease. A differential count is made by spreading a drop of whole blood thinly on a glass slide to form a blood smear. The smear is dried and stained with a blood stain, such as Wright’s stain. After staining is complete, the slide is examined with a microscope and the number of white cells of each kind is tabulated until a predetermined total number of white cells have been counted. The number counted is usually a multiple of 100, and the percentage of each leukocyte type observed in a given sample of blood is called the differential leukocyte count or differential white cell count. In reference laboratories, both total red and white cell counts are semiauto- matically determined by sophisticated laboratory equipment.
More on the topic Blood:
-
Veterinarian -
| |||