CAPILLARY DYNAMICS
1. Distinguish between diffusion and bulk flow.
2. What are the four pressures that are associated with bulk flow?
3. What contributes to plasma colloidal osmotic pressure?
4.
Consider each of the four pressures and determine the direction of fluid flow caused by each.5. Study the examples given for the arterial and venous ends of a capillary that determine the extent of filtration and reabsorption.
6. Study the examples of capillary imbalance and relate their causes to the pressure factors.
7. Why are venous side pressure increases more conducive to imbalance caused by increased capillary pressure than arterial side pressure increases?
The topic of capillary dynamics refers to the physical factors associated with the exchange of fluid between the blood and interstitial fluid at the level of the capillaries. The capillaries have slit-like spaces between adjacent endothelial cells that make up the capillary wall, known as intercellular clefts. Although water can diffuse through all parts of the endothelium (capillary membrane), it seems to diffuse more freely through the clefts, or pores. Lipid-soluble materials (e.g., oxygen, carbon dioxide) in blood diffuse freely through the lipid portion of the capillary membrane, but. lipid-insoluble substances (e.g., electrolytes, glucose, urea) must diffuse through the pores. Large lipid-insoluble molecules (e.g., protein) diffuse through the pores with difficulty.
Diffusion and Bulk Flow
The diffusion of water and its dissolved substances accounts for the greatest degree of interchange between capillaries and interstitial fluid (Figure Q-33). By the time blood traverses the distance of a capillary, the water of the plasma has been exchanged with water of the interstitial fluid about 80 times. Usually the relative proportions of the extracellular water between the plasma and interstitial space are in equilibrium.
In addition to diffusional flow of fluid, there is also a bulk flow; this results from osmotic and hydrostatic pressure differences between plasma and interstitial fluid. It should be noted, however, that the volume of interchange occurring by diffusion is many times greater than the volume of interchange by bulk flow. The volume of bulk flow into the interstitial space from the plasma is usually balanced by the amount returning to the capillaries from the interstitial space, coupled with that returning through the lymphatics. In certain circumstances imbalances occur and fluid can accumulate excessively in the interstitial spaces. In such cases, bulk flow into the interstitial space from the blood capillaries exceeds the volume returned to the blood capillaries by diffusion from the interstitial space and by lymph through lymphatic capillaries.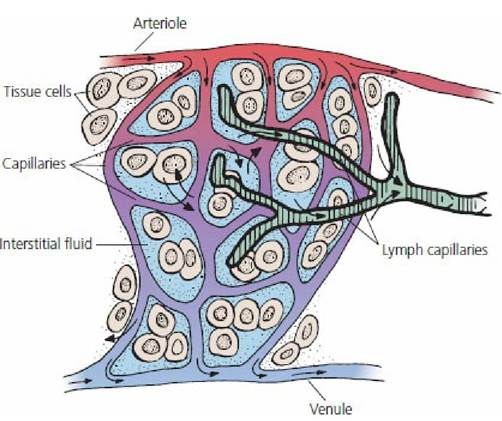
■ FIGURE 9-33 A schematic representation of a capillary bed. Blood is supplied to capillaries by arterioles and leaves the capillaries through the venules. Tissue cells are surrounded by interstitial fluid (ISF). Water and dissolved substances from blood capillaries are interchanged with ISF, intracellular fluid, and lymph capillaries by diffusion. ISF not returned to the blood capillaries is returned as lymph through lymphatic capillaries. Small arrowheads represent the direction of blood flow; large arrowheads represent the direction of diffusion.
Mechanism of Bulk Flow
The mechanism of bulk flow is determined by a number of parameters.
Capillary Pressure
The capillary pressure (Pc) is the hydrostatic pressure in the capillary. It averages 17 mm Hg (25 mm Hg at the arterial end and 10 mm Hg at the venous end).
Interstitial Fluid Pressure
The interstitial fluid pressure (Pif) is the hydrostatic pressure in the interstitial fluid. It averages about -6 mm Hg. It is a negative pressure (vacuum) and is created by the return of interstitial fluids to the venous end of the capillary and to the,lymphatics.
This can be compared with the attachment of a device to a water faucet to create a vacuum. When water flows through its open end, a vacuum is created at its side port.Plasma Colloidal Osmotic Pressure
The plasma colloidal osmotic pressure (πc) is the effective osmotic pressure of the plasma. It occurs because of the presence of the protein molecules and cations (positive ions) retained by the net negative charge of the protein. It can also be called the oncotic pressure. It averages about,28 mm Hg.
Interstitial Fluid Colloidal Osmotic Pressure
The interstitial fluid colloidal osmotic pressure (π⅛) is the effective osmotic pressure of the interstitial fluid and, like the πc, is a result of the presence of protein molecules that have leaked from the plasma and have not yet returned to the blood through the lymphatics. The ∏f averages about 5 mm Hg.
To understand bulk flow, it is helpful to consider these various pressures and to determine their effects, first at the arterial end of the capillary and then at the venous end. Normally, filtration or net outward flow occurs at the arterial end and reabsorption or net inward flow occurs at the venous end of the capillary.
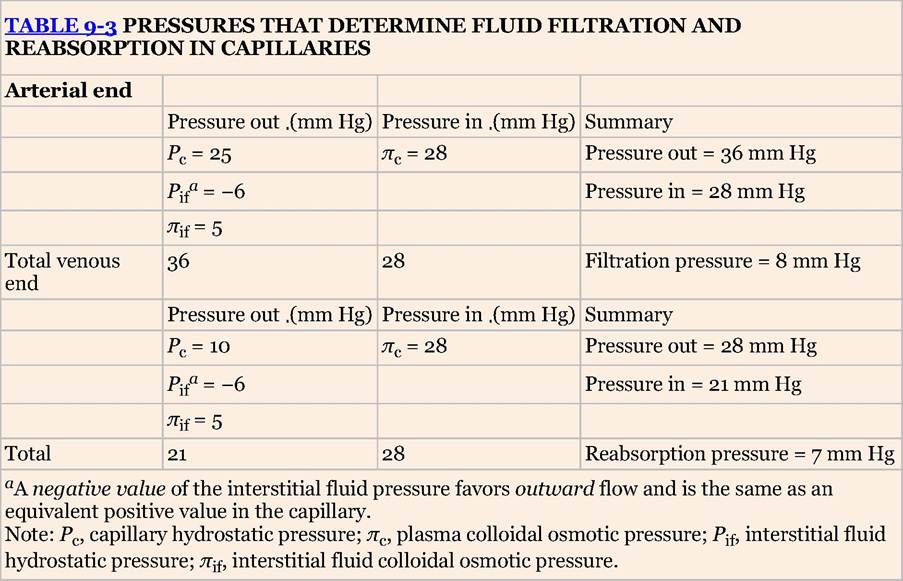
The arterial and venous ends of a capillary are shown in Figure 9-34. Each of the four pressures that influence the direction of fluid flow is shown with an arrow pointed in the direction of its influence. The effects of these four pressures are summarized in Table 9-3.
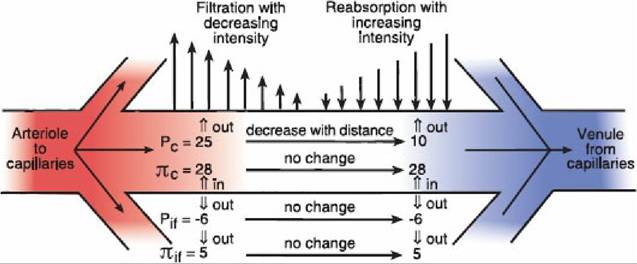
■ FIGURE 9-34 Physical factors associated with filtration at the arterial end and reabsorption at the venous end of a capillary. Values are in millimeters of mercury (mm Hg). Pc, capillary hydrostatic pressure; πc, plasma colloidal osmotic pressure; Pif, interstitial fluid hydrostatic pressure; π⅛, interstitial fluid colloidal osmotic pressure.
Open arrows indicate the direction of influence of Pc, πc, Pif, and πff.A filtration pressure of 8 mm Hg and reabsorption pressure of 7 mm Hg would seem to represent an imbalance (i.e., filtration exceeds reabsorption by 1 mm Hg), whereby fluid would accumulate in the interstitial fluid. Accumulation does not ordinarily occur, however, because the extra filtration represented by these values is removed from the interstitial fluid by the lymphatics. In fact, some of the interstitial fluid bulk flow must be removed by the lymphatics to carry the protein that has leaked from the capillaries back to the blood. Once again, the lymphatics are the only route by which leaked protein can return.
Capillary Imbalances
An imbalance of bulk flow can occur; when this happens, fluid accumulates in the interstitial space. This can be seen when high capillary pressure, low blood protein concentration, lymphatic blockage, and increased capillary porosity (which allows more protein to escape) are each sufficient to favor
filtration over absorption and lymphatic drainage. Increases in capillary hydrostatic pressure can arise from either the arterial or the venous end of the capillary. High arterial blood pressure (e.g., kidney retention of salt and water) is transmitted to capillaries and can influence capillary dynamics; however, increases of venous blood pressure are more conducive to imbalance caused by high capillary pressure than increases from the arterial side. Venous side increases transmit the increase throughout the length of the capillary, whereas the effect of an arterial side increase is minimized by its reduction in going from the arterial to the venous end. Some causes of increased venous pressures are heart failure, in which the weakened heart is unable to circulate all of the blood that is returned to it and venous blood pressure increases, venous obstruction (e.g., trauma, tight bandages), and venous pump failure (e.g., muscle paralysis, immobilized parts).
Lymphatic obstruction increases interstitial colloidal osmotic pressure because protein, ordinarily returned by lymphatic vessels, is retained in the interstitial fluid, thereby reducing the potential for fluid reabsorption. The failed reabsorption, in turn, causes an increase in interstitial fluid hydrostatic pressure (from its negative value to positive), thereby contributing to increased capillary hydrostatic pressure throughout the capillary, which decreases the potential for reabsorption at the venous end. Some causes of lymphatic obstruction are blockage of lymph nodes (e.g., cancer, infection), destruction of lymph vessels (e.g., surgery, trauma), and blockage of lymph vessels (e.g., obstructive devices, tumors).
A reduction of plasma protein concentration that is low enough causes an imbalance because plasma colloidal osmotic pressure, the reabsorption factor, is decreased to the point at which filtration exceeds reabsorption. Some causes of plasma protein depletion are renal disease (e.g., loss of protein in urine), reduced protein synthesis (e.g., liver disease, nutritional), and interstitial fluid loss (e.g., denuded skin).
Capillary injury by trauma or by toxins increases the porosity of the endothelial cells and protein is lost from the capillaries, which reduces the potential for reabsorption.
In each of these examples, fluid accumulates in the interstitial space and gives it a swollen appearance, a condition known as edema. When it is generalized, it is referred to as anasarca.
■