BLOOD FLOW
1. How is blood flow to body parts autoregulated?
2. What changes occur related to cardiac output and blood flow diversion when muscular activity increases from the resting state to extreme activity?
3.
Study “Breathing and Blood Flow” very well. Visualize the expansion of the venae cavae that occurs with each inspiration. Translate expansion of the venae cavae to increased blood flow to the heart.4. What is the difference between circulation time and mixing time?
There must be a difference in blood pressure between intake and output for blood to flow. Blood pressure alone does not imply blood flow. The flow of blood to a body part can be changed by changing the diameter of the vessel supplying the part. Constriction of a vessel reduces the blood flow and dilatation increases the blood flow.
Autoregulation
Generally, there is an autoregulatory mechanism affecting blood flow to a body part that is controlled by the amount of oxygen being received by the cells. When the oxygen is reduced in concentration, the blood vessels dilate and more blood is permitted to flow so that oxygen is replenished. It is also believed that more oxygen being supplied than is needed results in vasoconstriction, which would reduce blood flow and reestablish oxygen at its lower level.
Cardiac Output and Blood Diversion
Cardiac output is defined as the amount of blood pumped by the heart in a unit period of time. It is usually measured in milliliters or liters per minute. Under resting conditions, each body organ or muscle mass receives a rather constant amount. The percentage of the cardiac output that goes to the various organs or tissues changes, however, with the activity condition. At rest the muscles might receive only 20% to 25% of the cardiac output, whereas they might receive up to 75% during extreme muscular exertion. At such times there is diversion of blood flow from other organs (e.g., kidneys, intestines) so that it can be used by the muscle.
This is accomplished by constriction of the arteries and arterioles supplying the kidneys and intestines and by dilatation of the vessels supplying the muscles. During muscle exertion, the cardiac output is also increased; coupled with vasodilatation, this provides adequate blood flow to the muscle to satisfy the greater oxygen needs of muscle activity (Figure Q-30).
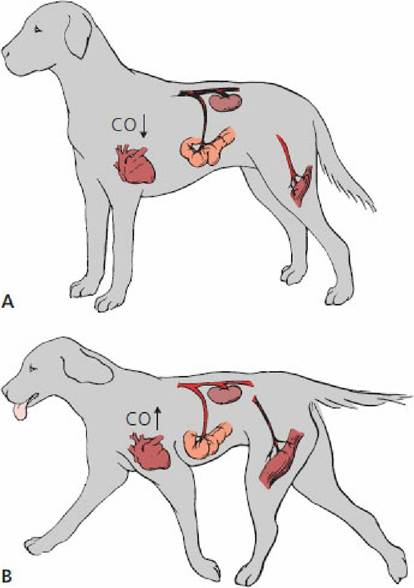
■ FIGURE 9-30 Diversion of blood flow according to need. Greater blood flow to kidneys and intestine at rest (A) and to muscles during exertion (B). Cardiac output (CO) is greater during exertion. Blackened vessels indicate locations of greater blood flow.
Breathing and Blood Flow3
An assist to blood flow is provided during the inspiratory phase of breathing. The venae cavae course through the thorax on their way to the right atrium. More specifically, they course through the mediastinum, a space shared by the other major blood vessels, the large lymph vessels, heart, and esophagus (Figure Q-31). The mediastinal space is intimately associated with the intrapleural space, a space that is in the thorax but outside the lungs. During inspiration, the thorax enlarges and a vacuum (negative pressure) develops in the intrapleural space. This vacuum provides for lung expansion. The negative pressure in the intrapleural space is also transferred to the mediastinal space because of the thin wall of separation. Any thin-walled structure within the mediastinal space responds to the developing vacuum by expansion, with the result being lowered pressure within the thin-walled structures (venae cavae, lymph vessels, and esophagus). This is helpful for the return of venous blood and lymph to the heart because it increases the pressure gradient to assist blood and lymph flow with every breath.

.Go to www.wiley.com/go/reece/functional to view a related video.
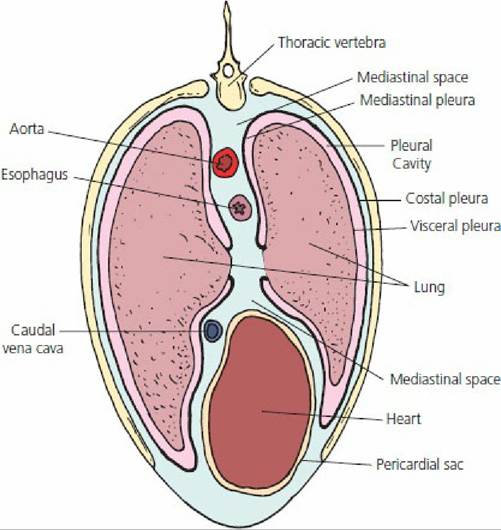
■ FIGURE 9-31 Cross-section of equine thorax at a level that shows the esophagus, caudal vena cava, aorta, and heart within the mediastinal space. Expansion of thoracic volume occurs with inspiration, which leads to lowering of pressure in the mediastinal space. This is followed by expansion of volume (and lowering of pressure) in thin-walled structures (e.g., lymphatics, venae cavae, esophagus) within the mediastinal space.
The above sequence of events is illustrated in Figure Q-32. In this laboratory model, the muscular diaphragm is represented by a rubber glove stretched over the bottom of a bell jar. Downward traction on the glove simulates contraction of the diaphragm. The lung and caudal vena cava are represented by balloons that respond to decreasing and increasing external pressure by expansion and collapse, respectively. During inspiration the diaphragm contracts; this is followed, in order, by: (1) increased thoracic volume, (2) decreased intrapleural pressure, (3) increased volume in the lung and vena cava, (4) decreased intrapulmonic and intravenous pressures, and (5) air flow into the lung and blood flow into the thoracic part of the vena cava. During expiration the diaphragm returns to its original position, so that: (1) the volume decreases in the thorax, lung, and vena cava and (2) the intrapleural, intrapulmonic, and intravenous pressures increase. Backflow of blood is prevented by valves in the vena cava, and air flows out of the lung.
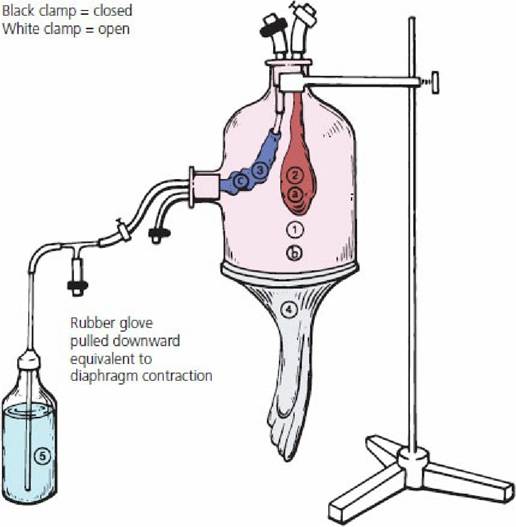
■ FIGURE 9-32 Laboratory model of the thorax. This illustrates the mechanics of breathing and the influence of breathing on venous blood return to the heart. Structures: 1, thorax; 2, lung; 3, vena cava; 4, diaphragm; 5, venous blood reservoir. Pressures: a, intrapulmonic; b, intrapleural; c, intravenous.
During inspiration, the diaphragm (4) contracts (downward pull of glove), resulting in an increase in thoracic volume (1) and a decrease in intrapleural pressure (b). This is followed by an increase in lung volume (2) and a decrease in intrapulmonic pressure (a). Air flows into the lung. Also, there is an increase in vena cava volume (3), simultaneous with lung volume increase, and a decrease of its intravenous pressure (c). Blood flow (5) to the heart increases because of intravenous pressure decrease. During expiration the diaphragm (4) relaxes, resulting in a decrease in the volumes of the thorax (1), lung (2), and vena cava (3), and an increase in intrapleural (a), intravenous (b), and intrapulmonic (c) pressures. Air flows out of the lung. Valves in veins prevent blood from flowing backward.Circulation Time
Circulation time refers to the time required for blood to return to the right atrium after it has been pumped from the left ventricle. This is variable but is approximately 40 to 60 seconds. Circulation time is distinct from mixing time, which is the time required for a substance injected into the blood to be mixed thoroughly, with either the blood or the body fluid compartment with which it is compatible. In all cases, the mixing time exceeds the circulation time.