Cardiac Tachyarrhythmias Result Either from Abnormal Action Potential Formation (by the Sinoatrial Node or Ectopic Pacemakers) or from Abnormal Action Potential Conduction ("Reentry")
Tachyarrhythmias are arrhythmias in which the atrial rate or the ventricular rate (or both) is abnormally high. An occasional extra atrial or ventricular beat is called a precontraction or a premature beat.
Occasional precontractions are common both in animals and in humans and usually have no clinical significance. If the precontractions become frequent or continuous, the condition is called tachycardia, which means “rapid heart.” Iachycardia is a clinically significant sign. The tachyarrhythmias result from abnormal pacemaker activity. The pacemaker initiating the rapid or “extra” beats can be the SA node itself. Alternatively, a region of abnormal cardiac muscle outside (he SA node can act as a pacemaker by spontaneously depolarizing to threshold before the regular SA node pacemaker does. Any such region is called an ectopic pacemaker. Common causes of ectopic pacemaker activity include cardiac infection or trauma, reaction to a drug or toxin, electrolyte imbalances, myocardial ischemia, and myocardial infarction.Tachycardia is a heart rate that is more rapid than is appropriate for the behavioral circumstances (e.g., 160 beats/ min in a resting dog). The tachycardias are named for the site of the pacemaker at which they originate. If the tachycardia appears to originate from the SA node pacemaker cells, the condition is called sinus tachycardia. If the tachycardia originates from an ectopic pacemaker within the atria, it is called atrial tachycardia. Atrial tachycardia is common in some canine breeds, including boxers and wolfhounds. Junctional tachycardias originate from ectopic pacemakers within the AV node or first part of the AV bundle. Supraventricular tachycardia is a collective term that encompasses sinus tachycardia, atrial tachycardia, and junctional tachycardia. If the ectopic pacemaker causing tachycardia is within the ventricles, the condition is called ventricular tachycardia.
In this situation the ventricles beat at a rapid rate, as dictated by the ectopic ventricular pacemaker. In occasional patients, some of the action potentials initiated by an ectopic ventricular pacemaker may be conducted backward through the AV node and may cause atrial precontractions. Usually, however, the AV node does not conduct action potentials backward; the atria continue to beat al the rale dictated by the normal SA node pacemaker. In either case, ventricular contractions are not preceded in the normal way by atrial contractions. The major dysfunction associated with ventricular tachycardia is that the ventricles do not relax long enough between contractions for adequate filling, and this problem is exacerbated by the absence of appropriately timed atrial contractions.An extremely rapid atrial tachycardia is called atrial flutter. Atrial flutter does not lead to ventricular flutter because of the long refractory period of the AV node cells; the AV node
conducts some, but not all, of the frequent atrial depolarizations to the ventricles. This is an example of the AV node protecting the ventricles from beating at too rapid a rate. If atrial contractions become so rapid that they lose synchrony, the condition is called atrial fibrillation. Atrial fibrillation is characterized by the continuous, random passage of action potentials through the atria. Fibrillating atria appear to quiver; there is no effective, coordinated contraction, and no blood is pumped. Atrial fibrillation is common in horses and in certain breeds of dogs, including Dobermans. Atrial fibrillation usually does not lead to ventricular fibrillation because of the protective effect of the AV node. The ventricles continue to contract with a synchronized, effective pumping stroke, at a rate that is limited by the refractory period of the AV node.
Synchronous ventricular contractions are essential for life. If the synchrony of ventricular contractions is disrupted and the ventricles begin to fibrillate, ventricular pumping stops.
In ventricular fibrillation, each tiny region of the ventricular wall contracts and relaxes at random, in response to action potentials that propagate randomly and continuously throughout the ventricles. The condition of ventricular fibrillation (“V- fib”) is synonymous with sudden cardiac death.In most cases, ventricular fibrillation can be reversed only by electrical defibrillation. In this process a strong electrical current is passed briefly through the heart muscle. This current depolarizes all the cardiac cells simultaneously and holds them in a depolarized state for several milliseconds. It is hoped that when the current is turned off, all the cardiac muscle cells will simultaneously repolarize to a resting membrane potential, so that the normal pacemaker of the heart will have a chance to initiate beats in an organized and synchronized manner once again. Sometimes it works; however, if the cardiac problems that caused ventricular fibrillation to develop in the first place are still present, fibrillation is likely to recur. Usually, defibrillation is performed by placing stimulating electrodes (“paddles”) on either side of the thorax. Therefore the stimulating current passes through, and depolarizes, the skeletal muscles of the thorax as well as the cardiac muscle of the heart. The resulting, involuntary contraction of the skeletal muscles causes the patient to “ jump” at the moment of defibrillation.
Ectopic pacemaker activity typically arises when a region of cardiac muscle develops the abnormal, twin properties of slow conduction of action potentials and an ability to conduct action potentials in Onlyonedirection. Figure 19-11 illustrates how a region of slow, one-way conduction in the wall of one cardiac chamber can initiate tachycardia. The process begins with a normally originating action potential being conducted in only one direction through the abnormal region of cardiac muscle. If the conduction through the abnormal muscle is so slow that all the normal muscle is past its refractory period by the time the action potential emerges from the abnormal region, the emerging action potential can trigger another action potential in the normal muscle.
If this second action potential then propagates around the cardiac chamber and back into the abnormal region, a self-perpetuating cycle can develop. The action potential once again propagates slowly through the abnormal region, and once again it emerges from the abnormal region after the normal muscle is past its refractory period. The result is a sequence of reentrant action potentials that propagate through the normal cardiac muscle, each one initiating a contraction—an “extra” beat. The reentrant pathway does not necessarily have to be all the way around the circumference of a cardiac chamber. An ischemic or infarcted area of cardiac muscle can form the nonconducting center around which reentrant action potentials can travel. This passage of an action potential around and around a nonconducting center is called a circus movement. In order for the circus movement of the action potential to be self-regenerating, however, a portion of the circular, conducting pathway must have the twin properties of slow and oneway conduction. In effect, an area of slow, one-way conduction within a circular conducting pathway (and around a nonconducting center) functions as an ectopic pacemaker. Reentry of cardiac action potentials can lead to occasional precontractions, continuous tachycardia, or even fibrillation. In any of these cases, the resulting tachyarrhythmia is called a reentrant arrhythmia.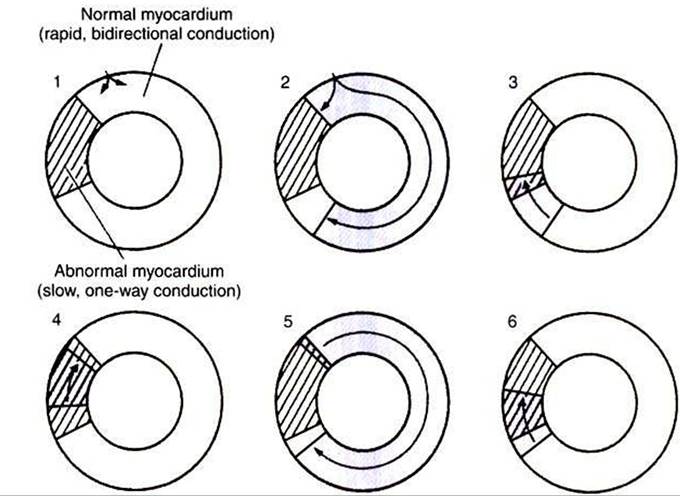
FIGURE 19-11 Cross section of a cardiac chamber (atrium or ventricle) is pictured at six different instants to illustrate how reentrant arrhythmias occur.The region of abnormal myocardium (cross-hatched area) conducts action potentials slowly and only in one direction (clockwise in this example), 1, Normal action potential has just entered this ring of tissue, and only the gray-shaded area is depolarized. 2, Action potential propagates rapidly in both directions through the normal cardiac tissue but is blocked from entering the abnormal myocardium in a counterclockwise direction. 3,The clockwise-going action potential can enter the abnormal region. 4z While the action potential propagates slowly, in a clockwise direction through the abnormal region, the normal cardiac tissue repolarizes to a resting state. 5z Action potential emerges from the abnormal region into normal cardiac tissue and propagates through the normal tissue for a second time. Meanwhile, the abnormal tissue repolarizes to a resting state. 6, Action potential begins to move slowly through the abnormal region for a second time. States 4, 5, and 6 repeat themselves. Thus the abnormal region functions as an ectopic pacemaker.