Clinical dysfunction
Disturbance of the vestibular system produces a series of characteristic signs that reflect derangement of the functions described in the preceding section. Lesions may be located in the inner ear (semicircular canals, utriculus or sacculus) the vestibular portion of CN VIII, the vestibular nuclei, the caudal cerebellar peduncle, the vestibulocerebellum or, potentially, the cranial cervical spinal cord.
The key point to understanding vestibular dysfunction is to recall that during normal function, the brain interprets unmatched input from the vestibular apparatus as indicating head movement. This unbalanced input will then induce changes in postural muscle tone, eyeball position and movement. If the normal animal moves its head to the left as in Fig. 8.4, there will be increased input from the left horizontal canal and decreased input from the right horizontal canal. This causes increased extension in the limb, trunk and neck muscles on the animal’s left side and decreased extension on the right side. The animal’s eyes will jerk in a rapid fashion to the left. The adjustments of limb position and head position will be coordinated by the cerebellum.If the animal had a lesion in the right side of the vestibular system then the vestibular nuclei would have decreased input from the right but sustained input from the left, that is, unbalanced input with left side input being greater than the right. In this diseased animal, the unbalanced input occurs when the animal is at rest, not moving as described in the preceding paragraph for the normal animal. The brain would interpret the unbalanced input as indicating that the head is turning to the left. At rest, the animal would have increased anti-gravity extensor tone on the left, and decreased muscle tone on the right side. Thus the animal with a right-sided vestibular lesion would have decreased tone in the right-sided postural muscles compared with the left.
This would present as decreased neck muscle tone on the right resulting in a head tilt to the right. There would be excess extensor tone on the left side of the body and decreased extensor tone on the right, thereby pushing the animal to the right. Thus the animal would tilt, stagger, drift, circle or, in severe cases, roll to the right (Figs. 8.8 and 8.9).
Fig. 8.8 Rabbit with right-sided peripheral vestibular disease resulting in ipsilateral head tilt and loss of extensor muscle tone in the neck and body. See also Fig. 1.14.
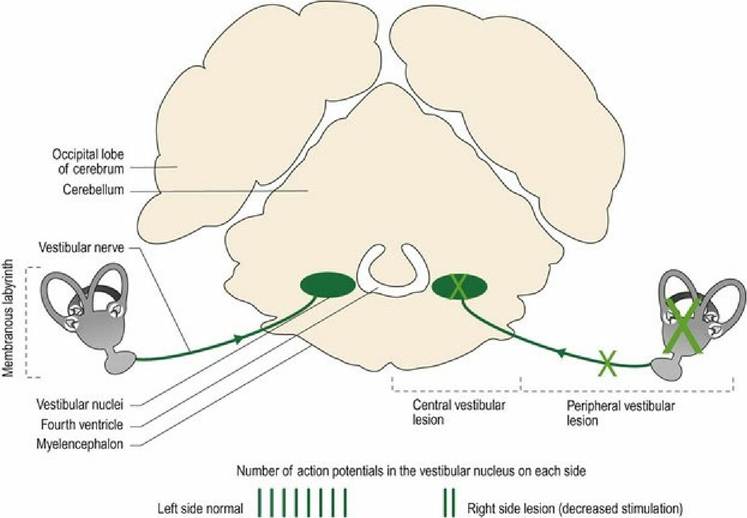
Fig. 8.9 Ihe caudal brainstem in transverse section, showing the sites of peripheral and central vestibular system lesions (green crosses) and their effect on vestibular stimulation when the head is in a resting, neutral position (see Figs. A21-23).
The animal tries to compensate for the altered posture but due to abnormal output from the vestibular nuclei to the cerebellum (subconscious proprioception of the head), coordination of limb position and stepping movements would be perturbed. Thus the animal would be ataxic with wide- or narrow-based postures and uncoordinated movement.
The brain perceives the animal to be turning to the left due to the unbalanced input, thus at rest, the eyes make rapid jerky movements to the left, before drifting back across the orbit again. This abnormal movement of the eyeballs is called pathological nystagmus and may occur in the horizontal, vertical or rotatory direction, depending on which semicircular canal inputs (x, y or z direction) have been disturbed by the lesion. Acutely affected dogs may appear nauseous or vomit (motion sickness) due to unbalanced input to the reticular formation.
Location of lesion and clinical signs
Classical vestibular signs include head tilt, staggering and ataxia, circling and nystagmus.
They may arise from lesions in the periphery in the inner ear or the vestibular portion of the vestibulocochlear nerve (CN VIII). Or they may arise centrally in the brainstem, the vestibular portions of the cerebellum or the cranial spinal cord (Fig. 8.9). Thus vestibular disease is called peripheral or central, respectively.Differentiating the location of the lesion is important for diagnosis and prognosis. Lesion localisation follows the golden rule of identifying which other neural functions are compromised and which neural functions are normal (see Fig. 13.1).
Any lesion in the nervous system, peripheral or central, may also compromise nearby structures. A disease causing peripheral vestibular lesions in the inner ear may also affect the facial nerve running beside the middle ear. In small animals, but not in large animals, the sympathetic supply to the face passes adjacent to the middle ear and can also be compromised. Respectively, this collateral damage can cause ipsilateral facial paresis and Horner’s syndrome (miosis, ptosis, enophthalmos and protrusion of the third eyelid (see Fig. 12.6)) or changes in ipsilateral sweating. Lesions affecting the site of attachment of CN V, VII and VIII to the rostral medulla oblongata can result in signs of masticatory muscle atrophy as well as facial hypoalgesia, paresis and vestibular signs.
Lesions affecting the vestibular nuclei (central disease) are highly likely to also affect nearby brainstem tracts and structures. These include adjacent proprioceptive pathways, UMN nuclei, sensory input from the head (CN V), facial nucleus (CN VII) and the ascending reticular activating system (ARAS) (Chapter 11). Thus central vestibular lesions may also cause ataxia, due to general and vestibular proprioceptive deficits, UMN paresis, facial hypoalgesia and paresis, and decreased awareness, respectively. The second dog in Fig. 10.12 (B and C) presented initially with CN V signs and subsequently developed facial paresis (CN VII), head tilt and nystagmus (CN VIII).
The presence of these clinical signs indicates that the lesion is likely to be where CNV, VII and VIII attach to the brainstem.Vestibular signs can also occur with lesions affecting the vestibulocerebellum. If the lesion in the cerebellum is quite extensive it may be accompanied by other signs of cerebellar disease (tremor, spasticity, dysmetria, see Chapter 7) but the animal will not be paretic (as the UMN nuclei are not involved). It will be bright, alert and responsive (no involvement of the ARAS) and will not have other CNN deficits (CN V and VII) or Horner’s syndrome.
Rarely, lesions in C1-3 spinal cord segments may affect the proprioceptive input from the muscles such as the obliquus and rectus capitis, and result in vestibular-like signs. Nystagmus may be observed with such lesions.
Paradoxical vestibular disease
Lesions may also occur in the area of the caudal cerebellar peduncle, which conveys the afferent subconscious proprioceptive fibres going to the cerebellum tracts and the efferent fibres from the vestibulocerebellum (flocculonodular lobe) to the brainstem. Lesions affecting the caudal cerebellar peduncle produce paradoxical vestibular signs. The signs are paradoxical because they seem to indicate that the lesion is on the contralateral side of the CNS. Note: the occurrence of paradoxical vestibular disease is far less common.
In typical vestibular disease (peripheral or central) the head tilt and circling will be towards the side of the lesion, while the fast phase of pathological nystagmus will be away from the side of the lesion (e.g. rightsided lesion, will result in a head tilt to the right and the fast phase of nystagmus to the left). In paradoxical vestibular disease, the head tilt and circling is to the opposite side of the lesion and the fast phase of the nystagmus is towards the side of the lesion.
The explanation for this rests in the primary concept that the output from the vestibulocerebellum is direct (not via the deep cerebellar nuclei) and hence, is inhibitory to the vestibular nuclei.
Thus on the side with the lesion, there will be decreased inhibition to the vestibular nuclei. These nuclei will have more activity than the vestibular nuclei on the normal side. The brain perceives from this unbalanced input that the animal must be turning to the side of the lesion (Fig. 8.10).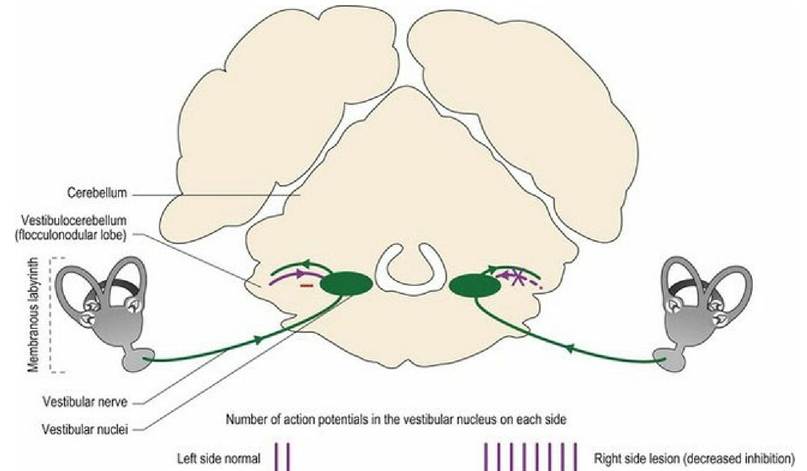
Fig. 8.10 Mechanism of paradoxical vestibular disease.
For example, if the right-side caudal cerebellar peduncle is damaged, as by a tumour or inflammatory mass, there will be decreased cerebellar cortical inhibition of the ipsilateral vestibular nuclei. Therefore, there will be increased activity of the vestibular nuclei on the right side. The uneven activity in the left- and rightside nuclei will be interpreted as the animal turning to the right. There will be increased reflex output down the right-side vestibulospinal tract, thus the right side extends while left-sided extension is inhibited. The animal tilts, staggers and drifts to the left (contralateral to the side of the lesion). At the same time, the apparent perception of turning to the right means that the eyeballs flick rapidly to the right as they would if the animal was truly turning to the right.
Identifying that the lesion is causing paradoxical signs involves identifying what other neural functions are compromised. Many proprioceptive fibres from the limbs and body (spinocerebellar tracts) travel via the caudal cerebellar peduncle into the cerebellum, thus such lesions can also compromise ipsilateral proprioception. In the example above the animal would have right-sided proprioceptive deficits. Due to the proximity of brainstem UMN nuclei, such lesions may also cause ipsilateral paresis.