Concentration and Dilution of Urine: Role of Loop of Henle and Collecting Duct Transport
To maintain water balance during potentially drastic changes in water intake, the kidneys must be able to excrete urine that is either more concentrated than plasma (hypertonic) or more dilute than plasma (hypotonic).
The ability of the kidneys to generate hypertonic or hypotonic urine depends on the functional and anatomic characteristics of both the loop of Henle and the collecting duct. The excretion of hypertonic urine also requires antidiuretic hormone (ADH, or arginine vasopressin) to alter the transport characteristics of the collecting duct.Sodium Chloride and Water Reabsorption by the Loop of Henle
Loops of Henle are the nephron segments found in the renal medulla. The U-shaped loops extend to variable depths in the medulla, and the terms descending and ascending limbs are applied to the different parts of the loops (Fig. 23-4).
The ascending limbs of the loops of Henle are relatively impermeable to water and have a thick portion that is the site of a great deal of sodium and chloride reabsorption. sodium and chloride transport by the thick ascending limb uses a unique membrane transporter that cotransports sodium, chloride, and potassium into the cell from the lumen. This transport is sodium-linked in that the Na-K-ATPase pump on the opposite side of the cell maintains the low intracellular sodium concentration that permits the cotransporter to function. The net effect of this cellular transport is continuous addition of sodium and chloride to the interstitial fluid of the medulla without any accompanying water (Fig. 23-11). Sodium chloride is also reabsorbed from the thin ascending limb of the loop (Fig. 23-11), but the mechanism responsible for this transport is controversial. The fluid entering the loop of Henle is isotonic, and the fluid exiting is hypotonic (Fig. 23-11). This change in tubular fluid shows that the net effect of loop of Henle transport is to add more particles than water to the interstitial fluids in the renal medulla.
Transport of sodium and chloride into the interstitium without water is the key factor in generation of hypertonic interstitial fluid in the medulla (Fig. 23-11), and this hypertonic fluid has an essential role in the ability to generate hypertonic urine. The transport of particles without water from the lumen of the loops also creates hypotonic fluid in the tubule, and this is an essential step in the ability to generate hypotonic urine. However, regardless of the tonicity of the final urine, the transport characteristics of the thick ascending limbs of the loops of Henle remain the same, so that hypertonic fluid is generated within the renal medulla and hypotonic fluid is generated within the loop of Henle.
The descending limbs of the loops of Henle are relatively permeable to water but relatively impermeable to particles. As fluid flows into and through the descending limbs, water is removed because of the osmotic gradient between the tubular lumen and the interstitial fluids of the renal medulla (Fig. 23-11).
Because the ascending and descending limbs of the loops of Henle are relatively close together in the medulla and because the tubular flows move in opposite directions, the combined effect of transport by ascending and descending limbs produces an osmotic gradient in the interstitial fluids of the renal medulla. interstitial fluid osmolality increases from the outer zones to the inner zones of the renal medulla (Fig. 23-11).
The countercurrent mechanism is any mechanism that depends on streams of flow moving in opposite directions, and these are usually close to each other. The ascending and descending loops of Henle form a countercurrent mechanism that amplifies the osmolyte (sodium chloride) transport properties of the ascending limb of the loop of Henle. This countercurrent mechanism generates the osmotic gradient in the interstitial fluids of the renal medulla.
The ascending and descending vasa recta also form a countercurrent exchange mechanism by permitting free exchange of solutes and water between the ascending and descending blood vessels.
This exchange allows for blood flow into and out of the medulla without disrupting the gradient. There is a small net gain of both water and particles by the vasa rectae, and some of these are the water and particles that were reabsorbed from the loop of Henle (Fig. 23-11).The maximal osmolality of the osmotic gradient in the renal medulla differs among species, and maximal urine concentration ability is determined by the maximal osmolality of the gradient (Fig. 23-11).
Collecting Duct Transport and Antidiuretic Hormone
Principal cells in the collecting ducts are the target cells for ADH. if ADH is not present, the luminal cell membrane of these cells is relatively water impermeable. ADH stimulates the insertion of water channels into these cell membranes to increase the overall water permeability of collecting ducts.
Collecting ducts begin in the renal cortex but extend into and through the renal medulla, where the interstitial fluids are hypertonic.
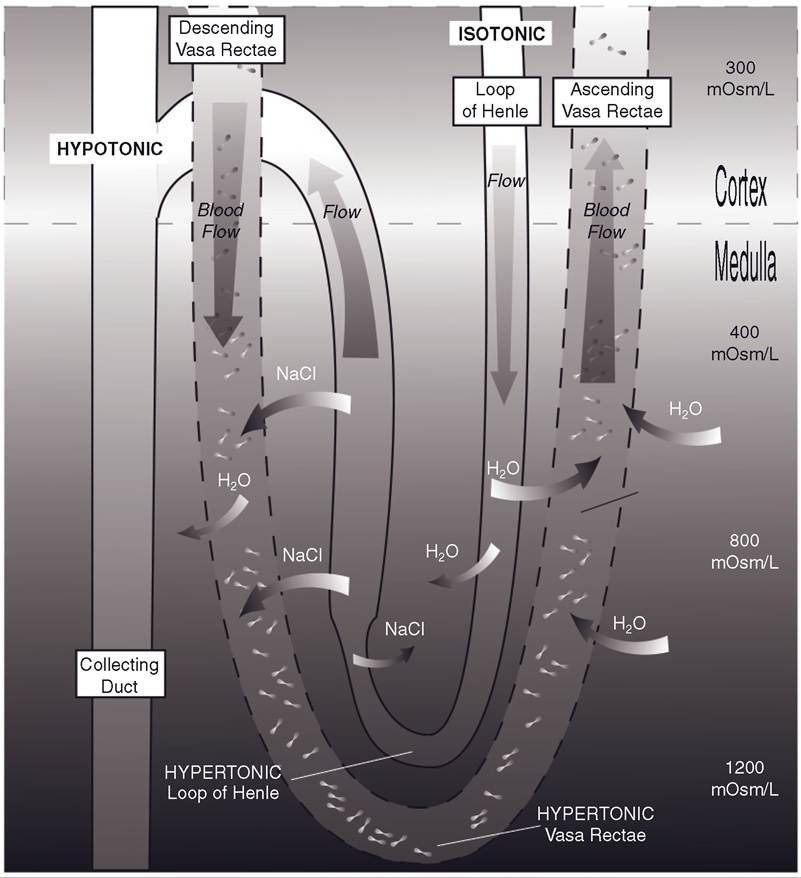
Figure 23-11. Transport of sodium chloride and water by loop of Henle and vasa rectae. Arrows indicate direction of net transport in the different tubular segments and vessels. The osmolarity of the interstitial fluids in the cortex is 300 mOsm/L; the osmolarity of the interstitial fluids in the medulla is shown as a gradient that increases from outer to inner medulla. Hypertonic, isotonic, and hypotonic refer to fluid and plasma in tubules and vessels, respectively.
Also, because of the transport in the loop of Henle, the tubular fluid entering the cortical portion of a collecting duct is dilute or hypotonic, and this is always true regardless of the water balance status of the animal. if ADH is not present, the water permeability of the collecting duct is relatively low, and the hypotonic fluid entering the collecting ducts passes through and is excreted as a hypotonic urine. Because water is not reabsorbed from the
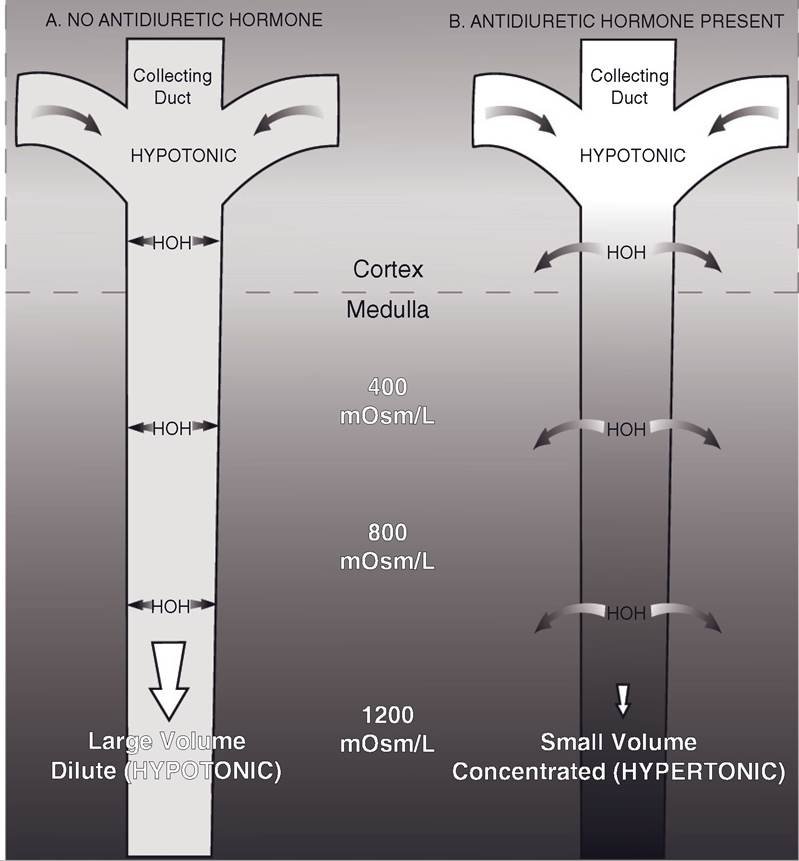
Figure 23-12.
A) Distal tubule and collecting duct when ADH is absent. Water permeability of collecting is low, so tubular fluid remains hypotonic (dilute). B) Distal tubule and collecting duct when ADH is present. Water permeability of collecting duct is increased, so water is reabsorbed and tubular fluid becomes hypertonic (concentrated).water-impermeable collecting duct, the volume is also relatively large (Fig. 23-12A). If ADH is present, the water permeability of the collecting duct is increased, and water is reabsorbed because the osmolality inside the duct is less than that outside. As the tubular fluid passes through the medullary portion of the collecting duct, more and more water is reabsorbed, and the osmolality of the tubular fluid increases further. in these circumstances urine volume is low and urine osmolality is high (Fig. 23-12B).
Osmotic Regulation of Antidiuretic Hormone
ADH (or arginine vasopressin in most mammalian species) release from the posterior pituitary can be regulated by changes in the ECF (extracellular fluid) osmolality. Specific cells (osmoreceptors) in the hypothalamus monitor the osmolality of ECF. in response to increases in ECF osmolality, these cells stimulate increases in ADH release, which results in the excretion of a small volume of a hypertonic urine. The elimination of excess particles and conservation of water dilutes the ECF, which acts as a negative feedback control to inhibit additional releases of ADH. Reductions in ECF osmolality inhibit ADH release, which results in the excretion of a relatively large volume of dilute urine. This eliminates any excess water.
Polyuria and Polydipsia
Polyuria is the passage of larger volumes of urine than normal. Animals that cannot generate hypertonic urine when necessary become polyuric. Polydipsia is excessive thirst, and polyuric animals are often able to maintain water balance by increasing water intake. The increased intake is considered to be a sign of excessive thirst.
Polyuria and polydipsia (often abbreviated PU/PD) may develop in animals with unregulated diabetes mellitus and significant increases in blood glucose. The renal tubules cannot reabsorb the abnormally large amounts of glucose in the glomerular filtrate, and the glucose that remains in the renal tubules exerts an osmotic effect to retain water in the tubules. Increased urine flow results, and the animal must increase water intake to maintain water balance.
Polyuria and polydipsia may also result when ADH is not available (e.g., pituitary tumor preventing its release) or the kidney does not respond appropriately to ADH. in either case the water permeability of the collecting ducts remains relatively low, and water cannot be reabsorbed from the collecting ducts into the blood. Again, the affected animals must increase water intake to maintain water balance. This condition is diabetes insipidus.