Proximal Tubule Transport
The proximal convoluted tubule is the longest of the tubules, and proximal tubules make up most of the renal cortex. Typical proximal tubule cells are cuboidal, with a luminal border that is modified with microvilli (brush border).
The length and brush border provide for a large amount of cell membrane surface area, and the proximal tubule does more tubular transport than any other nephron segment. The cellular junctions between proximal tubule cells are also permeable to some substances in the filtrate (e.g. chloride ions) so that some transport can occur between the cells.Glucose and amino acids are examples of essential nutrients that are reabsorbed from the filtrate by cells of the proximal tubule. Normally, 100% of the glucose and amino acids in the initial filtrate are reabsorbed by the proximal tubule. This reabsorption involves secondary active transport using a sodium-linked cotransporter in a manner similar to glucose absorption in the small intestine (see Chapter 21, Fig. 21-7). Substances such as glucose that require membrane transporters for reabsorption have limits to the amount that can be reabsorbed as the fluid flows through the tubules. This limit is the tubular maximum, or transport maximum. The blood level at which the amount of a substance presented to the tubules by glomerular filtration exceeds the transport maximum is the renal threshold. Animals or people with uncontrolled diabetes mellitus often have blood glucose levels that exceed their renal thresholds for glucose. In these cases, the increased amounts of glucose in the filtrate cannot be completely reabsorbed by the proximal tubules, and glucose is present in voided urine (glucosuria).
Bicarbonate ions are the predominant base in the plasma and other extracellular fluids throughout the body. Normally, the proximal tubule reabsorbs almost 85-90% of the bicarbonate ions in the initial filtrate to maintain this ready supply of base. The transport of bicarbonate ions from the tubular lumen into proximal tubule cells entails their conversion to carbon dioxide and water under the influence of the enzyme carbonic anhydrase.
This reaction requires a hydrogen ion supplied by transport from within the tubule cell. once inside the tubule cell, the carbon dioxide and water are reconverted to bicarbonate and hydrogen ions, again under the influence of carbonic anhydrase. The bicarbonate ion can then exit the cell, using a membrane transporter, to be added to the blood again (Fig. 23-10). Sodium accompanies the bicarbonate ions, so the electrical neutrality of body fluids is maintained.Sodium and chloride are the two predominant osmolytes in the initial filtrate, and cells of the proximal tubule reabsorb 70-75% of the sodium and chloride in the initial filtrate. The percentage reabsorbed can be increased by the actions of angiotensin ii and sympathetic nerves on tubule cells and by vasoconstriction of renal blood vessels. Angiotensin ii concentrations and sympathetic nerve activity to the kidneys
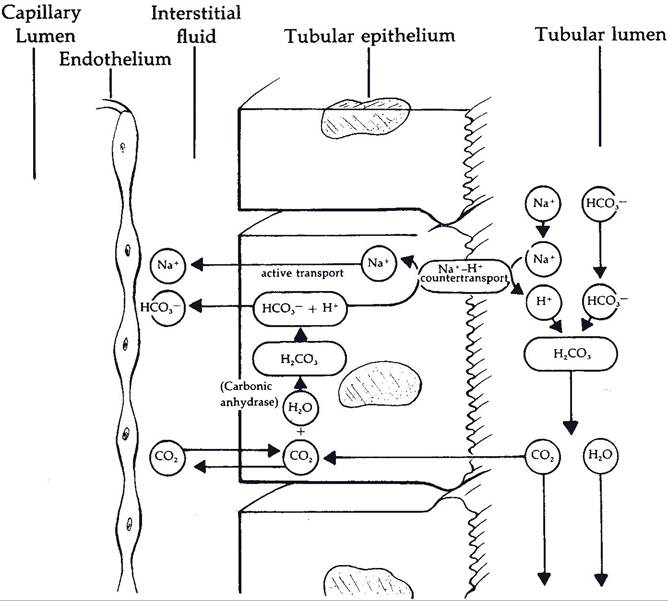
Figure 23-10. Mechanisms of reabsorption of bicarbonate ions by proximal tubule cells. (Reprinted with permission of Wiley-Blackwell from Reece W.O. Physiology of Domestic Animals. 2nd ed. Baltimore: Williams & Wilkins, 1997.)
increase during dehydration or blood loss, when it is appropriate to retain sodium chloride and water.
Cells of the proximal tubule also actively secrete organic anions and organic cations into the tubular fluid to be added to the urine. It is by these secretory systems that the kidneys eliminate many pharmaceuticals (that are organic compounds) in the urine.