Diagnosis of canine hepatic carcinoma
Due to the absence of nerves in the liver, the early liver neoplasia is painless. Therefore, when canine patients are clinically examined, their liver disease if any is diagnosed as moderate or severe.
The clinical symptoms include depression, lack of appetite, vomiting, weight loss, diarrhea, PU/PD, abdominal distention, lethargy, icterus, and ascites. The neurological disorder is mainly caused by hypoglycemia, hepatic encephalopathy, or metastasis of the central nervous system as shown in Figure 2 [9, 21-24].

Figure 2.
A 12-year-old female Maltese had distention of the abdomen, was diagnosed with a liver tumor via ultrasound.
2.1 Biological index
Hematologic features, including mild non-regenerative anemia, inflamed leukocytosis, and thrombocytosis, are common in canine liver tumors [1, 15, 16].
Thrombocytosis is observed in approximately half of canine patients with massive HCC [1]. The prolonged blood coagulation (prothrombin time, thrombin time, and activated partial thromboplastin time) is rare unless the liver disfunction occurs, being observed in only 20% of HCC cases [1, 16].
Serum biochemistry indexes of dogs with hepatic neoplasia are commonly increased. Thus, elevated enzyme alanine transaminase (ALT), alkaline phosphatase (ALP), and aspartate aminotransferase (AST) are observed in liver tumors. Moreover, AST to ALT ratios below one are consistent with HCC or bile duct carcinoma [1].
The increased content of α-Fetoprotein is used as a robust indicator of HCC in human patients [23, 24]. This indicator is less suitable for dogs with hepatic neoplasia, being intrinsic to other types of canine liver tumors. However, about 75% of dogs with HCC had increased serum α-Fetoprotein, as reported in [25, 26]. Hypoalbuminemia, hypoglycemia, hyperglobulinemia, and elevated bile acid concentration are also observed in canine liver tumors.
2.2 X-ray examination
Regular abdominal radiography images of canine patients obtained via a diagnostic X-ray device are used for diagnosing, staging liver tumors, and planning the surgery operation if any. Abdominal radiography may identify a cranial abdominal mass with caudal and lateral recumbency shift of the stomach. Ascites may interfere with visualizing a mass as depicted in Figure 3. Assessment of thoracic radiographs is considered critical to exclude metastatic disease.
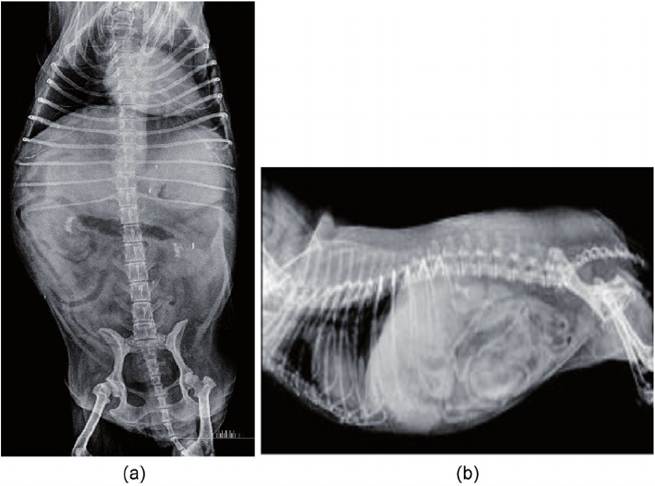
Figure 3.
(a) Right lateral recumbency of abdominal radiography. (b) Dorsal ventral recumbency of abdominal radiography. Two X-ray images were obtained from a Maltese with icterus and abdominal swelling. The liver board line is not obvious, rough, and hepatomegaly.
2.3 Abdominal ultrasound examination and MRI
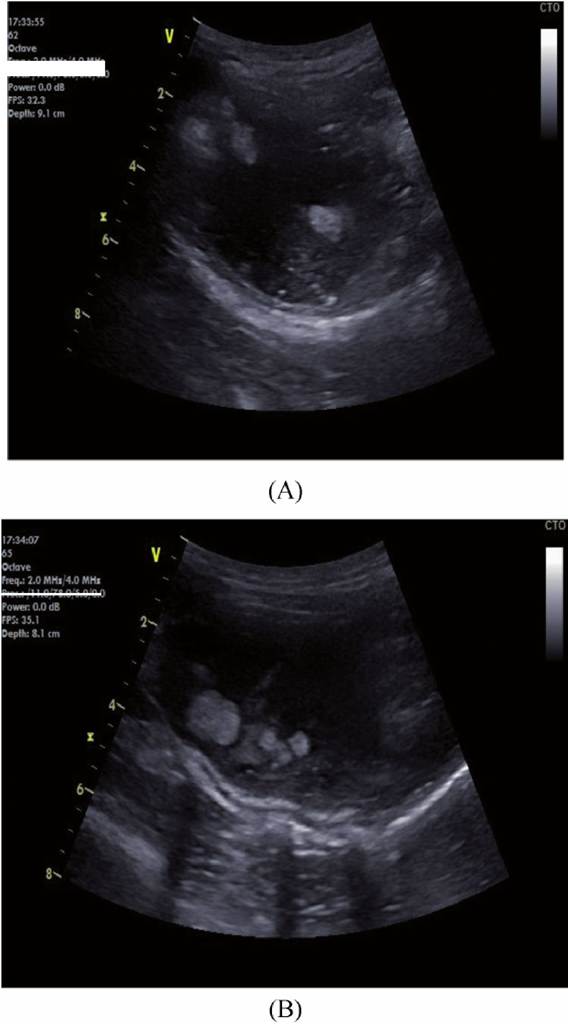
Abdominal ultrasound examinations are applicable to 94% of patients and allowed determination of an obvious mass in 99% of these patients. The efficiency
of the ultrasound method in detecting hepatic mass has been reported previously [1, 16]. In this study, the region containing the pathogenic mass (left, central, or right lobes) was correctly identified. This indicates that ultrasound examination is very sensitive in the identification of a mass as demonstrated in Figure 4. Besides the ultrasound examination, the magnetic resonance imaging (MRI) allows one to identify the tumor origin region. A variety of surgical planning modalities benefit from MRI accuracy in the localization of liver tumors; advanced imaging may be needed for precise tumor localization.
./11.0,71.0 5.0 0.0
Figure 4.
(A) Ultrasonography of right medial liver tumor. (B) Ultrasonography of right lateral liver tumor. Survey abdominal sonography 14.5y spayed female cocker spaniel dog before Ga67 examination, several hyperechoic nodules are seen within a large hypoechoic portion in the right medial and lateral hepatic lobe.
wq.: 10 MHi 4.0 MHi roct∕llΛ7tΛ,'5Λ∕0Λ
2.4 Ga-67 nuclear examination
Canine liver carcinoma cases were analyzed in this study via the nuclear examination technology. We have proposed a preliminary/simplified biokinetic model according to the general-purpose biokinetic model as recommended by the ICRP-30 report, to interpret the empirical data from the clinical examination of a case-control group of hepatic carcinoma dogs [27, 28]. In doing so, every dog was surveyed by a gamma camera/8-slice CT to derive eight complete scanned images within 72 hours. The raw outputs were processed with a self-developed program run in MATLAB to compose a thorough scenario of time-dependent Ga-67 nuclides’ intensity changes among multiple compartments (organs or tissues) for dogs that underwent a nuclear examination after being injected the Ga-67-citrate. Each canine patient was administered 22.2 MBq (0.6 mCi) Ga-67 citrate solution via the intravenous injection. The Ga-67 citrate solution was carrier-free with radionuclide and radiochemical purity values exceeding 99.9 and 95.0%, respectively. All radiopharmaceutical capsules were fabricated by the Syncor International Corporation (USA). The position-sensitive gamma ray emitted from the Ga-67 dose administration for each study object could be robustly assessed and plotted for further analysis. Figure 5 depicts the eight-compartmental biokinetic model of Ga-67 in liver figuring in the ICRP-30 report, which contains: (1) body fluid, (2) liver, (3) gastrointestinal (GI) tract, (4) kidney, (5) heart, (6) remainder, (7) bladder, and (8) excretion.
Figure 6 illustrates the fragments of scans obtained for a canine patient with liver carcinoma via a gamma camera: (A) The gamma camera/8 slice CT (GE Discovery NM/CT 670) facility indicates that the anesthetized dog was placed between two NM plates for scanning; (B) Close-up view of the anesthetized dog; (C) Particular scans were quoted directly from the E-CAM and implied the raw data
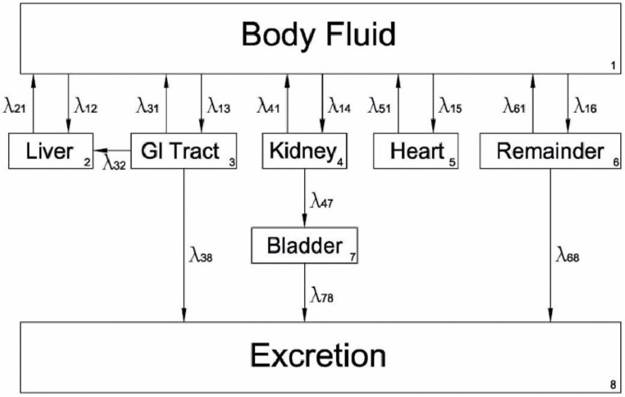
Figure 5.
A simplified biokinetic model of Ga-67 in the liver can be defined by eight major compartments: (1) body fluid, (2) liver, (3) gastrointestinal tract (GI tract), (4) kidney, (5) heart, (6) remainder, (7) bladder and (8) excretion according to ICRP-30 report.
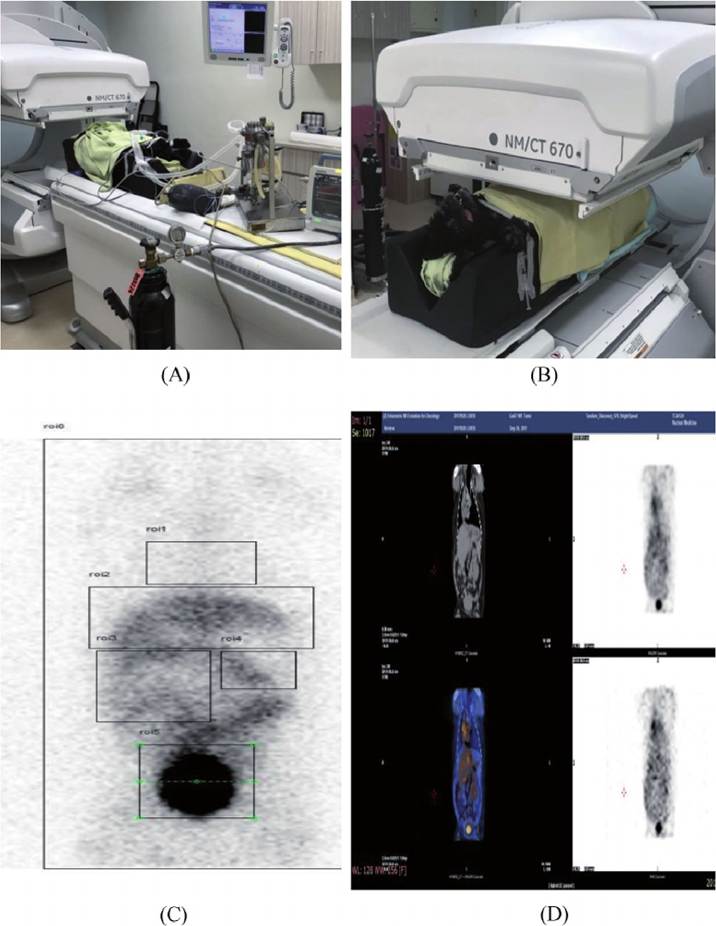
Figure 6.
(A) The gamma camera/8 slice CT (GE discovery NM/CT 670) facility indicates that the anesthetized dog was placed between two NM plates for scanning; (B) close up view of the anesthetized dog; (C)particular scans were quoted directly from the E-CAM and implied the raw data offifteen-minutes, counting after 72 elapsed hours. Here, the full-size scanning of the dog contained regions of interest (ROI), indicated as follows: ROIo (whole-body), RθIι (heart), ROI2 (liver), and ROI3 (GI tract), ROI4 (kidney), and ROI5 (bladder); (D) the fusion plot from gamma camera and CT scanning.
of 15 min counting after 72 elapsed hours. Here, the full-size scanning of the dog contained regions of interest (ROI), indicated as follows: ROI0 (whole-body), ROI1 (heart), ROI2 (liver), and ROI3 (GI tract), ROI4 (kidney), and ROI5 (bladder); (D) The fusion plot from gamma camera and CT scanning. The CT was preset at 130 kV, 150 mA, 0.8 sec., spin width 0.625 mm, spiral speed 3.75 mm/s, and matrix size 512 ? 512. The remainder was defined by subtracting all defined compartments (ROI1-5) from the whole body (ROI0).
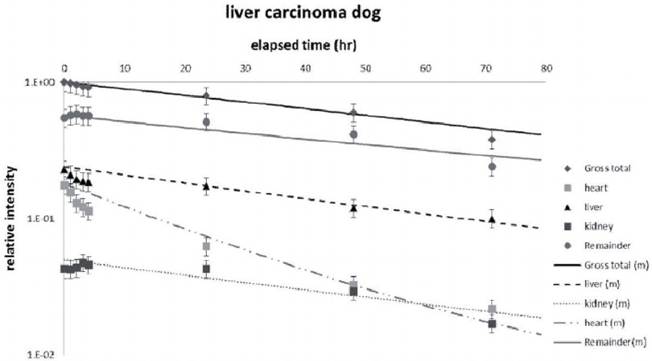
Figure 7.
The time-dependent curves of the Ga-67 concentration among various compartments for a liver carcinoma dog
Figure 7 shows the time-dependent curves of the Ga-67 concentration among various compartments for the dog with liver carcinoma.
Liver and GI Tract: In contrast to the I-131 thyroid model or GI Tract model for human patients, the model of Ga-67 for liver carcinoma dog was elaborated by the simplification of the general-purpose biokinetic model, according to the ICRP-30 report.
As seen in Figure 5, a complicated correlation among compartments allows one to use a MATLAB program to optimize the estimation via the empirical data [27]. The feedback path exists between compartments 2-6 and compartment 1. Each compartment has its biological half-life to transfer the Ga-67 radionuclides among compartments, which also confounds the theoretical estimation. Specifically, the liver provides a 22%-contribution of the body fluid (I12, 0.22), which is the second- largest share, whereas the GI Tract has the largest share (I13, 0.33 ~ 0.43) after the Ga-67 administration. However, 60% (I21, 0.60) of the Ga-67 radionuclides returns as feedback to the body fluid with a biological half-life of 15 ~ 40 h. Meanwhile, the remaining nuclides of Ga-67 in GI Tract are transferred to the body fluid (I31), liver (I32), or directly to excretion (I38) with a biological half-life of 20 ~ 600 h. Noteworthy is that the effective half-life is defined as the reciprocal of the sum of reciprocal radiological and biological half-lives (1/T1/2(eff) = 1/T1/2(R) + 1∕T1∕2(bio)). Thus, in practice, either 600 or 20 h of biological half-life still perform as 69 or 16 h of the effective half-life from the continuous gamma camera scanning. Some of Ga-67 radionuclides were found to migrate from the GI Tract to the liver (]32, 0.2 ~ 0.7). Since portal vein circulation provides the blood flow from gastrointestinal section to the liver, the excessive blood pressure will slow the liver’s feedback path.Kidney and bladder. Nearly 20% of Ga-67 nuclides were transferred to the kidney (I14, 0.2), exhibiting nearly no feedback to body fluid (I41, 0.07), in contrast to the bladder (I47, 0.93), and then were fully transferred to excretion (I78, 1.0).
Heart. Only 5-15% of Ga-67 nuclides were transferred to the heart (I15, 0.05-0.15), whereas most of them exhibited an instant feedback to body fluid (I51, 0.99) with a short biological half-time T1∕2 of 18-20 h. The derived biological half-life of the heart can be treated as a group of cardiac muscles, which provide the blood circulation loop in the whole body, with no apparent Ga-67 nuclides’ repository effect.
A long biological half-life of liver for the liver carcinoma dog (40 h vs. 35 h or 15 h) reveals a potential risk of hepatic disorder, whereas the remaining data are barely available to solidify the syndrome of liver carcinoma. The evolution of Ga-67 in the liver carcinoma survey model still plays an essential role in veterinary and human medical domains, since it quantifies the time-dependent concentration of Ga-67 nuclides among compartments of the case-control group and allows one to acquire robust raw data via in-vivo scanning.
3.