Introduction
1.1 Motivation and purpose
Dog owners are aware of the sad fact that their pets are vulnerable to various tumors that may occur at any age/location and cause severe complications.
In particular, canine hepatic tumors correspond to 0.6 to 1.3% of canine neoplasms, while about 7-36% of dogs are metastasized from other organs [1-9]. The canine patients, which usually suffer from systemic metabolic stress and cachexia, require a surgery or chemotherapy based on the veterinarians’ recommendations and life expectations. Noteworthy is that different tumor types of primary carcinoma can arise from different cell types listed in Table 1 [2]. The major types of primary liver cancer are hepatocellular carcinoma (HCC), bile duct carcinoma, neuroendocrine (carcinoid) tumor, and mesenchymal tumor (sarcoma). Hepatocellular carcinoma (HCC) is generally found in dogs, especially elder ones. Compared with the modular or diffuse forms, the majority of HCC has a lower rate of metastasis. A single massive HCC tumor can usually be removed by surgical treatment. However, the most difficult clinical treatment is the diffuse HCC involving in the entire liver. Dogs with multiple liver lobes’ HCC are not recommended to undergo surgical resection, have a poor prognosis and very limited treatment options [2-4, 10-13]. Bile duct carcinomas are the second common malignant liver tumor in dogs. Neuroendocrine tumors are quite rare and mostly nodular or diffuse, while primary liver sarcomas, including hemangiosarcoma, fibrosarcoma, and hepatocellular carcinoma, are unusual clinically. Dogs with liver tumors can be either asymptomatic or exhibit nausea, vomiting, weight loss, loss of appetite, diarrhea, lethargy, or PU/PD. Occasionally, yellowing of the skin and eyes like jaundice, or neurological signs (hepatic encephalopathy), such as seizures, disorientation, and weakness, are observed. Liver carcinoma grows slowly and manifests itself too late [2-6, 14-16]. This study attempts to set up the Ga-67 nuclear examination protocol for liver carcinoma canine patients, which would guide the veterinary expert and dog owner on the further optimal treatment: intensive surgery/chemotherapy or/and traditional Chinese veterinary medicine.1.2 Definition of critical terminology
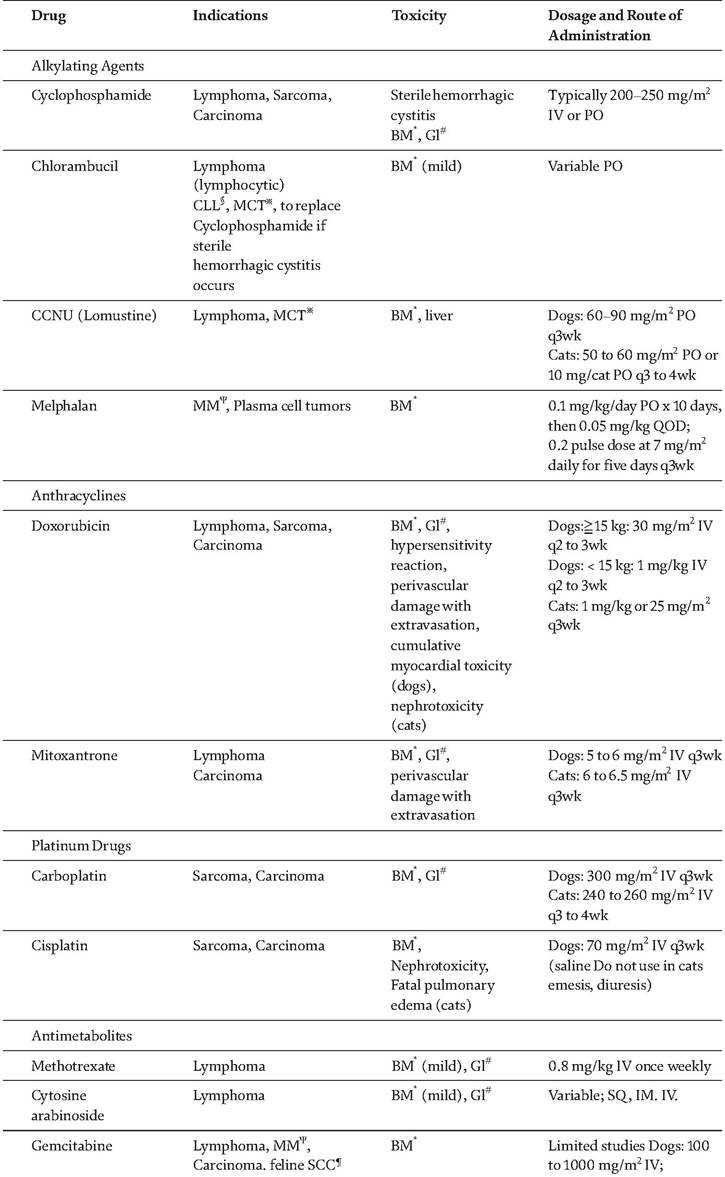
In this study, the global state-of-the-art approach to the above problem implies the conventional medicine based on modern science and advanced evaluation methods of canine physical and biochemical conditions. The respective treatment methods include chemotherapy, drugs, radiology, and surgery. Local tumor ablation and radiotherapy have been applied in veterinary medicine for decades. Chemotherapy is related to the use of several anti-cancer drugs administered intravenously, orally, or subcutaneously, which circulate in the patients body and attack cancer cells. The most common chemotherapy drugs for treating liver cancer are listed in Table 2. Alkylating agents react with DNA strands and change the DNA structure. The commonly utilized
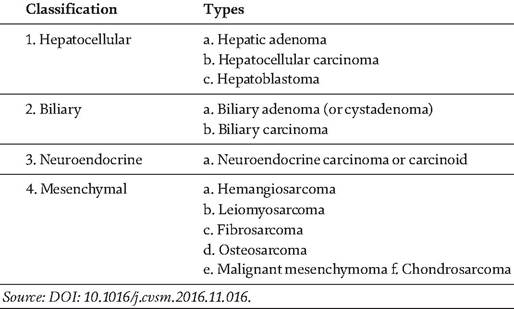
Table 1.
Primary hepatobiliary tumor types.
50 mg/m2
twice/wk. with RT ω Cats:
25 mg/m2 twice/wk. with RTω
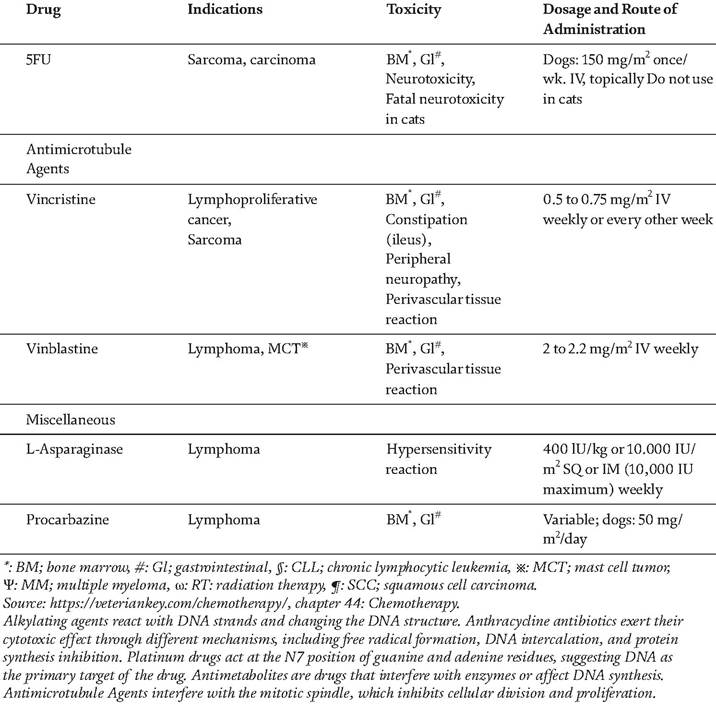
Table 2.
Classification of chemotherapy drugs for treatment.
alkylating agents in veterinary oncology are chlorambucil, cyclophosphamide, melphalan, and lomustine. The common toxicity of cyclophosphamide is related to sterile hemorrhagic cystitis. Anthracycline antibiotics exert their cytotoxic effect through different mechanisms, including free radical formation, DNA intercalation, and protein synthesis inhibition.
An example of such medicine is Mitoxantrone, which is metabolized in the liver and eliminated via feces and urine. Platinum drugs act at the N7 position of guanine and adenine residues, having DNA as their primary target and being eliminated via kidneys [6]. Antimetabolites are drugs that interfere with enzymes or affect DNA synthesis. Their chemo group, methotrexate, is primarily eliminated via renal excretion. Finally, there are antimicrotubule agents, which interfere with the mitotic division process, inhibiting cell division and proliferation.Quite a recent treatment introduced to veterinary oncology is radiology or radiation therapy. It rapidly became one of the most common procedures of cancer treatment, insofar as it could be clinically performed when surgical resection of the tumor remaining after chemotherapy would be problematic or too dangerous. Radiotherapy can make cells unable to replicate and eliminate the cell division and proliferation. However, radiation therapy can damage normal cells, rather than only malignant ones. A well-designed radiotherapy program is intended and designed to maximize tumor effect and minimize normal tissue effect. The benefit of radiotherapy is a cure for tumors and a split course treatment before surgery or chemotherapy [17].
The alternative approach to the above “targeted instrumental and drug invasion into the injured body part” is the overall improvement of the whole body and emotional well-being of a patient. In case of canine patients, this approach is reduced to the Traditional Chinese Veterinary Medicine (TCVM), which has been introduced several thousand years ago as a system of health care and is being implemented globally nowadays as alternative medicine [12]. Briefly, the TCVM has accumulated a vast list of robust diagnoses of canine diseases based on basic symptoms and appearances (tongue color, skin conditions, iris, pulse, etc.). A veterinarian analyzes these symptoms and the related overall system problems.
The proposed cure is TCVM-based herbal medicine aimed to fine-tune the immune system and prevent a reoccurrence of an illness or future problem as illustrated in Figure 1 [18, 19].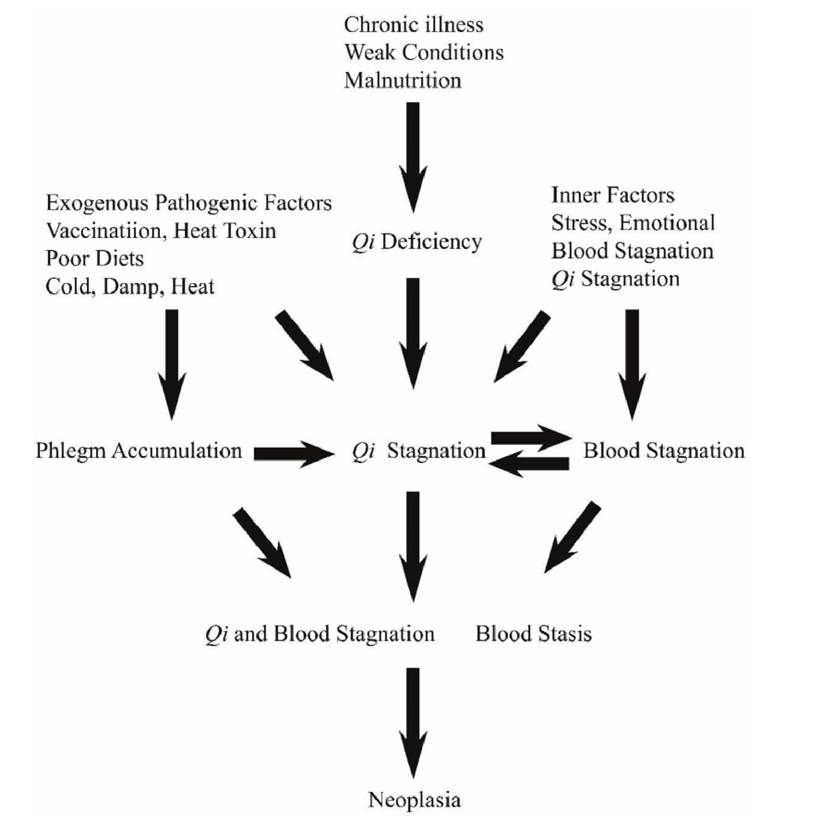
Figure 1.
Etiology of neoplasia in TCVM. The factors contributing to form phlegm, qi and blood stagnation, blood stasis, and eventually, neoplasia, are summarized. It is shown that qi deficiency is the root of cancer and phlegm, qi/blood stagnation, and blood stasis are one part of the branches. (cited from Huisheng Xie, Vanessa Preast, TCVM fundamental principles, 2nd edition).
1.2 Background review and rationale study with reference
Liver carcinoma can be diagnosed or detected by using multiple methods. Histological findings are considered the most robust for canine patients. The TNM staging system for canine hepatocellular carcinoma (HCC) is summarized in Table 3 [20]. Veterinary surgeons may perform additional blood examinations to look for signs of liver dysfunction. Surgery is one of the treatments for all liver tumors. However, right-sided tumors are more challenging to resect because the resection lesion is related to the vena cava [2]. For massive hepatic carcinoma, surgical resection via lobectomy is the treatment when complete resection is accepted [10, 11]. The mass ligation for complete lobectomy is not recommended for large dogs, or central or right divisional liver tumors, because this method will increase the risk of complications, such as bleeding or bile leakage. Surgical stapling devices are recommended to perform liver lobectomy; in these devices, overlapping rows of staples are quickly placed to attenuate vascular and biliary structures within the liver lobe’s hilus. If stages T3, N1, or M1 in Table 3 are confirmed by clinical- stage evaluations, no surgical resection is recommended [20] because it would not remove some malignant liver tumors. Therefore, chemotherapy becomes an alternative treatment.
Unfortunately, according to many clinical practices and references, chemotherapy is not very effective liver carcinoma treatment. Thus, HCC treatment with intravenous gemcitabine or carboplatin is no longer performed. Instead, in the last decade, the Metronomic chemotherapy and Sorafenib treatment (5 mg/kg, twice daily) became widely used due to lower-dose usage and administration ease [6, 7].Alternatively, radiotherapy is sometimes used to make the liver tumor smaller or incapsulate it. However, it is not applicable to most liver tumor cases because of its side-effects. The major complication is a radiation heat-induced damage to the adjacent unaffected liver tissue. A 3D-CRT (three-dimensional conformal radiation therapy) is introduced as a new viable treatment option for canine patients with an inoperable massive liver carcinoma. From 6 to 10 Gy per fraction are prescribed on the planning target volume, and the total dose is 18-42 Gy with 1 to 2 fractions per week [17].
1.3 The innovative features of this study
This study is the first attempt to apply the biokinetic Ga-67 model to canine liver carcinoma. The aim is to identify the best routine for detecting the metastatic or primary hepatic carcinoma and substantiating the optimal further treatment.
| Classification | stage |
| Primary tumor (T) | T0: no evidence of primary tumor Tl: solitary tumor of any size involving one lobe T2: multiple tumors of any size involving multiple lobes T3: tumor(s) with direct invasion of adjacent organs regional lymph nodes |
| Regional lymph nodes (N) | N0: no regional lymph nodes metastasis Nl: regional lymph node metastasis N2: lymph node metastasis Distant metastasis |
| Distant metastasis (M) | M0: no distant metastasis Ml: distant metastasis |
| Source: doi:l0.3390∕cancersl205l272 | |
| Table 3. The TNM staging system for canine hepatocellular carcinoma. | |
1.4 The specific rationale study with a solid description
The biokinetic model of Ga-67 evolution was elaborated in this study for the case-control group of canine liver carcinoma via in-vivo gamma camera/8-slice CT technique. The circulation of time-dependent concentrations of Ga-67 among organs was monitored and simulated. The obtained quantitative data for organs and branching ratios among organs were incorporated into the biokinetic model of Ga-67 radionuclide administered during the hepatic survey.
2.