Disease of Lower Motor Neurons Causes Stereotypical Clinical Signs
Regardless of the pathological basis for disease of lower motor neurons, a stereotypical set of clinical signs results in the skeletal muscles they innervate.
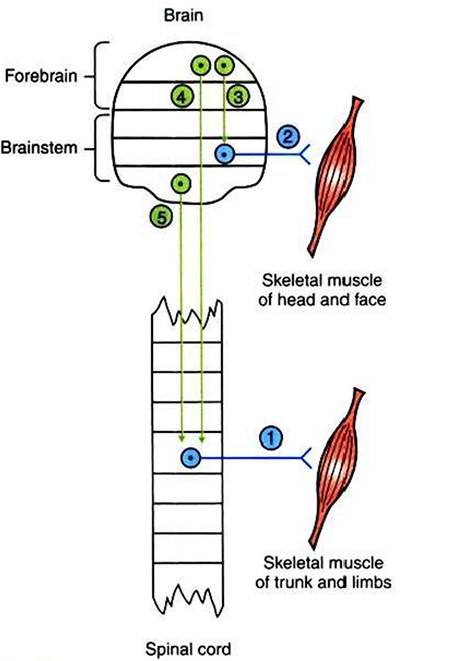
FIGURE 9-1 ■ General organization of lower and upper motor neurons.
Blue, Lower motor neurons typically originate in the ventral horn of the spinal cord (neuron 1) or in cranial nerve nuclei (neuron 2) and synapse within skeletal muscle. Green, Upper motor neurons typically originate in the brain and project to and control lower motor neurons. Upper motor neurons usually belong to the Corticobulbar (neuron 3), corticospinal (neuron 4), or bulbospinal, also called brainstem motor (neuron 5), pathways. Arrowheads indicate that local synapses may be interposed between the upper and lower motor neurons. Horizontal lines delimit either spinal cord segments (e.g., L1, L2) or major brain divisions (e.g., medulla, pons).1. Paralysis or paresis. Disease of the α motor neurons usually prevents the neurons’ action potentials from reaching the neuromuscular junction. Therefore, despite the brain’s command to the muscle to contract, the message cannot reach the muscle, and paralysis is the result. In fact, such paralysis can be so complete that the adjective flaccid is used to describe the paralysis in which no muscle contraction occurs. Because not all the α motor neuron axons of a peripheral nerve may be affected by an insult, and because muscles can be supplied by axons of more than one spinal nerve, paralysis may be incomplete. This symptom is referred to as paresis.
2. Atrophy. Atrophy is the shrinking or wasting of skeletal muscle mass distal to the lower motor neuron lesion. This occurs within days of the injury to a nerve. The exact origins of this atrophy are controversial.
However, evidence indicates that the reduced frequency of muscle stimulation caused by α motor neuron insult and the resulting reduced use of the muscle trigger reductions in muscle protein synthesis and increases in muscle proteolysis. The magnitude of this denervation atrophy can be reduced by direct electrical stimulation of the muscle itself.3. Loss of segmental and intersegmental reflexes. Segmental and intersegmental reflexes require a viable α motor neuron in the reflex arc for the reflex response to occur (see Chapter 7). Therefore, such reflexes as the muscle stretch (knee jerk) reflex and the toe-pinch withdrawal (nociceptive) reflex, as well as the proprioceptive positioning reaction, fail to occur because the motor neuron portion of the arc, which activates the skeletal muscle, is gone.
4. Electromyographic changes. Within a few days of damage to α motor neurons, abnormal electrical activity of the muscle can be observed on an electromyogram (see Chapter 6). Damage of α motor neurons occurs often on insult to a
peripheral nerve that also contains axons of sensory neurons. Therefore, there may be an accompanying loss of sensory modalities, although this is not a cardinal sign of lower motor neuron damage.