EXTRACELLULAR FLUID VOLUME REGULATION
1. How do osmoregulation and volume regulation differ?
2. Where are the receptors located that respond to blood volume changes?
3. What are the graded responses to efferent renal sympathetic nerve activity?
In osmoregulation (regulation of ECF osmolality), the ratio of Na+ to water (osmoconcentration) is being regulated, and in volume regulation (regulation of ECF volume and hence blood volume), the absolute amounts of Na+ and water that are present are being regulated.
The principal receptors responding to acute changes in blood volume are those in the left atrium of the heart. Vagal nerve afferents from these receptors provide a neural link between the heart as a sensor of blood volume and the kidneys as effector organs. In hypovolemia (abnormally decreased volume of circulating fluid in the body), there is decreased left atrial filling that is followed by decreased vagal afferent stimulation and responses that are summarized in Finure 11-21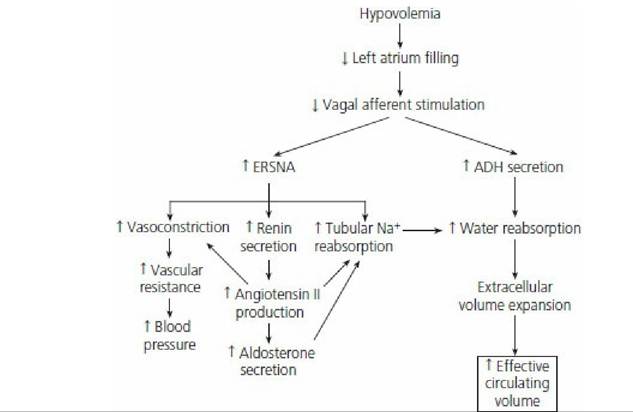
■ FIGURE 11-21 Renal and cardiovascular responses induced by the sympathetic division of the autonomic nervous system in response to reduced circulating volume (hypovolemia). Efferent renal sympathetic nerve activity (ERSNA) responses are graded depending on the severity of hypovolemia. Accordingly, renin secretion is the first response, followed by tubular Na+ reabsorption, and finally vasoconstriction to alleviate declining blood pressure associated with hypovolemia. ADH, antidiuretic hormone. (From Reece WO. Kidney function in mammals. In: Reece WO, ed. Dukes’ Physiology of Domestic Animals. 13th edn. Ames, IA: Wiley-Blackwell, 2015.) Stimulation to the kidneys is provided by efferent renal sympathetic nerve activity with innervation to the JG granular cells, the nephron tubules, and the renal vasculature. Each of these groups is innervated by functionally specific groups of the sympathetic nerves. Accordingly, the responses to the groups are graded and, with increasing intensity, renin secretion from the JG granular cells increases first, followed by increased renal tubular reabsorption of sodium, and, lastly, by renal vasoconstriction with decreases in RBF and increased vascular resistance. These effects can override autoregulatory responses.
■