CONCENTRATION OF URINE
1. Where is the degree of dehydration of the ECF detected?
2. Where does ADH exert its influence?
3. What is the direction of water diffusion (i.e., collecting duct to medullary ISF or vice versa) when ADH secretion is increased?
4.
What blood vessels collect water reabsorbed into the interstitial space of the medulla?5. What is the approximate urine-to-plasma osmolal ratio in the dog? How does this compare to that of humans? Would greater urine concentration be possible where the ratio is increased?
6. How do diabetes insipidus and diabetes mellitus differ regarding cause of observed polydipsia and polyuria?
7. What are reasons for concentration failure in chronic renal failure disease?
There is continued active transport of NaCl and low permeability for water and urea.in the distal tubule. At the end of the distal tubule, and before the fluid enters the cortical collecting tubules and ducts, the osmolality is about 150 mOsm. Tubular fluid entering the distal tubules has an osmolality lower than that of plasma because of the removal of Na+ and Cl- that occurred in the ascending limb of the loops of Henle along with the simultaneous retention of water.
Antidiuretic Hormone and Osmoregulation
The epithelial cells of the collecting tubules and collecting ducts have a variable permeability for water, depending on the amount of ADH that has been secreted from the posterior pituitary gland. ADH increases the permeability of these cells for water. Significant changes occur in the rate of ADH secretion when there are deviations in the plasma osmolality of as little as 2% in either direction.
The degree of hydration of the ECF is detected by osmoreceptor cells in the hypothalamus. The osmoreceptors of the hypothalamus respond to effective osmotic pressure; hence, an increase in osmolality must be caused by substances restricted from diffusion into the osmoreceptor cells.
For this reason, the osmoreceptor cells are often considered to be Na+ receptors because Na+ is the nondiffusible cation with the greatest concentration in the ECF. An osmolality increase as a result of urea (freely diffusible) does not stimulate the receptors. When the cells detect increased plasma osmolality (hyperosmolality), they stimulate the posterior pituitary to secrete more ADH and, when decreased plasma osmolality (hypoosmolality) is detected, the rate of ADH release is decreased. The secreted ADH is circulated by the blood to the kidney tubules, where the water permeability changes take place (Figure 11-19). The thirst center, also located in the hypothalamus, is stimulated by hyperosmolality. A water deficit requires water intake for correction, and animals seek water. The responses to increased plasma osmolality are summarized in Figure 11-20.
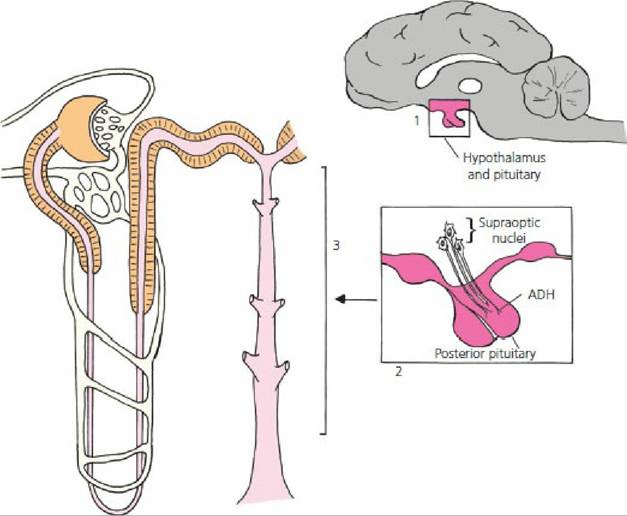
■ FIGURE 11-19 Relationships among the hypothalamus, posterior pituitary, and kidneys in the regulation of extracellular hydration. (1) Extracellular dehydration detected by osmoreceptors in the hypothalamus. Boxed area in 1 shows the location in the brain of the boxed area in 2. (2) ADH (neurosecretion of supraoptic nuclei in hypothalamus) secreted into blood in response to dehydration. (3) Cortical collecting tubules and medullary collecting ducts are targets of ADH, causing increased reabsorption of H2O.
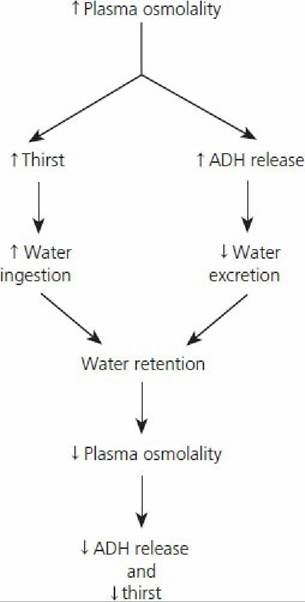
■ FIGURE 11-20 Cycle of events for the relief of hyperosmolality. Increased thirst is the predominant factor for the correction of hyperosmolality. ADH, antidiuretic hormone. (From Reece WO. Kidney function in mammals. In: Reece WO, ed. Dukes’ Physiology of Domestic Animals. 13th 2dn. Ames, IA: Wiley-Blackwell, 2015.)
Hypotonic tubular fluid entering the collecting tubules and ducts could be excreted as urine if water was not reabsorbed.
This happens in diabetes insipidus, in which there is either an absence of ADH or severely decreased amounts of ADH. Animals with this condition have clinical signs of polyuria (formation and excretion of a large volume of urine) and polydipsia (excessive thirst manifested by excessive water intake). The urine formed is dilute and has a lower-than-normal specific gravity. Animals with diabetes mellitus may also show polyuria and polydipsia. Polyuria in this disease is caused by an osmotic diuresis because of the presence of glucose in the urine (failed to be reabsorbed) and is not caused by a lack of ADH. The urine specific gravity is likely to be higher than normal and would test positive for glucose. As in diabetes insipidus, polydipsia is a compensation for the polyuria to overcome the water deficit.In healthy animals, when tubular fluid enters the collecting tubules and ducts, water is reabsorbed as it proceeds to the renal pelvis because it is exposed to effective osmotic pressures of increasing magnitudes in the ISF of the kidney medulla, as established by the countercurrent mechanism. ADH secretion is consistent with the need for water conservation. In extreme cases of water conservation, it would be possible for the osmolality of the tubular fluid, and hence that of the urine, to approach the osmolality of the ISF in the innermost region of the medulla. In the dog, this would approach 2,400 mOsm and the urine-to-plasma osmolal ratio (2,400:300) would be approximately 8:1. The urine would have a concentration eight times that of plasma. Some desert rodents attain a urine-to- plasma osmolal ratio of about 16:1. This ratio represents an extreme adaptation for body water conservation. Environmental water is not available for desert animals (water gain mostly metabolic water) and water losses are minimized for survival. Table 11-3 compares the percentage of long- looped nephrons (loops of Henle extending deeply into the medulla) and relative medullary thickness of different animals.
The relative medullary thickness is derived from measurements of the depth of the medulla from the corticomedullary junction to its innermost depth, which protrudes into the renal pelvis. Relative medullary thickness is believed to be a better predictor of urine concentrating ability than percentage of long-looped nephrons. As judged by freezing point depression (solute particles lower the freezing point of solutions), the kangaroo rat has the greatest concentrating capacity for urine. As compared with humans, it seems that its innermost medullary osmolality would be about four times that of humans, or about 4,800 mOsm.| TABLE 11-3 RELATIONSHIP OF STRUCTURE TO CONCENTRATING CAPACITY IN MAMMALIAN KIDNEYS | ||||
| ANIMAL | KIDNEY SIZEa (mm) | LONG-LOOPED NEPHRONS (%) | RELATIVE MEDULLARY THICKNESSb | MAXIMUM FREEZING POINT DEPRESSION IN URINE (°C) |
| Beaver | 36 | 0 | 1.3 | 0.96 |
| Pig | 66 | 3 | 1.6 | 2 |
| Human | 64 | 14 | 3 | 2.6 |
| Dogc | 40 | 100 | 4.3 | 4.85 |
| Cat | 24 | 100 | 4.8 | 5.8 |
| Rat | 14 | 28 | 5.8 | 4.85 |
| Kangaroo rat | 5.9 | 27 | 8.5 | 10.4 |
| Jerboa | 4.5 | 33 | 9.3 | 12 |
| Psammomys | 13 | 100 | 10.7 | 9.2 |
| aKidney size = cube root of the product of the dimensions of the kidney. bRelative medullary thickness = medullary thickness in millimeters = 10 ÷ kidney size. cBeeuwkes and Bonventre have shown (1975) that the dog kidney does contain short-looped or corticomedullary nephrons; therefore, long-looped nephrons compose fewer than 100% of the nephrons.From Schmidt-Nielsen B, O’Dell R. Structure and concentrating mechanism in the mammalian kidney. Am J Physiol. 1961; 200: 1119-1124. | ||||
Other Factors Affecting ADH Release
ADH release from the posterior pituitary is influenced by other factors in addition to hydration of the ECF. Cold environments inhibit ADH release, so urine production and water intake increase. The need for water intake results from thirst induced by water loss from diuresis. The need for water availability in cold weather is apparent.
Ethyl alcohol inhibits ADH secretion and dehydration is a consequence of alcohol consumption (not a factor for domestic animals).
Concentration Failure
In addition to diabetes insipidus, other kidney disease processes are characterized by decreased concentrating ability. Impaired concentrating ability is notable in chronic renal failure. Reasons cited are as follows:
1. More solute than usual is presented to the remaining functional nephrons, whereby the high solute content in the tubules contributes to osmotic diuresis.
2. Hypertonicity in the medullary ISF is not maintained because of: (a) loss of medullary tissues or decreased blood flow in the vasa recta and (b) decreased Na+ and Cl- transport from the thick segment of the ascending limb of the loop of Henle.
3. Damage to cells in the collecting tubules and collecting ducts makes them less responsive to ADH.
■