FACTORS ASSOCIATED WITH BREATHING
1. Under normal conditions, is greater effort required for inspiration or for expiration?
2. Define a complementary breathing cycle.
3. Differentiate between abdominal and costal breathing.
When is either accentuated?4. What are some commonly referred to states of breathing?
5. Respiratory frequency is an excellent indicator of health, but what are some variations that must be considered for its interpretation?
6. Be aware of the terminology associated with lung sounds.
7. Know the subdivisions of lung volume. What is the difference between a lung volume subdivision and a lung capacity subdivision?
Many factors of breathing terminology must be understood for one to observe, describe, and measure individual animal behavior related to respiration.
Respiratory Cycles
A respiratory cycle consists of an inspiratory phase followed by an expiratory phase. Inspiration involves an enlargement of the thorax and lungs, with an accompanying inflow of air. The thorax enlarges by contraction of the diaphragm (the musculotendinous separation between the thorax and abdomen) and by contraction of external intercostal muscles (muscles located between the ribs) (Figure 10-11). Diaphragmatic contraction enlarges the thorax in a caudal direction and external intercostal muscle contraction enlarges the thorax in a cranial and outward direction. Under normal breathing conditions, inspiration requires greater effort than expiration, and sometimes expiration might seem to be passive. Expiration can become quite an active process, particularly during times. of accelerated breathing and also when there are impediments to the outflow of air..The appropriate intercostal muscles contract to assist in expiration. Other skeletal muscles can aid in either inspiration or expiration, such as the abdominal muscles. When contracted, these muscles force the abdominal viscera forward to press on the diaphragm, which in turn decreases thoracic volume.
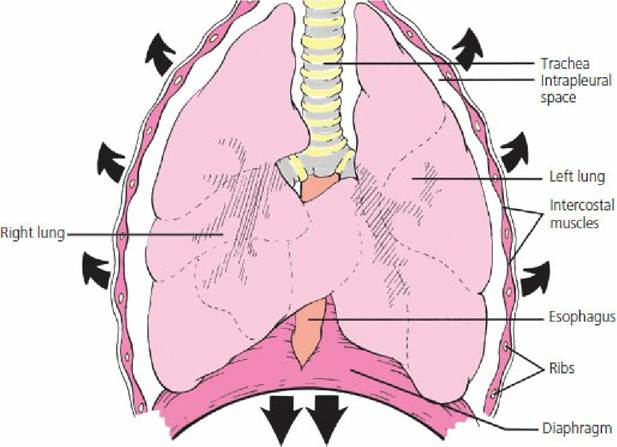
■ FIGURE 10-11 Schematic of the thorax during inspiration (ventral view). Shown are the directions of enlargement (arrows) when the diaphragm and inspiratory intercostal muscles contract during inspiration.
Complementary breathing cycles are characterized by a deep rapid inspiration followed by expiration of longer duration. They occur normally in many species but apparently not in the horse. This type of cycle has frequently been called a sigh. As it naturally occurs, it is probably a compensatory mechanism for poor ventilation. In laboratory exercises where ventilation is impaired by the addition of dead space volume, not only do respiratory frequency and tidal volume increase but also the number of complementary breathing cycles. Anesthetists often create complementary breaths at regular intervals by manually compressing the rebreathing bag.
Types of Breathing
There are two types of breathing: abdominal and costal. Abdominal breathing is characterized by visible movements of the abdomen, in which the abdomen protrudes during inspiration and recoils during expiration. Normally the abdominal type of breathing predominates. The other type is called costal breathing; it is characterized by pronounced rib movements. During painful conditions of the abdomen, such as peritonitis, in which movement of the viscera would aggravate the pain, costal breathing can predominate. Similarly, during painful conditions of the thorax, such as pleuritis, abdominal breathing might be more apparent. Binding of the thorax to minimize the outward and cranial expansion of the thorax requires greater diaphragmatic effort, and subsequent movement of abdominal viscera accentuates the abdominal type of breathing.
States of Breathing
In addition to the different types of breathing, there are variations in breathing relating to the frequency of breathing cycles, depth of inspiration, or both.
Eupnea is the term used to describe normal quiet breathing, with no deviation in frequency or depth. Dyspnea is difficult breathing, in which visible effort is required to breathe. The animal is usually aware of this breathing state. Hyperpnea refers to breathing characterized by increased depth, frequency, or both, and is noticeable after physical exertion. The animal is not acutely conscious of this state. Polypnea is rapid, shallow breathing, somewhat similar to panting. Polypnea is similar to hyperpnea in regard to frequency, but is unlike hyperpnea in regard to depth. Apnea refers to a cessation of breathing. However, as used clinically, it generally refers to a transient state of cessation of breathing. Tachypnea is excessive rapidity of breathing and bradypnea is abnormal slowness of breathing.Respiratory Frequency
Respiratory frequency refers to the number of respiratory cycles each minute. It is an excellent indicator of health status, but must be interpreted properly because it is subject to numerous variations. In addition to variations observed among species, respiratory frequency can be affected by other factors, such as: (1) body size, (2) age, (3) exercise, (4) excitement, (5) environmental temperature, (6) pregnancy, (7) degree of filling of the digestive tract, and (8) state of health. Pregnancy and digestive tract filling increase frequency because they limit the excursion of the diaphragm during inspiration. When expansion of the lungs is restricted, adequate ventilation is maintained by increased frequency. For example, when cattle lie down, the large rumen pushes against the diaphragm and restricts its movement, and the respiratory frequency is seen to increase.
Respiratory frequency usually increases during disease. Thus, frequency is a useful determinant of health status, but the frequency for a species under various conditions must be known so that this parameter can be interpreted properly (Table 10-1). Values are meaningful only when obtained unobtrusively from animals at rest.
| TABLE 10-1 RESPIRATORY FREQUENCY FOR SEVERAL ANIMAL SPECIES UNDER DIFFERENT CONDITIONS | ||||
| CYCLES/MIN | ||||
| ANIMAL | NUMBER | CONDITION | RANGE | MEAN |
| Horse | 15 | Standing (at rest) | 10-14 | 12 |
| Dairy cow | 11 | Standing (at rest) | 26-35 | 29 |
| 11 | Sternal recumbency | 24-50 | 35 | |
| Dairy calf | 6 | Standing (52 kg body weight,,3 weeks old) | 18-22 | 20 |
| 6 | Lying down (52 kg body.weight, 3 weeks old) | 21-25 | 22 | |
| Pig | 3 | Lying down (23 to 27 kg body weight) | 32-58 | 40 |
| Dog | 7 | Sleeping (24 °C) | 18-25 | 21 |
| 3 | Standing (at rest) | 20-34 | 24 | |
| Cat | 5 | Sleeping | 16-25 | 22 |
| 6 | Lying down, awake | 20-40 | 31 | |
| Sheep | 5 | Standing, ruminating, 1/2 inch wool, 18 °C | 20-34 | 25 |
| 5 | Same sheep and conditions,except 10 °C | 16-22 | 19 | |
From Reece WO. Respiration in mammals.
Average of values obtained from student laboratory assignments. In: Reece WO, ed. Dukes' Physiology of Domestic Animals. 13th edn. Ames, IA: Wiley-Blackwell, 2015.
Lung Sounds
It is obvious from Figure 10-7 that considerable branching of the pulmonary airways occurs. Although the branches may have smaller diameters than the parent branch, the combined crosssectional area of the branches shows an increase over that of the parent. Consequently, the velocity of air flow diminishes progressively from the trachea toward the bronchioles. Listening for lung sounds with the aid of a stethoscope is termed auscultation. A good-quality stethoscope should be used in quiet surroundings. The high-velocity, turbulent air flow in the trachea and bronchi produces the lung sounds heard through a stethoscope in a normal animal. Laminar, low-velocity flow in the bronchioles produces no sound. To amplify the sounds, deep respiratory efforts can be produced by placing an adequately sized plastic bag loosely over the muzzle of the animal.
The term breath sound applies to any sound that accompanies air movement through the tracheobronchial tree. Breath sounds vary randomly in intensity over a broad range depending on whether the sounds are produced over the larger airways or over the remaining lung parenchyma. Adventitious sounds are extrinsic to the normal sound production mechanism of the respiratory tract and are abnormal sounds superimposed on the breath sounds. Adventitious sounds are further classified as crackles and wheezes. Diseases resulting in edema or exudates within the airways can result in crackles. Wheezes suggest airway narrowing (e.g., bronchoconstriction, bronchial wall thickening, external airway compression).
With the exception of laminar, low-,velocity flow in the bronchioles (noted above), the absence of respiratory sounds implies that nonfunctional lung tissue is beneath the stethoscope.
Pulmonary Volumes and Capacities
Conventional descriptions for lung volumes are either associated with the amount of air within them at any one time or with the amount associated with a breath.
Tidal volume is the amount of air breathed in or out during a respiratory cycle. It can increase or decrease from normal, depending on ventilation requirements. Tidal volume is probably used more frequently than other terms. Inspiratory reserve volume is the amount of air that can still be inspired after inhaling the tidal volume and expiratory reserve volume is the amount of air that can still be expired after exhaling the tidal volume. Residual volume is the amount of air remaining in the lungs after the most forceful expiration. Also, some part of the residual volume remains in the lungs after they have been removed from the thorax during slaughter or for postmortem examination. Because of the remaining residual volume, excised lung sections float in water. Consolidation of lung tissue, as occurs in pneumonia, causes them to sink. Sometimes it is useful to combine two or more of these volumes. Such combinations are called capacities. Total lung capacity is the sum of all volumes. Vital capacity is the sum of all volumes over and above the residual volume; it is the maximum amount of air that can be breathed in after the most forceful expiration. Inspiratory capacity is the sum of the tidal and inspiratory reserve volumes. Functional residual capacity is the sum of the expiratory reserve volume and the residual volume. This is the lung volume that is ventilated by the tidal volume. It serves as the reservoir for air and helps to provide constancy to the blood concentrations of the respired gases. Relationships of pulmonary volumes and capacities are illustrated in Figure 10-12.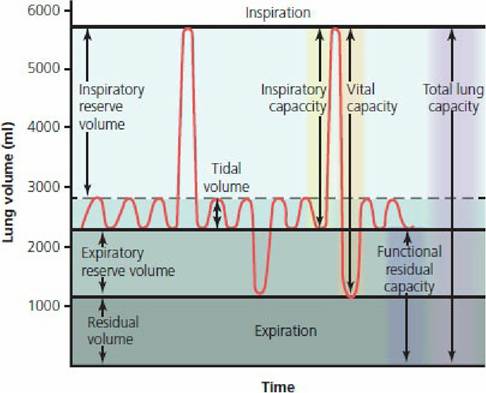
■ FIGURE 10-12 Subdivisions of lung volume. The values shown for lung volume are those that approximate values for an average adult human male. (From Guyton AC, Hall JE. Textbook of Medical Physiology. 11th edn. Philadelphia, PA: Elsevier Saunders, 2006.)
■