GASTROINTESTINAL MOTILITY
1. Study Figure 12-30 and review nerve impulse transmission to understand changes in intestinal motility.
2. What is the basic difference between segmentation and peristalsis? How would you define peristalsis?
3.
Would peritonitis (e.g., from hardware disease in cattle) inhibit intestinal activity?4. How do gastrin, cholecystokinin, and secretin affect gastrointestinal motility?
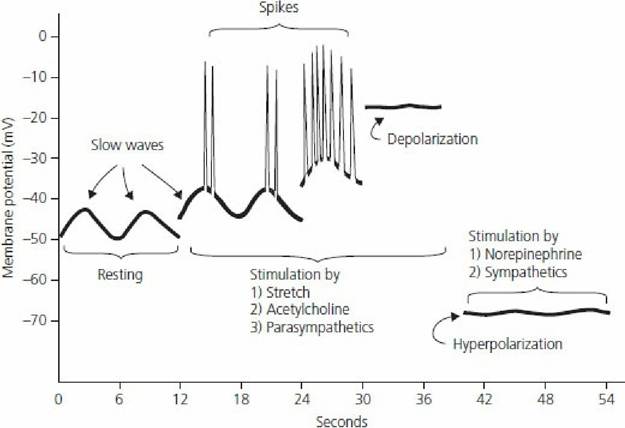
■ FIGURE 12-30 Membrane potentials in mammalian intestinal smooth muscle. Note the slow waves, spike potentials, and directions of depolarization and hyperpolarization. (From Guyton AC, Hall JE. Textbook of Medical Physiology. 10th edn. Philadelphia, PA: WB Saunders, 2000.)
Once food reaches the stomach, its movement is controlled by the activity of the smooth muscle in the wall of the stomach and intestine. Muscle activity is spontaneous (myogenic) and is modulated by the autonomic nervous system. Smooth muscle is an excitable tissue, and the resting membrane potential of about -50 mV is subject to fluctuation (Figure 12-30). The fluctuations are represented by slow waves characterized by slow, transient, undulating changes of the resting membrane potential that are propagated for varying distances. When the peak (toward positive) of a slow wave reaches threshold (membrane potential at which an action potential is produced), a spike potential (true action potential) is observed, and muscle contraction follows. The greater the encroachment of the peaks of slow wave potentials on the threshold potentials, the greater the frequency of the spike potentials, and gastrointestinal muscle contraction is sustained for a longer period.
The duration of spike potentials is longer in gastrointestinal smooth muscle than in nerve fibers because, in addition to the inflow of Na+ associated with depolarization, there is also an inflow of Ca2+; the “channels” that permit Ca2+ to enter are slower to open and close than the Na+-only channels of nerve fibers.
In addition, the calcium ions that enter are associated with the actin and myosin interaction of contraction. A representation of spikes.superimposed on slow waves is shown in Figure 12-30. Less-negative values (toward positive) are associated with depolarization and more-negative values (further from threshold) are associated with hyperpolarization. The rhythmical frequencies of the slow waves represent the maximum frequency for contraction and act as pacemakers. Parasympathetic stimulation causes the resting membrane potential to approach threshold, resulting in depolarization, and increases spiking that results in more vigorous gastrointestinal activity, whereas sympathetic stimulation hyperpolarizes and reduces spiking that results in decreased gastrointestinal activity.Segmentation and Peristalsis
Two important intestinal reflexes are segmentation and peristalsis. Segmentation movements are myogenic (i.e., property of smooth muscle cells) and do not depend on a nervous mechanism. Segmentation causes back-and-forth mixing as a result of intermittent circular muscle contractions occurring at different sites on an intestinal segment (Figure 12-31). Contraction is initiated by distention and chyme is moved in both directions, creating new distentions that are followed by contractions. Segmentation movements promote digestion and absorption by mixing chyme and bringing it into contact with the epithelial cells lining the intestinal lumen.
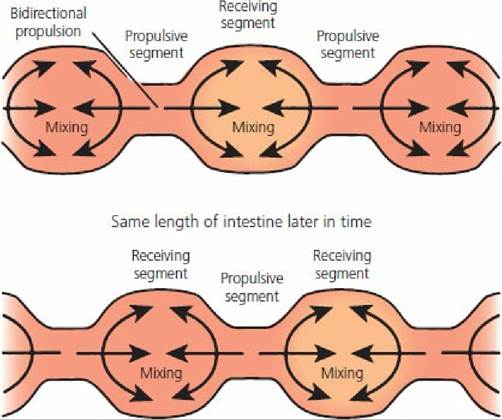
■ FIGURE 12-31 Segmentation contractions of the small intestine. Movement of chyme into the receiving (relaxed) segment by the propulsive (contracting) segment results in mixing. The receiving segment then becomes the propulsive segment and mixing continues. (From Rhoades RA, Tanner GA. Medical Physiology. 2nd edn. Baltimore, MD: Lippincott Williams & Wilkins, 2003.)
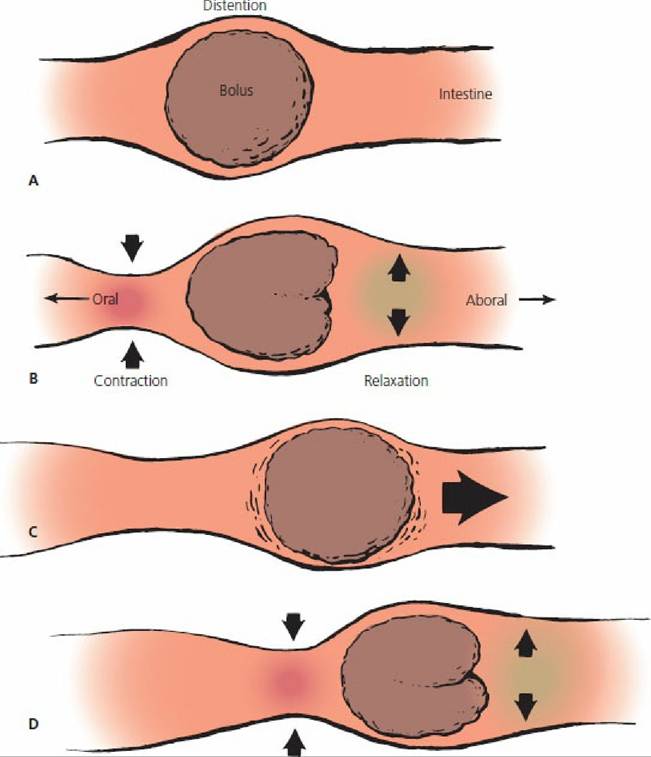
■ FIGURE 12-32 Intestinal peristalsis and movement of contents.
A. Original distention. B. Contraction occurs cranial (oral) to the distention and relaxation caudal (aboral) to the distention. C. Contraction and relaxation followed by movement of contents in an aboral direction. D. A new distention point initiates a new locus of contraction and relaxation, which continues aborally as a wave.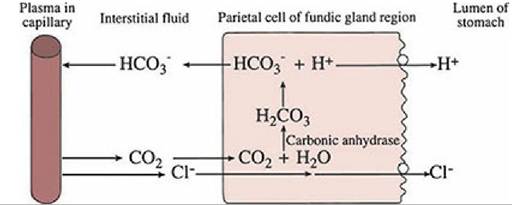
■ FIGURE 12-33 Mechanism of hydrochloric acid secretion by parietal cells of the gastric mucosa. Carbonic anhydrase facilitates the formation of H2CO3 from CO2 that diffuses into the cells from the interstitial fluid. H2CO3 dissociates into H+ and HCO3-. H+ and Cl- are actively secreted by the parietal cells into the lumen of the stomach, and this causes a gradient for diffusion of Cl- from the plasma. The loss of Cl- from plasma is followed by diffusion of HCO3- into plasma so that electrical neutrality is maintained. Accordingly, plasma bicarbonate concentration increases after ingestion of food, associated with the secretion of HCl into the lumen of the stomach.
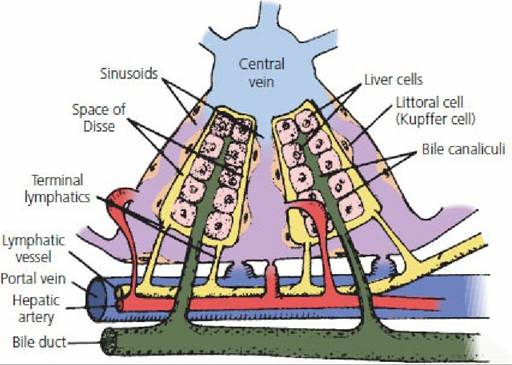
■ FIGURE 12-34 Schematic representation of the microstructure of a liver lobule and its association with bile secretion. Most of the bile salts are reabsorbed from the intestine by active transport (others are lost in feces), enter the portal vein, and pass to the liver (enterohepatic circulation). They are quickly absorbed from the sinusoids into the liver cells and are then resecreted into the bile canaliculi by active transport. The bile salts then enter the bile duct from the canaliculi. Small amounts of bile salts are secreted continuously by the liver cells, and this accounts for that which is lost in the feces. The secretion of bile by the liver is stimulated by the amount of bile salts being recirculated.
Therefore, the larger the amount recirculated, the higher the rate of bile secretion. (From Guyton AC, Taylor AE, Granger HJ. Dynamics and Control of the Body Fluids. Philadelphia, PA: WB Saunders, 1975.)Peristalsis is characterized by unidirectional, usually aboral (toward the anus) waves of contraction that are propulsive in nature. These movements are neurogenic and are carried out through local reflexes mediated through intrinsic nerve plexuses within the wall of the structure where they occur. The peristaltic reflex is initiated by distention of the bowel, which activates local reflexes and causes stimulation of activity cranial (oral towards the mouth) to and inhibition of activity caudal (aboral) to the distention. The cranial activity creates a zone of higher pressure that drives contents into the relaxed area caudal to the distention. The moving contents propagate the reflex and provide for movement of the contents aborally (Figure 12-32). There is also an extrinsic reflex for the small intestine that responds to gas distention, pain, and peritonitis, which can inhibit gastrointestinal motility.
■